

Translate this page into:
Efficiency of friction versus frictionless mechanics for correcting bimaxillary dentoalveolar protrusion in dizygotic twins – A case report


*Corresponding author: Rezeen Aziz, Department of Orthodontics and Dentofacial Orthopedics, Coorg Institute of Dental Sciences, Virajpet, Karnataka, India. rezeen.kkr32@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Aziz R, Goutham B, Somaiah S, Muddaiah S. Efficiency of friction versus frictionless mechanics for correcting bimaxillary dentoalveolar protrusion in dizygotic twins – A case report. APOS Trends Orthod. doi: 10.25259/APOS_64_2024
Abstract
The purpose of this case presentation is to determine the efficiency of two treatment mechanics in correcting clinically comparable malocclusion in dizygotic twins. The case report describes the orthodontic management of 19-year-old non-identical twins diagnosed with bimaxillary dentoalveolar protrusion on a Class I skeletal base with severe crowding using two different treatment mechanics. The first patient was treated with frictionless mechanics by making use of Kalra simultaneous intrusion and retraction arch for space closure, whereas the friction mechanics accomplished the task in the second patient with mini-implant (Titanium mini-implant, FavAnchor™ SAS, Favorite supplies, Thane west, Maharashtra, India) assisted power arm (Power hook, Azdent Orthodontics, Zhengzhou, China) retraction. It evaluated the overall treatment duration, anterior torque control, and level of comfort for the patients with the two mechanics. The post-treatment results in both cases exhibited remarkable change in inclination of upper anterior teeth which were established through cephalometric findings. Moreover, the anterior torque control was comparatively superior with loop mechanics over mini-implant assisted sliding mechanics. Both the treatment mechanics effectively and efficiently corrected the malocclusion with considerable impact on soft-tissue profile.
Keywords
Frictionless
Intrusion arch
Torque
Mini-implants
Dizygotic twins

INTRODUCTION
Bimaxillary dentoalveolar protrusion is a commonly occurring esthetic concern among adults, which leads them to seek orthodontic treatment.[1] The common treatment option in those patients is to extract the first premolars followed by retraction of anterior teeth, either using friction or frictionless mechanics with a resultant decrease in soft-tissue convexity.[2] Space closure in such a situation is more challenging if the clinician is not well-versed in the science of biomechanics; otherwise, undesirable side effects are inevitable. In friction mechanics, the amount of friction generated between brackets and the archwire interface may impede the rate of desired tooth movement. This compromises the delivery of desired force levels, causing loss of anchorage[3] and may even result in the deepening of the bite secondary to the resistance for the archwire in sliding.[4] With the advent of mini-implants as temporary anchorage devices, controlled anterior retraction is possible with minimal side effects, provided that the operator is mindful of the utilized biomechanics, whereas, in frictionless mechanics, the teeth are being moved without the brackets sliding along the archwire which nullifies the generation of friction. However, the frictionless system has the disadvantage of the complexity of loop forming and the need for precision in fabricating loops, with even minor errors in fabrication that can affect the outcome of treatment.