

Translate this page into:
Evaluation of a correlation between the severity of root resorption of adjacent teeth and level of difficulty of impacted canine – A cone-beam computed tomography study

*Corresponding author: Adnan Sarfaraz Khan, Department of Orthodontics and Dentofacial Orthopedics, Dr. D. Y. Patil Dental College and Hospital, Pimpri, Pune, Dr. D. Y. Patil Vidyapeeth DPU, Maharashtra, India. adnan.khan94@hotmail.com
-
Received: ,
Accepted: ,
How to cite this article: Chhutani PD, Deshmukh SV, Khan AS, Rahalkar JS. Evaluation of a correlation between the severity of root resorption of adjacent teeth and level of difficulty of impacted canine – A cone-beam computed tomography study. APOS Trends Orthod 2023;13:230-9.
Abstract
Objectives:
An interrelation between the level of difficulty of canine impaction based on its three-dimensional position and the degree of root resorption of the adjacent teeth improves the quality of orthodontic treatment planning. It would be advantageous for clinicians to know the predilection of resorption in varying canine positions. The aim of the study is to evaluate and correlate the severity of root resorption of adjacent teeth and the level of difficulty of impacted canine classified by KPG Index and sector analysis using cone-beam computed tomography.
Material and Methods:
The study sample comprised 48 impacted canines in orthodontic patients (17 boys and 27 girls) with a mean age of 24 years. The cone-beam computed tomographs were evaluated using Dolphin Imaging Software and primarily, three observations were recorded: KPG index, sector analysis, and root resorption. The samples were equally divided into four groups based on the KPG index, with 12 samples in each group. Additionally, the inclination of the canine in the frontal plane and their degree of vertical eruption were recorded.
Results:
The number and severity of resorptive lesions increased as the KPG score escalated. The mean KPG score was 13.67 ± 6.336 and the average KPG index was 2.5 ± 1.13. A statistically significant positive correlation was found between all the parameters and root resorption.
Conclusion:
A positive correlation exists between the level of difficulty of canine impaction and root resorption of the adjacent teeth. A KPG score higher than 13.67 can be a resourceful predictor of resorptive lesions. An increased tendency of root resorption of the neighboring teeth was observed when angle α and angle β exceed 43.71° and 43.26°, respectively.
Keywords
Impaction
Canine
Impacted canine
Difficulty
Root resorption
Severity
KPG index
Sector analysis
Cone-beam computed tomography