[5] However, despite the large number of research done on investigating the superiority of different mechanics in space closure, not enough evidence was found in the literature regarding the best technique for anterior teeth retraction.[6] On the other hand, it is complicated to compare the treatment outcome or to determine the effectiveness of different treatment mechanics on different individuals since craniofacial components are greatly influenced by both genetic and environmental factors. Variations in genetic makeup and environmental influence can negatively impact our research findings. Twins’ studies provide a large benefit in comparative studies since monozygotic and dizygotic twins share part of their genetic material.[7] Hence, the authors decided to treat the twins with two different mechanics and to compare the efficiency of the respective mechanics expecting that they would have comparable biological responses during orthodontic treatment.
CASE REPORT
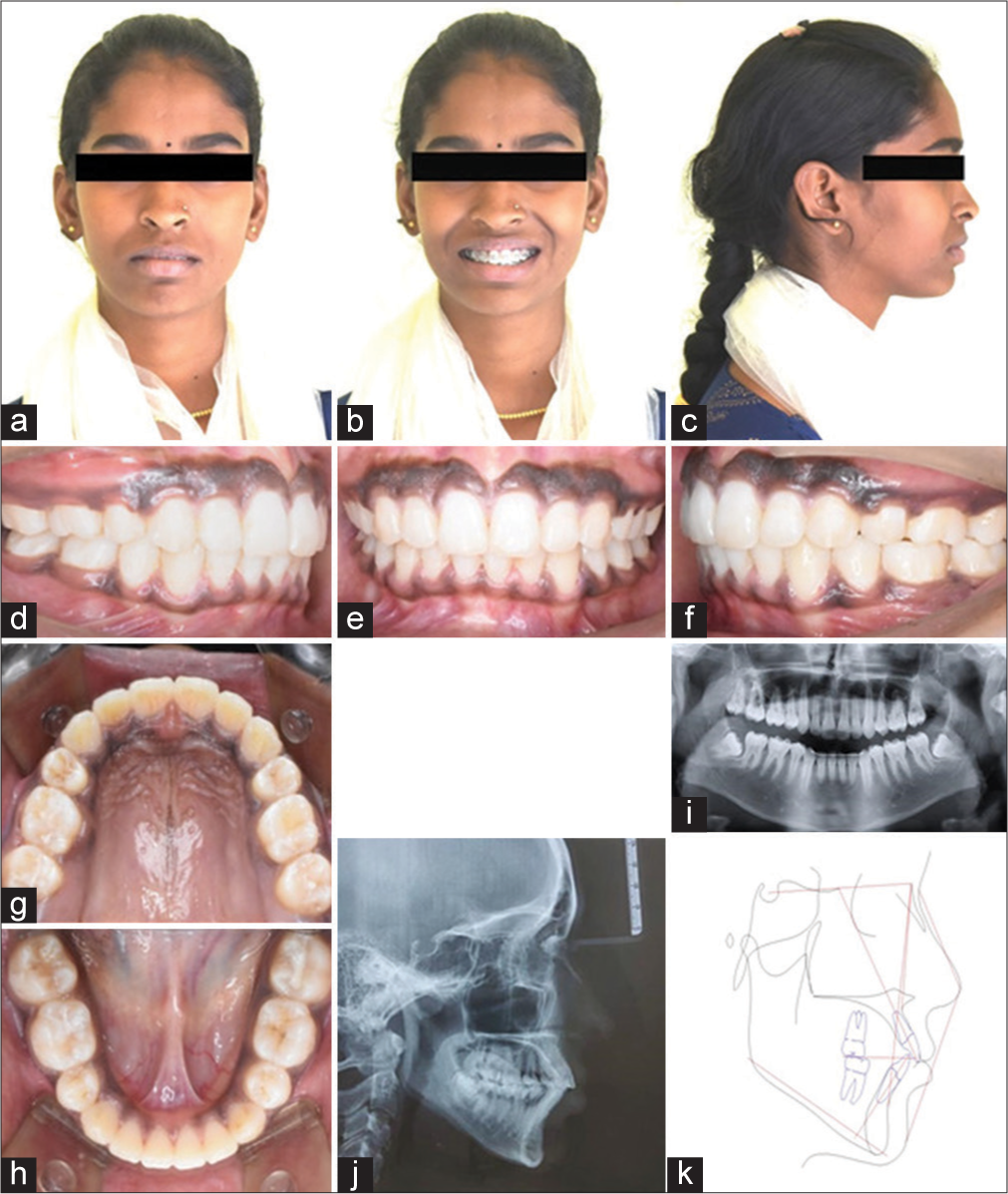
Two 19-year-old female non-identical twins of South-Asian origin reported to the Department of Orthodontics with a chief complaint of forwardly placed upper front teeth and inability to attain lip competency. On clinical examination, the authors observed Patient 1 was having Angle’s Class I malocclusion with a bimaxillary protrusion, gummy smile, increased overjet of 10 mm with severe crowding of the mandibular arch, lower dental midline shift of 3 mm toward the left, grade 3 mobility, and grade 3 gingival recession of lower left central and lateral incisors [Figure 1]. Patient 2 presented with Angle’s Class II div I malocclusion subdivision with a bimaxillary protrusion, full arch gummy smile, increased overjet of 9 mm with moderate crowding in the mandibular arch, and lower dental midline shift of 2 mm toward the right [Figure 2]. The patient also had a functional mandibular shift toward the right side in centric occlusion, resulting in an evident chin deviation without any symptoms of degenerative temporomandibular joint disorder. Apart from these features, both patients presented with other common characteristics, such as a mild convex profile, leptoproscopic facial form, medium buccal corridor, and lip incompetency. Small differences could be noted between them, as Patient 2 presented with hyperpigmented gingiva, whereas Patient 1 had a thin soft-tissue biotype lacking pigmentation. The cephalometric tracings and measurements of Patient 1 and Patient 2 demonstrated that the dental and skeletal characteristics were comparable except for molar and canine relation [Table 1].
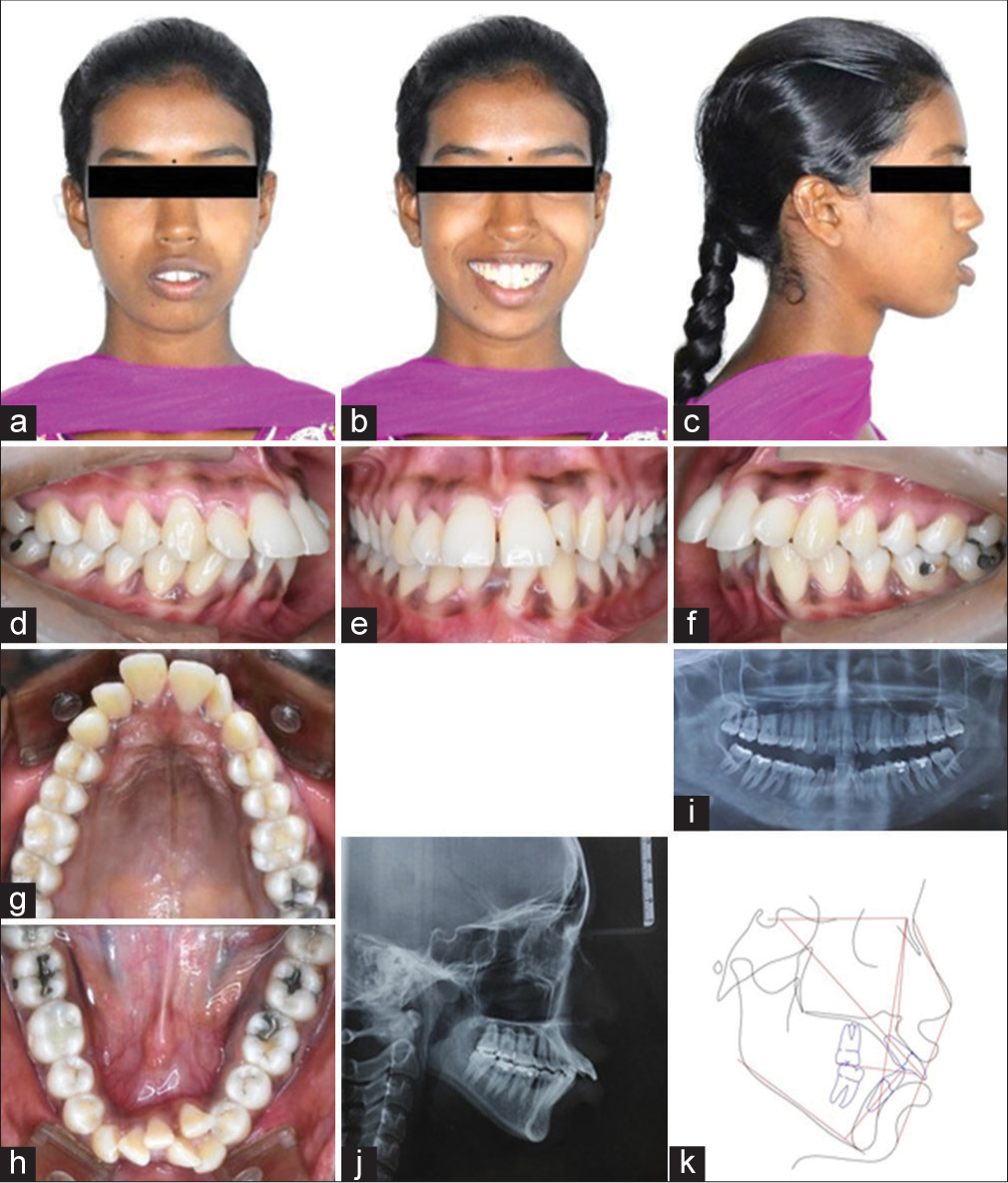
- Pre-treatment records of patient 1. a. Extra oral- Frontal, b. Extra oral - Frontal smiling, c. Extra oral - Profile, d. Intra oral - Right lateral, e. Intra oral - Frontal, f. Intra oral - Left lateral, g. Upper occlusal, h. Lower occlusal, i. Orthopantomogram (OPG), j. Lateral cephalogram, k. Ceph tracing.
| Cephalometric Variables | Mean | Patient 1 | Patient 2 | ||
|---|---|---|---|---|---|
| Pretreatment | Posttreatment | Pretreatment | Posttreatment | ||
| SNA | 82±2 | 81° | 79° | 82° | 81° |
| SNB | 80°±2° | 78° | 79° | 78° | 79° |
| ANB | 2° | 3° | 0° | 4° | 2° |
| FMA | 25° | 34° | 34° | 34° | 31° |
| INTERINCISAL ANGLE | 131° | 106° | 128° | 106° | 135° |
| U1-SN | 102° | 127° | 108° | 126° | 99° |
| U1-NA | 22°, 4 mm | 44°, 14 mm | 26°, 6 mm | 39°, 10 mm | 22°, 5 mm |
| L1-MP | 95° | 92° | 89° | 96° | 90° |
| L1-NB | 25°, 4 mm | 27°, 8 mm | 25°, 6 mm | 32°, 9 mm | 25°, 5 mm |
| NASOLABIAL ANGLE | 102±8° | 74° | 89° | 78° | 98° |
| E LINE TO U-LIP | −3 mm | 1 mm | 0 mm | 1 mm | −1 mm |
| E LINE TO L-LIP | −2 mm | 5 mm | 2 mm | 4 mm | 1 mm |
SNA - Sella-Nasion-Point A, SNB - Sella-Nasion-Point B, ANB - Point A-Nasion-Point B, FMA - Frankfort mandibular plane angle, U1-SN - Upper incisor to Sella- Nasion, U1-NA - Upper incisor to Nasion-Point A, L1-MP - Lower incisor to Mandibular plane, L1-NB - Lower incisor to Nasion-Point B
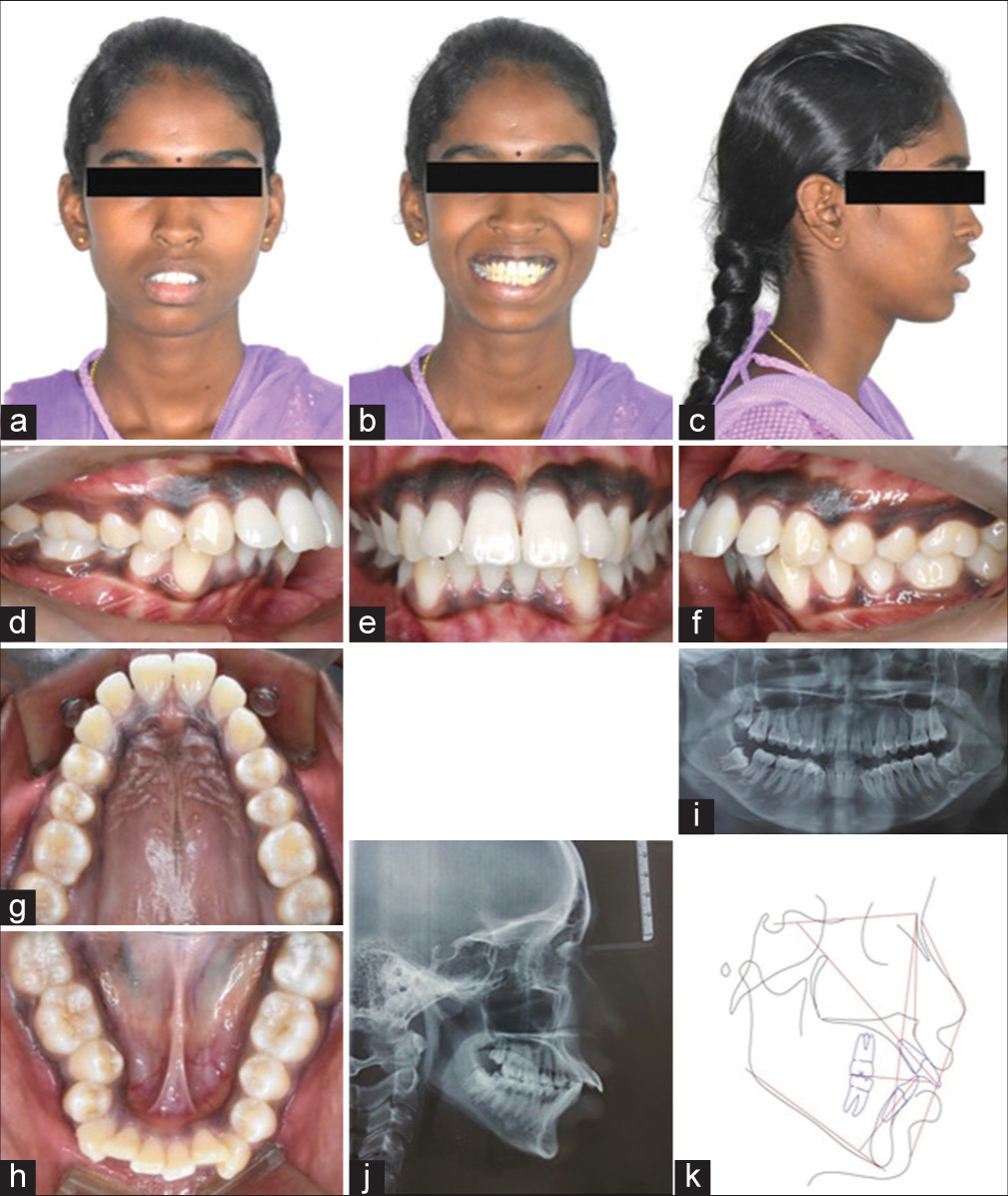
- Pre-treatment records of patient 2. a. Extra oral- Frontal, b. Extra oral - Frontal smiling, c. Extra oral - Profile, d. Intra oral - Right lateral, e. Intra oral - Frontal, f. Intra oral - Left lateral, g. Upper occlusal, h. Lower occlusal, i. Orthopantomogram (OPG), j. Lateral cephalogram, k. Ceph tracing.
TREATMENT OBJECTIVES
The treatment objectives were to (1) Achieve appropriate tooth alignment with good interdigitation; (2) reduce dental protrusion to achieve a pleasing soft-tissue profile; (3) obtain Class I molar and canine relationship; (4) achieve normal overjet and overbite; (5) coordinate midlines; and (6) correction of a gummy smile.
TREATMENT ALTERNATIVES
The treatment plans proposed for Patient 1 were: (1) to extract the upper two first premolars followed by extraction of the lower left central incisor and the lower left lateral incisor, which were periodontally compromised, and to utilize the extraction spaces in the upper arch for correcting dental proclination and lower arch for de-crowding since posterior occlusion was apparently normal. The alternative plan was: (2) to extract all four permanent first premolars and utilize the space for decrowding as well as correction of proclination. The extractions of healthy two first premolars in the lower arch were opposed due to the existing cariogenic status of the patient with multiple decayed teeth in both arches. In Patient 2, the proposed plans were as follows: (1) to extract all first premolars except in the lower right quadrant where the second premolar was decided to extract to facilitate easy molar protraction to attain Class I molar relationship. The alternative plan was: (2) to extract the lower first left premolar and lower right second premolar to level and align the arch, followed by extraction of the upper first premolars to surgically set back the maxilla through anterior maxillary osteotomy at the end of leveling and alignment. However, Patient 2 accepted the first non-surgical treatment plan. The presence of a gummy smile in Patient 2 was also decided to be addressed by making use of mini-implant assisted power arm retraction guided through the center of resistance of dentition, which would not further extrude the maxillary anterior while retraction.