INTRODUCTION
The permanent maxillary canine is the second most frequent tooth to be impacted, following the third molar. Its prevalence accounts up to 2% in the general population.[1] About 85% of the maxillary impacted canines are located palatally; as opposed to 15% that are buccally positioned.[2] Although, buccally positioned canines are not a rare finding. It is found that females are more likely to present with maxillary canine impactions, with a gender predilection ratio of 2:1.[3] Patients having impacted canines often undergo prolonged orthodontic treatment contingent on its level of difficulty and distance from the ideal occlusal plane.
There are several etiological factors associated with the occurrence of impaction. The authors suggest two theoretical explanations for their complex etiology. (1) Genetic theory. (2) Guidance theory. The former illustrates the role of genes in several dentofacial anomalies, among which the impaction of canines is a significant feature. The guidance theory stresses on the role of the lateral incisor, that is, its genesis, size, and shape in guiding the canine tooth into its ideal position.[4] Nevertheless, regardless of the causal factor, early detection, and accurate diagnosis of impacted canines is mandatory for proper treatment planning. Unattended impacted canines could lead to their ankylosis, further complicating the treatment scenario and prolonging treatment time. Orthodontic-surgical management of maxillary impacted canines has evolved as a tedious challenge faced in clinical practice due to its intricate position within the bone. The efficient localization of such teeth is the first step of every treatment protocol and is of paramount importance.
Among the various complications that impacted canines bring, resorption of the adjacent teeth is seen occasionally.[5] This resorption is commonly induced by the neighboring impacted canines.[6-9] The definite etiology of this phenomenon is unknown; however, it is believed that the pressure-provoking factor by the maxillary canine could be responsible for inducing resorption of the roots of the adjacent teeth.[6] It has been deciphered that a well-developed dentition, a more medially located canine in the dental arch, or one with a horizontal path of eruption are primary predisposing factors for incisor resorption.[10] The spatial relationships between the cusp tip of the impacted canine have been found to influence the severity of root resorption seen in the adjacent maxillary teeth, most predominantly the lateral incisor.[10] Depending on the extent of the resorption, the treatment modalities vary and may involve endodontic treatment or extraction which significantly modulates the orthodontic treatment plan.
Resorptive lesions are often overlooked on intraoral periapical radiographs and orthopantomograms due to the two- dimensional representation of overlapping structures. This necessitates the use of an X-ray imaging system that generates three-dimensional (3D) images to allow better visualization of dentofacial structures. With the advent of cone-beam computed tomography (CBCT), the impacted teeth can be visualized in all three planes and their spatial relationships with the adjacent structures. Three-dimensional imaging is a boon in clinical orthodontics and helps clinicians tackle challenging malocclusions by expanding diagnostic horizons and improvising judgment in treatment planning.[6,11,12] These resorptive lesions are clearly visualized with the use of computed tomography which eliminates magnification and blurring errors, thereby ensuring precision in diagnosis.
This study revolves around both- 3D and 2D representations of canine orientation by means of KPG index and sector analysis respectively, and aims to correlate them with the incidence of resorption of the adjacent teeth.[10,13]
Ericson and Kurol have suggested a thorough clinical and radiographic examination at an early stage, that is, when the normalcy of the eruption pattern of the cuspids is found questionable. It is evident that the orthodontic treatment plan depends on the status of vitality of the adjacent maxillary teeth.[6,7] To further enhance the expertise by which the treatment can be planned, it would be advantageous for clinicians to know the predilection for resorption in varying canine positions.
Hence, deriving an interrelation between the levels of difficulty of the canine impaction based on its 3D position and the degree of root resorption of adjacent teeth could benefit the orthodontic-surgical team to modulate the management of impaction cases.
The KPG index is a reliable research tool and is essentially a composite measure that aggregates and compiles the level of difficulty of canine impaction in all three planes of space.[13] Although there are limited studies on it, the validity of the KPG Index has been documented.[14]
There is a substantial amount of literature that puts light on the effect of canine impaction on the roots of the adjacent teeth. However, no study compares the extent of root resorption with a quantitative index that summarizes the canine’s 3D position, thus necessitating documentation.
Therefore, the aim of the study was to evaluate and correlate the severity of root resorption of adjacent teeth and the level of difficulty of impacted canine classified by KPG Index and sector analysis using CBCT.
MATERIAL AND METHODS
This study was carried out to assess the potential risk of root resorption inflicted by impacted canines. The inclusion criteria involved participants having unilateral or bilateral impacted maxillary canines, participants having buccally or palatally positioned impacted canines, participants aged above 12 years and participants who had not undergone any prior orthodontic treatment. Participants with craniofacial anomalies were excluded from the study.
Convenience sampling technique was used to select the sample size and the following formula was used:
n = ([za + zβ]c)2 + 3
Zα = 1.96
Zβ = 0.84
c = 0.5 × In([1 + α]/[1 - α]) = 0.424
The sample size determined by the aforementioned formula was 48 impacted canines.
All patients reporting to the department of orthodontics and dentofacial orthopedics fitting the inclusion criteria were added to the study.
Waiver of consent was obtained and ethical clearance was given by the institution’s Research and Recognition Committee (Ref: DPU/R&R(D)/112(23)/18).
Four patients displayed bilateral impacted maxillary canines whereas 40 patients displayed unilateral impacted maxillary canines, thus adding up to a sample of 48 impacted canines. In essence, 44 CBCT scans of subjects (17 boys, 27 girls) ranging between ages 13 years and 35 years, with a mean age of 24 years were included. The iCAT FLX V17 machine was used to obtain the CBCTs of all the patients. The V17 machine had a maximum and scalable FOV of up to 23 cm × 17 cm.
Dolphin Imaging Software (11.8 Premium Version) was utilized to view the DICOM files and to calculate measurements.
On examination of the samples, 32 impacted canines were positioned palatally and 16 were positioned buccally. Primarily, three observations were recorded: KPG index, sector analysis, and root resorption. The KPG index is the first index to represent the difficulty of canine impaction by evaluating its 3D position using CBCT [Figures 1-5]. This index assists in standardizing orthodontic diagnosis by predicting treatment difficulty.[13] Each impacted canine was meticulously examined to allocate 2 scores to its crown and root tips in each dimension of space-horizontal, vertical, and axial. The final KPG score for an impacted tooth is the sum of all 6 scores obtained. The final KPG score depends on the degree of deviation of the position of the ectopically erupting cuspid in each dimension. [Table 1] shows the scoring system used for the categorization of the level of difficulty of impacted canines by Kau et al.,[13,15] The sample was equally divided into four groups based upon the KPG index, as postulated by the original authors: Group I: Easy, Group II: Moderate, Group III: Difficult, and Group IV: Extreme, with 12 samples falling into each group.