TREATMENT PROGRESS
Patient 1 was treated with a conventional pre-adjusted edgewise appliance of “0.022 × 0.028” slot, Roth prescription (Mini 2000, Ormco Corp. Glendora, CA). The initial leveling and aligning were performed in a segmental approach with an archwire sequence comprising “0.012,” “0.014,” “0.016,” “0.017 × 0.025,” “0.019 × 0.025” HANT (Tinol-2, Modern Orthodontics, Ludhiana, India) wires, and “0.019 × 0.025” SS wire. The posterior segment was stabilized using “0.019 × 0.025” SS segmental base archwire, and the transverse anchorage was augmented through a transpalatal arch made of 0.8 mm stainless steel round wire. At the end of 6 months, both the arches were well aligned and leveled. The space closure was accomplished with frictionless mechanics using Kalra simultaneous intrusion and retraction arch (K-SIR arch)[8] made of “0.019 × 0.025” TMA archwire in the upper arch and in the lower arch, the remaining anterior space was closed using a keyhole loop [Figure 3]. The K-SIR arch was activated 3 mm every 60 days and the subsequent appointments were used for finishing the occlusion.
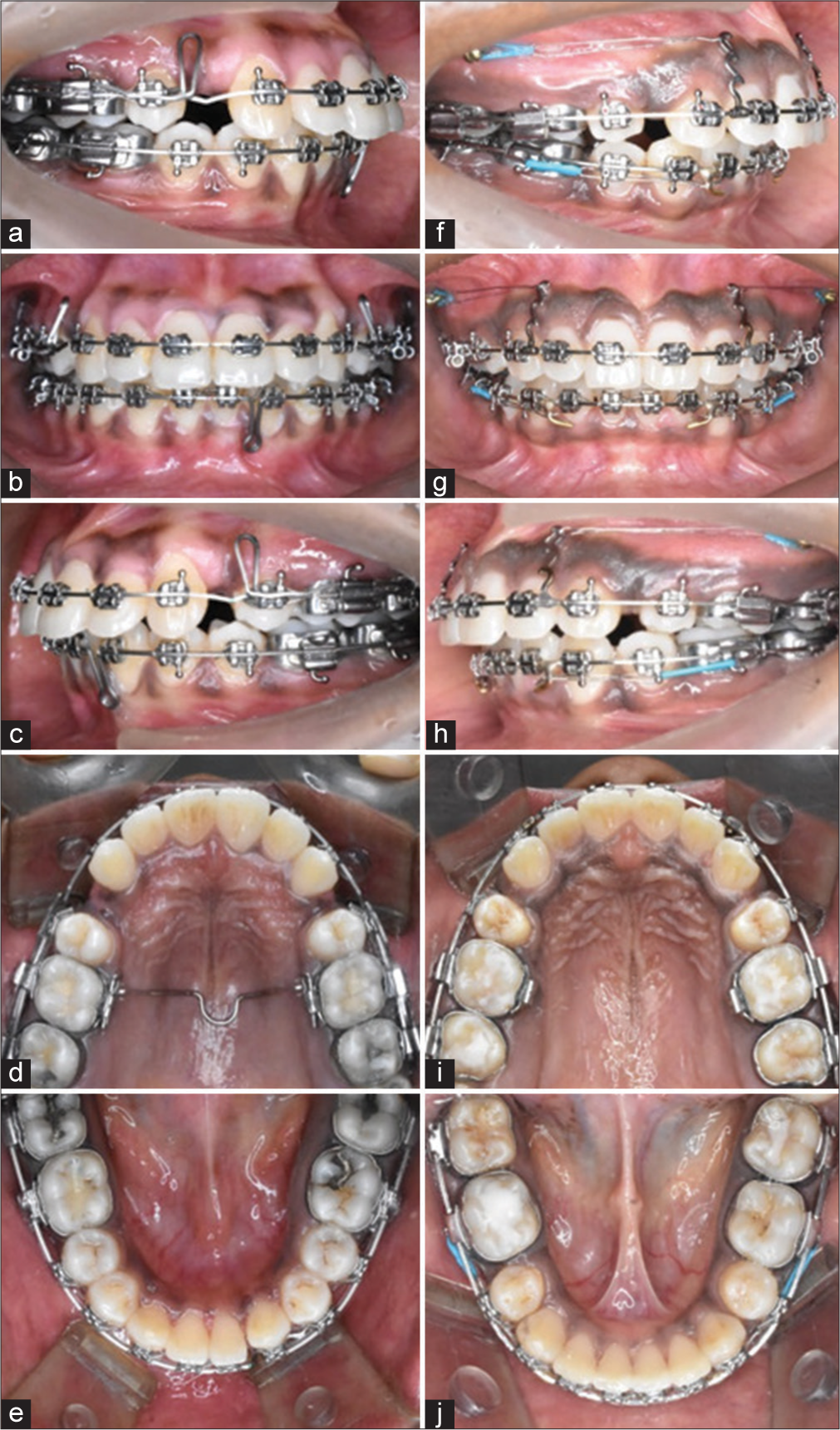
- Space closure mechanics: Kalra simultaneous intrusion and retraction arch retraction in patient 1 (left), Implant-supported power arm retraction in patient 2 (right). a. Extra oral- Frontal, b. Extra oral - Frontal smiling, c. Extra oral - Profile, d. Intra oral - Right lateral, e. Intra oral - Frontal, f. Intra oral - Left lateral, g. Upper occlusal, h. Lower occlusal, i. OPG, j. Lateral cephalogram, k. Ceph tracing.
In Patient 2, a conventional Pre-adjusted edgewise appliance of “0.022 × 0.028” slot, MBT prescription (Mini 2000, Ormco Corp. Glendora, CA) was used. The archwire sequence used for initial leveling and aligning was “0.012,” “0.014,” “0.016,” “0.017 × 0.025,” “0.019 × 0.025” HANT (Tinol-2, Modern Orthodontics, Ludhiana, India) wires, and “0.019 × 0.025” SS. The friction mechanics were chosen to treat this patient, contrary to Patient 1. The anterior retraction was done on “0.019 × 0.025” SS archwire in both arches with two power arms (Power hook, Azdent Orthodontics, Zhengzhou, China) of 8 mm height crimped onto the archwire in the upper arch between the lateral incisor and canine bracket to prevent bite deepening while retraction. The anchorage was taken from two mini-implants of dimension 1.4 mm × 8mm (Titanium mini-implant, Color code: Golden, FavAnchor™ SAS, Favorite supplies, Thane West, Maharashtra, India) placed between the roots of maxillary first and second molars at the level of the mucogingival junction [Figure 3]. The retraction force of 150 g per side was given to the power hooks parallel to the upper archwire using conventional tie-backs. In the lower arch, the minimal space left over after alignment was closed using conventional tie-backs engaged to the anterior soldered hooks, with first molars as anchor units.
TREATMENT RESULTS
At the end of comprehensive orthodontic treatment, the authors achieved good posterior occlusion with interdigitation, bilateral Class I molar and canine relationship, ideal overjet and overbite with lip competency, and agreeable soft-tissue profile in both Patient 1 [Figure 4] and Patient 2 [Figure 5]. Subsequently, the overall treatment duration, anterior torque control, and level of comfort for the patients with the two mechanics were assessed. The authors considered only the upper arch for comparison of all the parameters since the extraction pattern was different in the lower arch for both patients. The level of comfort was evaluated through a subjective measuring scale to assess pain perception using the Universal Pain Assessment tool (UPAT). The overall treatment duration for friction and frictionless mechanics extended for a period of 18 and 15 months, respectively. In Patient 1, the initial leveling and aligning took 6 months to complete in segmental mode, whereas in Patient 2, this stage lasted for 8 months. Patient 2 also reported an increased amount of pain and discomfort during this period, with a corresponding score of 5 on the UPAT subjective scale against a score of 2 by Patient 1 in UPAT [Figure 6]. The treatment duration in space closure for both patients lasted for 6 months with a significant variation in the rate of retraction [Figure 7]. In frictionless mechanics, space closure took place at the rate of 0.9 mm per month, contrary to 0.6 mm per month for friction mechanics. Patient 1 reported moderate pain and difficulty in tolerating the appliance during the space closure stage due to loops abutting the cheek mucosa. The final finishing and detailing lasted for 3 months in Patient 1 and 4 months in Patient 2.
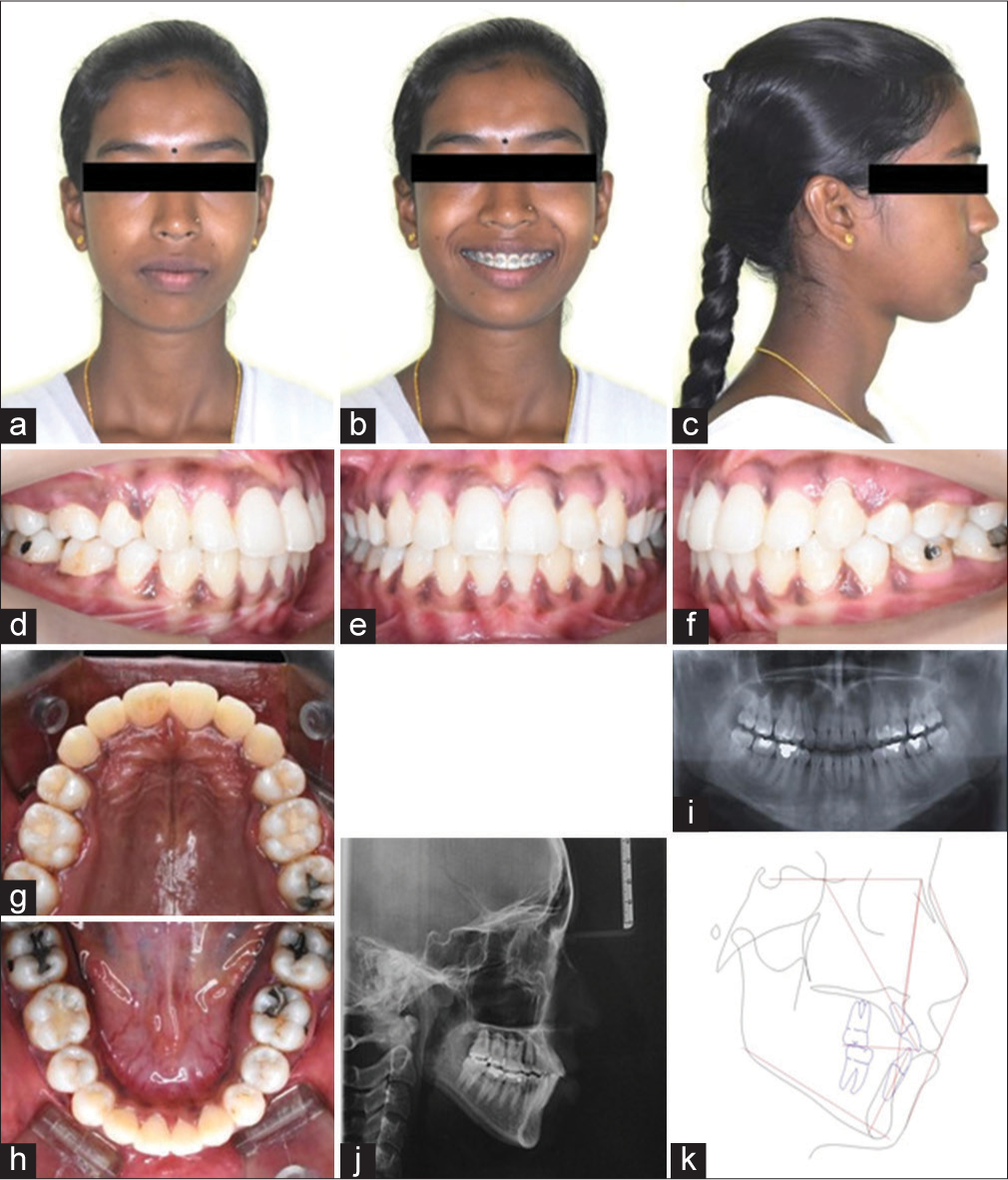
- (a-k) Post-treatment records of Patient 1.
- Post-treatment records of Patient 2. a. Extra oral- Frontal, b. Extra oral - Frontal smiling, c. Extra oral - Profile, d. Intra oral - Right lateral, e. Intra oral - Frontal, f. Intra oral - Left lateral, g. Upper occlusal, h. Lower occlusal, i. Orthopantomogram (OPG), j. Lateral cephalogram, k. Ceph tracing.