- Method of evaluating the level of difficulty of impacted canine on X-axis.

- Method of evaluating the level of difficulty of impacted canine on Y-axis – Cusp Tip.

- Method of evaluating the level of difficulty of impacted canine on Y-axis – Root Tip.

- Method of evaluating the level of difficulty of impacted canine on Z-axis.

- Illustration of the method used in this study for evaluating the level of difficulty of impacted canine on Z-axis.
| Leave of difficulty | Modified KPG Index |
|---|---|
| Easy | 0–-7 |
| Moderate | 7–14 |
| Difficult | 15-19 |
| Extreme | 20 and above |
Furthermore, orthopantomograms were generated from the CBCTs to study the sector in which the impacted canine was present as postulated by Lindauer et al.[16] The inclination of the canine in frontal plane was examined by 2 angular measurements, that is: Angle α which is the angle of eruption path to the midline and Angle β which is the angle of eruption path to the long axis of the lateral incisor [Figures 6-12]. The degree of vertical eruption of the impacted canines was examined by 2 linear measurements, that is: d1 which is the distance between the cusp tip and occlusal plane as seen in the panoramic view and d2 which is the distance between the cusp tip and occlusal plane as seen in the lateral view [Figures 13 and 14].[6]

- Method of evaluating the level of canine impaction by sector analysis.

- Figure illustrating impacted canines in Sector 1.

- Figure illustrating impacted canines in Sector 2.

- Figure illustrating impacted canines in Sector 3.

- Figure illustrating impacted canines in Sector 4.

- Figure illustrating measurement of inclination of impacted canine in the Frontal Plane.

- Figure illustrating measurement of inclination of impacted canine in the Frontal Plane showing α and β angles.
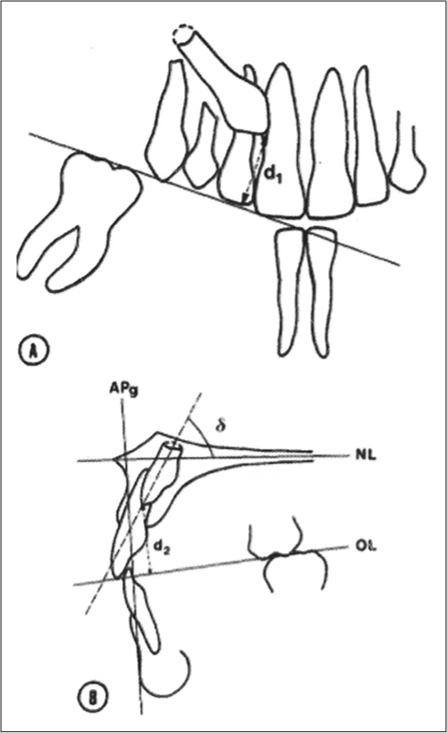
- Figure illustrating measurement of degree of vertical eruption of impacted canine in the Frontal Plane.

- Figure illustrating measurement of degree of vertical eruption of impacted canine in the Frontal Plane showing d1 and d2.
Ericson and Kurol’s classification of degree of root resorption was used to determine the extent of resorption seen in the adjacent teeth, most commonly the central incisor, lateral incisor and the first premolar [Figure 15].[9] A score was designated to the lesion, if present, according to the proposed classification in each group. To determine the reliability and repeatability of this method, measurements were taken thrice by the same person at a time interval of 3 days. These measurements were repeated again after a duration of 30 days. To further confirm the consistency between the sets of readings, the mean was calculated. The collected data were then analyzed and inferences were made.

- (a) Figure illustrating root resorption of the adjacent teeth caused by the impacted canine, (b) figure illustrating root resorption of the adjacent teeth caused by the impacted canine.
Statistical analysis
The statistical analysis was carried out using the SPSS software (version 19.0, SPSS for Windows, Version 19; SPSS Inc. Chicago, IL, USA). Each parameter’s arithmetic mean and standard deviation were calculated. The Spearman correlation test was used to evaluate the correlation between each of the test variables with the grade of root resorption. The level of significance was P > 0.01. P < 0.01 was considered significant. Multiple linear regression analysis was applied and the model summary was derived. The model fit obtained was 0.692, with R2 and adjusted R2 values equal to 0.479 and 0.400, respectively (F = 6.120, P < 0.001). This relation was found to be statistically significant.
RESULTS
The occurrence of root resorption was directly proportional to an increasing KPG score. Our study reflected 5, 7, and 9 resorptive lesions in the roots of the adjacent teeth in Group II, Group III, and Group IV, respectively. The Spearman’s correlation coefficient test was applied to analyze the statistical correlation between each of the test parameters with the grade of root resorption. [Table 2] shows the correlation between the KPG index and the grade of resorption encountered in 48 samples. It was found to be statistically significant with a positive correlation. This relation is graphically represented in [Graph 1].
| KPG Index | Resorption | |||
|---|---|---|---|---|
| Spearman’s Rho | KPG Index | Correlation Coefficient | 1.000 | 0.545** |
| Sig. (2-tailed) | . | <0.001 | ||
| n | 48 | 48 | ||
| Resorption | Correlation Coefficient | 0.545** | 1.000 | |
| Sig. (2-tailed) | <0.001 | . | ||
| n | 48 | 48 | ||

- Correlation between KPG Index of impacted canine and grade of root resorption of adjacent teeth.
[Table 3] shows the correlation between sector analysis and the grade of resorption encountered in 48 samples. It was found to be statistically significant with a positive correlation. This relation is graphically represented in [Graph 2].
| Resorption | Sector | |||
|---|---|---|---|---|
| Spearman’s Rho | Resorption | Correlation coefficient | 1.000 | 0.433** |
| Sig. (2-tailed) | 0.002 | |||
| N | 48 | 48 | ||
| Sector | Correlation coefficient | 0.433** | 1.000 | |
| Sig. (2-tailed) | 0.002 | |||
| n | 48 | 48 |

- Correlation between Sector Analysis of impacted canine and grade of root resorption of adjacent teeth.
[Table 4] shows the correlation between the inclination of the impacted canine in the frontal plane, as represented by Angle α and the grade of resorption encountered in 48 samples. It was found to be statistically significant with a positive correlation. This relation is graphically represented in [Graph 3].
| Resorption | Angle α | |||
|---|---|---|---|---|
| Spearman’s Rho | Resorption | Correlation coefficient | 1.000 | 0.532** |
| Sig. (2-tailed) | . | 0.000 | ||
| n | 48 | 48 | ||
| Angle α | Correlation coefficient | 0.532** | 1.000 | |
| Sig. (2-tailed) | 0.000 | . | ||
| n | 48 | 48 | ||

- Correlation between Angle α of impacted canine and grade of root resorption of adjacent teeth.
[Table 5] shows the correlation between the inclination of the impacted canine in the frontal plane, as represented by angle β and the grade of resorption encountered in 47 samples. It was found to be statistically significant with a positive correlation. This relation is graphically represented in [Graph 4].
| Resorption | Angle β | |||
|---|---|---|---|---|
| Spearman’s Rho | Resorption | Correlation Coefficient | 1.000 | 0.396** |
| Sig. (2 tailed) | . | 0.006 | ||
| n | 48 | 47 | ||
| Angle β | Correlation Coefficient | 0.396** | 1.000 | |
| Sig. (2 tailed) | 0.006 | . | ||
| n | 47 | 47 | ||