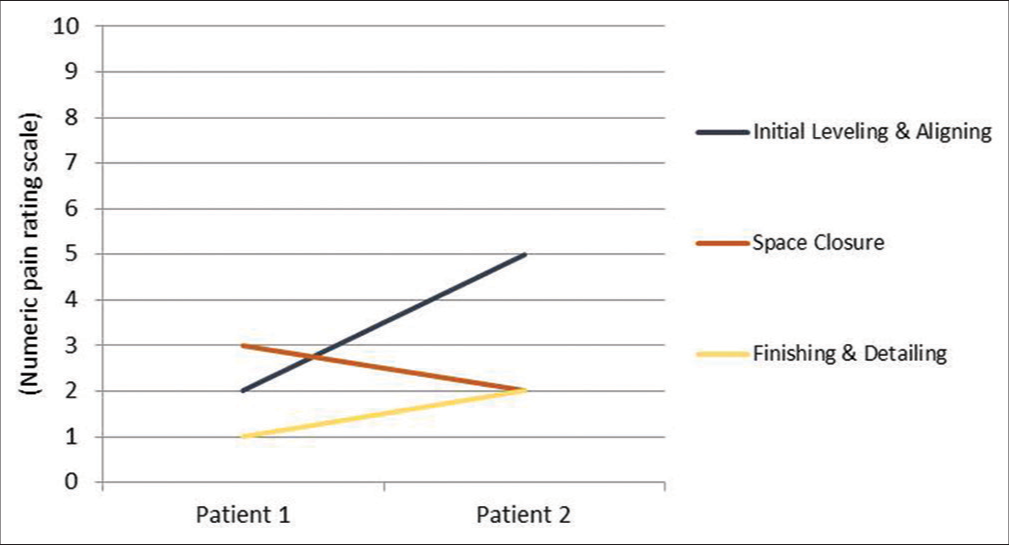
- Graphical representation of pain perception.
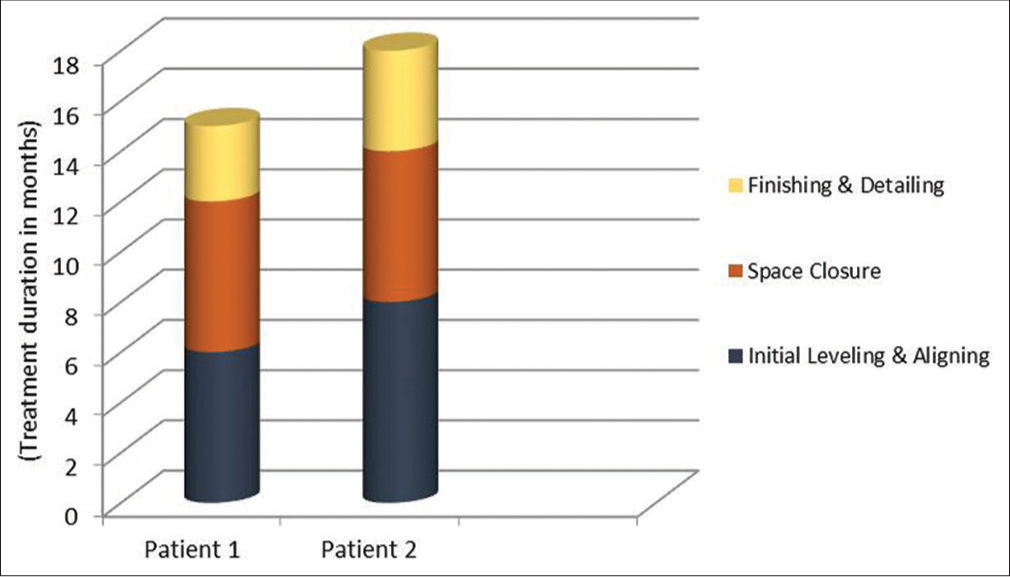
- Graphical representation of treatment duration.
To determine the amount of maxillary anterior torque loss, the authors described a novel method using cephalometric tracing of the maxilla and upper incisor [Figure 8]. It made use of the palatal plane connecting ANS-PNS and the long axis of the upper incisor as the reference planes. A perpendicular is dropped down from the palatal plane, passing through the midpoint of the cementoenamel junction, named the “Mc” point. The linear root position is measured horizontally from the root apex to the perpendicular line, named “linear torque,” depicted as “Phi” (f), and root inclination is measured between the long axis of the upper incisor to the perpendicular line, namely “angular torque,” depicted as “Theta” (θ). This method is more predictable since no skeletal landmark that may get affected by anterior teeth movement is considered as a reference point. To evaluate the amount of torque loss, the linear and angular torque values, along with overbite, were compared before and after retraction on lateral cephalometric tracing [Table 2]. In Patient 1, angular torque decreased from 35° to 28° and linear torque from 10 mm to 8 mm, suggesting torque loss or labial root movement while retraction. In contrast, Patient 2 exhibited a significant post-treatment change in both angular and linear torque from pretreatment values of 33–18° and 9 mm–3 mm, respectively, indicating severe torque loss compared to Patient 1. In terms of overbite, Patient 2 experienced increased bite deepening following retraction compared to Patient 1. All other skeletal and dental cephalometric parameters revealed significant positive changes in the post-treatment cephalometric values [Table 1] and superimpositions [Figures 9 and 10].
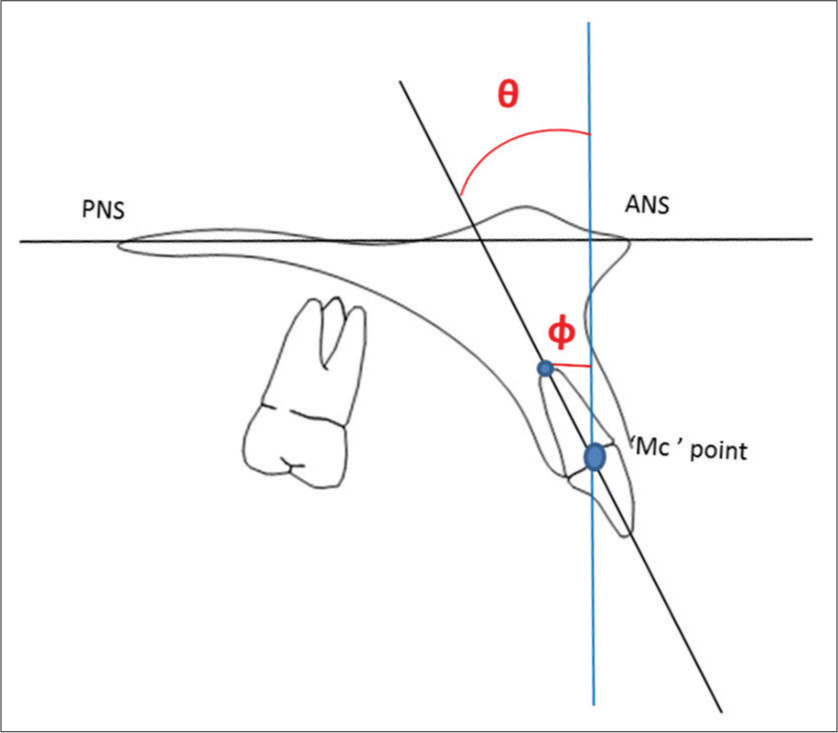