- Correlation between Angle β of impacted canine and grade of root resorption of adjacent teeth.
[Table 6] shows the correlation between vertical degree of eruption of the impacted canine in the frontal plane on orthopantomogram, as represented by d1 and the grade of resorption encountered in 48 samples. It was found to be statistically significant with a positive correlation. This relation is graphically represented in [Graph 5].
| Resorption | d1 | |||
|---|---|---|---|---|
| Spearman’s Rho | Resorption | Correlation Coefficient | 1.000 | 0.442** |
| Sig. (2-tailed) | . | 0.002 | ||
| n | 48 | 48 | ||
| d1 | Correlation Coefficient | 0.442** | 1.000 | |
| Sig. (2-tailed) | 0.002 | . | ||
| N | 48 | 48 | ||

- Correlation between d1 of impacted canine and grade of root resorption of adjacent teeth.
[Table 7] shows the correlation between vertical degree of eruption of the impacted canine in the frontal plane on lateral cephalogram, as represented by d2 and the grade of resorption encountered in 48 samples. It was found to be statistically significant with a positive correlation. This relation is graphically represented in [Graph 6].
| Resorption | d2 | |||
|---|---|---|---|---|
| Spearman’s Rho | Resorption | Correlation Coefficient | 1.000 | 0.383** |
| Sig. (2-tailed) | . | 0.007 | ||
| n | 48 | 48 | ||
| d2 | Correlation Coefficient | 0.383** | 1.000 | |
| Sig. (2-tailed) | 0.007 | . | ||
| n | 48 | 48 | ||

- Correlation between d2 of impacted canine and grade of root resorption of adjacent teeth.
[Table 8] highlights the mean and standard deviation of all variables analyzed in 48 samples. The range of values of all variables is summarized. Of the 48 samples examined, the mean KPG score was 13.67 ± 6.336 and the average KPG index was found to be 2.5 ± 1.13. The average sector in which the impacted canines were located was 1.04 ± 3. The mean distance between the cusp tip of the impacted canine and the occlusal plane on orthopantomogram was 11.10 ± 3.71 and on lateral cephalogram was 11.32 ± 3.74. The mean inclination of the long axis of the impacted canine with the midline of the dentition was 43.71 ± 19.30 m and that with the long axis of the adjacent lateral incisor was 43.26 ± 18.87. The average grade of resorption encountered into be 0.94 ± 1.227.
| KPG Score | KPG Index | Sector | d1 | d2 | Angle α | Angle β | Resorption | |
|---|---|---|---|---|---|---|---|---|
| N Valid | 48 | 48 | 48 | 48 | 48 | 48 | 47 | 48 |
| Missing | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 |
| Mean | 13.67 | 2.50 | 2.75 | 11.106 | 11.329 | 43.7125 | 43.26383 | 0.94 |
| Std. Deviation | 6.336 | 1.130 | 1.042 | 3.7121 | 3.7472 | 19.3001 | 18.87861 | 1.227 |
| Range | 20 | 3 | 3 | 17.7 | 16.1 | 75.3 | 79.9 | 3 |
| Minimum | 5 | 1 | 1 | 2.1 | 3.2 | 5.7 | 3.7 | 0 |
| Maximum | 25 | 4 | 4 | 19.8 | 19.3 | 81 | 83.6 | 3 |
After applying multiple linear regression analysis, the model summary was derived. The model fit obtained was 0.692, with R2 and adjusted R2 values equal to 0.479 and 0.400, respectively (F = 6.120, P < 0.001) as shown in [Table 9]. This relation was found to be statistically significant.
| Model | R | R2 | Adjusted R2 | Std. Error of the Estimate | Change statistics | ||||
|---|---|---|---|---|---|---|---|---|---|
| R2 Change | F Change | df1 | df2 | Sig. F Change | |||||
| 1 | 0.692 | 0.479 | 0.400 | 0.931 | 0.479 | 6.120 | 6 | 40 | 0.000 |
Considering root resorption as the dependent variable, the model for logistic regression analysis produced a significant difference of 0.000 with R2 value of 0.479.
This shows that angle α and angle β have subsequent effect on root resorption.
DISCUSSION
The purpose of our study was to evaluate and correlate the relationship between the severity of root resorption of adjacent teeth and the level of difficulty of impacted canine classified by modified KPG index and sector analysis using CBCT. There are several studies that highlight the advent of CBCT to evaluate the 3D location of impacted canine and its spatial relationship with the adjacent structures. Several authors have attempted to document the incisor root resorption inflicted by the respective ectopically erupting canine.[6-10,16-25] However, through an exhaustive search of the existing literature, no studies exist that derives a correlation between the severity of root resorption and the level of difficulty of the impacted canine.
In our study, the ectopically erupting canine induced root resorption of at least one adjacent tooth in 43.75% of the samples. We observed that the lateral incisors, central incisors and 1st premolars accounted for 52.38%, 28.57%, and 19.04% of the resorptive lesions, respectively, making the lateral incisor most susceptible to root resorption. The root length of 42.86% of the resorbed teeth appeared to be normal when compared with the root length of the healthy contralateral teeth. This means that 57.14% of the resorbed adjacent teeth displayed obliteration in root length. The vitality of the pulp due to severe root resorption of the affected teeth needs to be evaluated separately.
It is evident that the degree of root resorption plays a key role in orthodontic treatment planning. Atypical extraction patterns have to be taken into consideration depending on the severity of canine impaction and the degree of root resorption induced by it. In the research, we conducted, Ericson and Kurol’s classification of root resorption was used to classify the resorptive lesions into mild, moderate and severe categories.[9] The results of this study showed that 47.61% of the resorptive lesions were severe, that is, exposed the pulpal cavity, whereas the mild and moderate categories accounted for 33.33% and 23.8%, respectively.
We determined the level of difficulty of the impacted canine using the KPG index.[13] It is evident that comprehension of the 3D spatial position of the impacted canine is of paramount importance. The decision to salvage an intricately located impacted canine is often a dilemma in orthodontic practice. The KPG index allows us to determine the level of complication associated in aligning the impacted canine into ideal occlusion by means of a scoring system. This index helps the ortho-surgical team to be decisive about the treatment plan before its implementation. A linear correlation was noted between the KPG index and the occurrence of root resorption of the adjacent teeth. This correlation was found to be statistically significant (r = 0.544, P = 0.01). According to the linear regression analysis, it was found that a KPG score above 13.67 could be a resourceful predictor for detecting root resorption.
Guarnieri et al. correlated the degree of root resorption of adjacent teeth with the inclination of the ectopically erupting canine as reflected by its angular measurements.[18] The findings of our study are analogous with their study. In our study, a positive correlation existed between the severity of canine impaction as determined by sector analysis and the degree of root resorption (r = 0.433, P = 0.01). Root resorption was found to be more likely when the canine acquired a more mesial path of eruption. In other words, impacted canines located in Sector 3 and Sector 4, according to Lindauer’s sector analysis inflicted a greater amount of root resorption of the adjoining teeth. Furthermore, the KPG index evaluates the spatial position of impacted canines in all three planes, as opposed to the sector analysis which provides a two-dimensional vision. Thus, a correlation between root resorption and a 3D index seemed mandatory. The inclination of the impacted canine in the frontal plane as represented by angle α and angle β was linearly correlated with the degree of root resorption (r = 0.532, P = 0.01 for angle α and r = 0.396, P = 0.01 for angle β). An increase in these angular measurements reflected a greater risk of induced root resorption of the adjacent teeth. It was found that angle α and angle β exceeding a mean value of 43.71° and 43.26°, respectively, could be resourceful predictors of detecting root resorption.