- A novel method to determine maxillary incisor torque. ANS: Anterior nasal spine, PNS: Posterior nasal spine, ‘Mc’ point: Midpoint of cementoenamel junction
| Cephalometric variables | Patient 1 | Patient 2 | ||
|---|---|---|---|---|
| Pre-treatment | Post-treatment | Pre-treatment | Post-treatment | |
| Angular torque (θ) | 35° | 28° | 33° | 19° |
| Linear torque (φ) | 10 mm | 6 mm | 9 mm | 3 mm |
| Overbite | 3 mm | 2 mm | 3 mm | 4 mm |
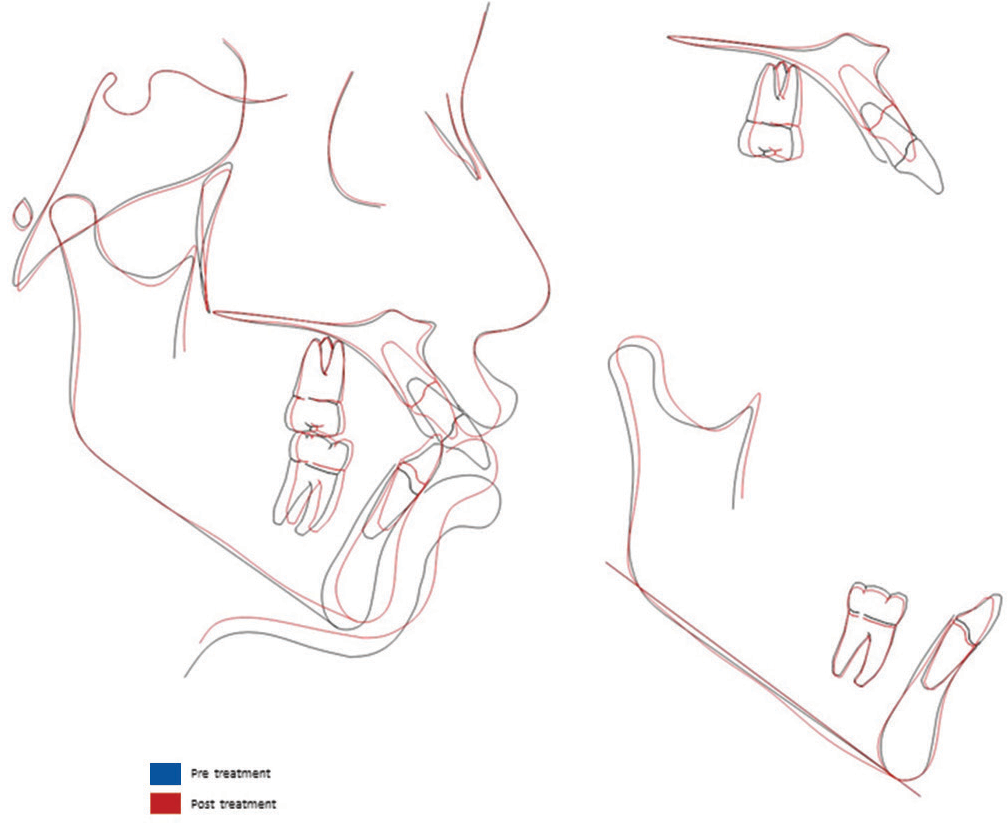
- Superimposition of pre-treatment and post-treatment lateral cephalogram of Patient 1.
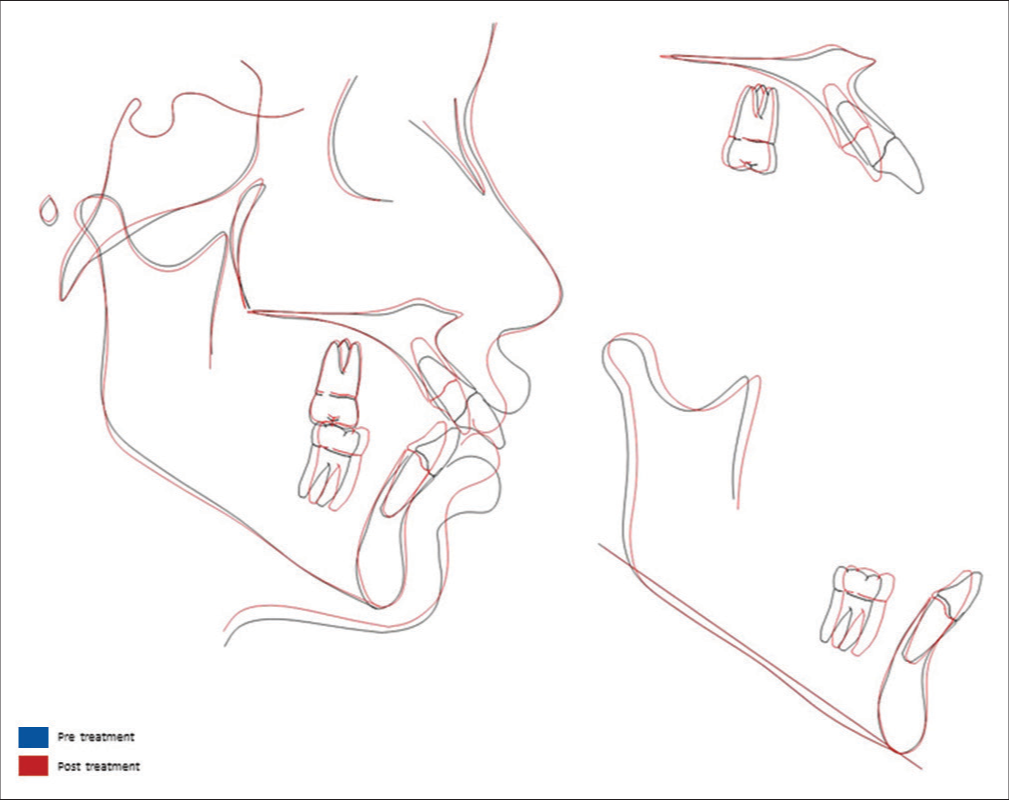
- Superimposition of pre-treatment and post-treatment lateral cephalogram of Patient 2.
DISCUSSION
Orthodontic treatment is a time-consuming procedure, and so, it is always a primary concern for every patient to know how fast the treatment can be completed. While comparing the treatment results, the authors appreciated that the time taken for initial leveling and aligning in frictionless mechanics was marginally faster. In terms of space closure, both mechanics continued for 6 months, exhibiting an atypical rate of retraction, with frictionless mechanics being superior to friction mechanics. Few studies reported a marginally faster, yet not significantly different, rate of incisor retraction when frictionless mechanics were implemented compared to friction mechanics, which is consistent with our results.[9,10] Contrary to the above findings, Rhee et al.[5] did not find any superiority of either mechanic over the other for canine retraction using a typodont simulation system. The activation of loops in frictionless mechanics was spaced every 60 days, while tie-back activation in friction mechanics was carried out every 30 days since the force levels in elastic modules degrade within a short period.[11] The frictionless mechanics dominated friction mechanics in terms of overall treatment duration, with a completion period of 15 months in 13 appointments and 18 months in 18 appointments, respectively.
The anterior torque control while space closure is a difficult task to accomplish even though there are various methods available to overcome the side effects like uncontrolled tipping of anterior teeth during retraction.[12] The efficiency of the method selected solely depends on the clinician’s skill and individual experience. The comparison of the amount of torque loss resulting during anterior teeth retraction can help to assess the efficiency of the selected method. In frictionless mechanics, the difference between angular and linear torque values was comparatively less compared to the friction mechanics, demonstrating better torque control of the K-SIR arch [Table 2]. The root apex in Patient 2 moved labial by 6 mm, losing 15° of root inclination, resulting in torque loss. This finding was consistent with the reports of Tominaga et al.[13] who pointed out that the use of power arms alone cannot control bodily movement or root movement of the incisors, which was further established by Hamanaka et al.[14] through a finite element study, whereas, in Patient 1, root inclination was maintained with minimal loss of torque by 6° compared to the pre-retraction stage, and 2 mm of labial root movement establishing the moment-to-force ratio generated by the K-SIR arch was relatively higher than the power arms, to maintain torque of anterior teeth. The study by Goyal et al.[15] and Sardana et al.[16] revealed that retraction using sliding mechanics resulted in a significant reduction in the proclamation of upper anterior compared to loop mechanics, suggesting superior torque control with loops. Furthermore, in terms of an overbite, there was a significant bite deepening noticed after space closure in friction mechanics, even after using mini implant-assisted power arm retraction. Another study reported similar findings suggesting that the use of miniscrews cannot prevent anterior torque loss nor the bowing effect during space closure.[17]
The level of comfort was correlated with the pain experienced by the patients during orthodontic treatment. The UPAT was preferred by the authors because patients can compare a numerical rating or facial expression with the activity tolerance scale that coincides with the level of pain perceived by the individual, which is not possible to assess with basic methods like the visual analog scale. It was found that pain perception was comparatively less, with frictionless mechanics getting an average score of 2 on the numeric pain rating scale, whereas Patient 2 gave an average score of 3 for friction mechanics. Patient 2 related an increased amount of pain in the initial leveling and alignment stage, which interfered with her concentration and to perform day-to-day activities. This finding corresponded with the results reported by Ertan Erdinç and Dinçer[18] and Polat et al.[19] proving pain perception appeared approximately 2–3 h after orthodontic appliance placement. It reduced its intensity after 72 h with a high degree of inter and intra-individual variation. In contrast, Patient 1 experienced minimal pain during initial leveling and alignment but experienced moderate pain and difficulty in tolerating the appliance during the space closure stage because the loops were abutting the cheek mucosa. Hence, it can be concluded that the pain experienced by patients does not seem to be directly related to the magnitude of the force exerted but relies heavily on the psychological well-being of the individual.[20,21]
CONCLUSION
Both the cases presented here have been well treated by the selected biomechanics even though there were comparable differences noted in the time taken to finish the treatment, anterior torque control, and comfort level of the patients.
In the presented cases, loop mechanics was superior to mini-implant-assisted sliding mechanics in controlling anterior torque, rapidness of finishing treatment, and patient comfort. More research is essential to conclude which system has biomechanical advantages since the current literature does not provide high-quality evidence.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Bimaxillary dentoalveolar protrusion: Traits and orthodontic correction. Angle Orthod. 2005;75:333-9.
- [Google Scholar]
- Analysis of maxillary arch force/couple systems for a simulated high canine malocclusion: Part 1. Passive ligation. Angle Orthod. 2011;81:953-9.
- [CrossRef] [PubMed] [Google Scholar]
- Understanding the basis of space closure in orthodontics for a more efficient orthodontic treatment. Dent Press J Orthod. 2016;21:115-25.
- [CrossRef] [PubMed] [Google Scholar]
- A comparison between friction and frictionless mechanics with a new typodont simulation system. Am J Orthod Dentofacial Orthop. 2001;119:292-9.
- [CrossRef] [PubMed] [Google Scholar]
- Canine retraction: A systematic review of different methods used. J Orthod Sci. 2015;4:1-8.
- [CrossRef] [PubMed] [Google Scholar]
- Phenotypic differences in genetically identical organisms: the epigenetic perspective. Hum Mol Genet. 2005;14(Spec No 1):R11-8.
- [CrossRef] [PubMed] [Google Scholar]
- Simultaneous intrusion and retraction of the anterior teeth. J Clin Orthod. 1998;32:535-40.
- [Google Scholar]
- The retraction of upper incisors with the PG retraction system. Eur J Orthod. 2000;22:33-41.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of the rate of anterior segment retraction in orthodontic patients with bimaxillary protrusion using friction vs frictionless mechanics: A single-center, single-blind randomized clinical trial. Angle Orthod. 2022;92:738-45.
- [CrossRef] [PubMed] [Google Scholar]
- In vitro assessment of the mechanical properties of latex and non-latex orthodontic elastics. Am J Orthod Dentofacial Orthop. 2001;120:36-44.
- [CrossRef] [PubMed] [Google Scholar]
- Methods of anterior torque control during retraction: A systematic review. Diagnostics (Basel). 2022;12:1611.
- [CrossRef] [PubMed] [Google Scholar]
- Optimal loading conditions for controlled movement of anterior teeth in sliding mechanics. Angle Orthod. 2010;69:129-30.
- [CrossRef] [Google Scholar]
- Numeric simulation model for long-term orthodontic tooth movement with contact boundary conditions using the finite element method. Am J Orthod Dentofacial Orthop. 2017;152:601-12.
- [CrossRef] [PubMed] [Google Scholar]
- To evaluate and compare the rate of space closure and incisor retraction between sliding mechanics and CNA mushroom loop archwire using indirect anchorage. J Contemp Orthod. 2019;3:13-8.
- [CrossRef] [Google Scholar]
- Rate and anchorage loss during en-masse retraction between friction and frictionless mechanics: A randomized clinical trial. Orthod Craniofac Res. 2023;26:598-607.
- [CrossRef] [PubMed] [Google Scholar]
- Biomechanical considerations in treatment with miniscrew anchorage: Part-I: The sagittal plane. J Clin Orthod. 2008;42:79-83.
- [Google Scholar]
- Perception of pain during orthodontic treatment with fixed appliances. Eur J Orthod. 2004;26:79-85.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of preoperative ibuprofen and naproxen sodium on orthodontic pain. Angle Orthod. 2005;75:791-6.
- [Google Scholar]
- Pain in orthodontics: A review and discussion of the literature. J Orofacial Orthop. 2000;61:125-37.
- [CrossRef] [PubMed] [Google Scholar]
- Pain and discomfort during orthodontic treatment: Causative factors and effects on compliance. Am J Orthod Dentofacial Orthop. 1998;114:684-91.
- [CrossRef] [PubMed] [Google Scholar]