The degree of vertical eruption of the impacted canine was determined using 2 linear measurements, that is, d1 and d2. A linear correlation was noted between these values and the resorptive lesions. (r = 0.442, P = 0.01 for d1 and r = 0.338, P = 0.01 for d2). An increase in these linear measurements was suggestive of highly placed canines, farther away from the occlusal plane. These canines were more likely to induce root resorption of the adjacent teeth. On the other hand, ectopically erupting canines that are more vicinal toward the occlusal plane do not tend to resorb their neighboring teeth. It was found that d1 and d2 values exceeding 11.1 mm and 11.3 mm, respectively, could be resourceful predictors of detecting root resorption.
Brin and Becker in their study evaluated the relationship between the resorptive lesions caused by the eruptive path of the ectopically erupting canine and the anatomic features of the adjacent lateral incisors.[20] From our observations, we found that the maximum amount of resorptive lesions were observed in the roots of the adjacent lateral incisors. All the lateral incisors that pertained root resorption had normal morphological features. Six samples exhibited the typical “splaying” pattern of the lateral incisors caused by the altered eruptive path of the impacted canines. One sample exhibited agenesis of the lateral incisor, which was most likely the cause of canine impaction due to lack of root guidance. In this case, severe root resorption was seen with respect to the 1st premolar.
In our study, the physical proximity of the cusp and root tips of the impacted canines and the roots of the adjacent teeth played a significant role in initiating root resorption. Three samples in our study pertaining KPG scores between 21 and 22 which showed extreme difficulty, did not display any signs of root resorption. This indicates that a greater difficulty in the level of impaction of canine does not necessarily commensurate root resorption. These canines exhibited a severely horizontal path of eruption, almost parallel to the nasal floor. This feature corresponded to marked discrepancies in all the axes assessed while performing KPG index, thereby designating extreme scores. It is imperative to note that despite the level of difficulty of impaction being “Extreme” or “Very difficult,” the canines were too remotely placed to incite root resorption of the adjacent teeth. This finding highlights the significance of analyzing the proximity of the impacted cuspid and the adjacent roots while detecting root resorption. This finding remains consistent with the findings of another study by Yan et al. who suggested that a physical proximity of <1 mm increased the risk of root resorption of the adjacent structures.[21]
We aimed to derive a correlation between a 3D index, that is, KPG index and the incidence of root resorption, and a correlation between the severity of canine impaction as foretold by sector analysis and root resorption. A linear positive correlation was found. It was also observed that the inclination of the impacted canine in the frontal plane and the degree of vertical eruption of the canine also influence the occurrence and severity of root resorption.
Implementing these analyses can benefit clinicians in the interceptive stages of orthodontic treatment to determine the risk of root resorption. Timely screening and diagnosis of resorptive lesions can assist orthodontic treatment modulation, possibly saving the adjacent teeth.
CONCLUSION
A positive correlation exists between the level of difficulty of canine impaction and root resorption of the adjacent teeth. Impacted canines having higher KPG indices are more susceptible to inflicting root resorption of the neighboring teeth. A KPG score higher than 13.67 can be a resourceful predictor of resorptive lesions
A positive correlation exists between the level of canine impaction and root resorption of the adjacent teeth. There is an increased tendency of root resorption of the neighboring teeth as the impacted canine approaches mesially toward the midline. Root resorption is linearly correlated with Lindauer’s sector analysis
A positive correlation exists between the inclination of the long axis of the canine in the frontal plane. There is an increased tendency of root resorption of the neighboring teeth when angle α and angle β exceed 43.71° and 43.26°, respectively. Angle α and angle β can be resourceful predictors of resorptive lesions
A positive correlation exists between the degree of vertical eruption of the impacted canine. There is an increased tendency of root resorption of the neighboring teeth when d1 and d2 exceed 11.1 mm and 11.3 mm, respectively. Both d1 and d2 can be resourceful predictors of resorptive lesions
An impacted canine with angle α and angle β more than 43.71° and 43.26° respectively, in Sector 3 or 4, and a KPG Score of more than 13.67, are all suggestive of high chances of root resorption of the adjacent tooth.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
None.
References
- Local factors in impaction of maxillary canines. Acta Odontol Scand. 1968;26:145-68.
- [CrossRef] [PubMed] [Google Scholar]
- Radiographic assessment of maxillary canine eruption in children with clinical signs of eruption disturbance. Eur J Orthod. 1986a;8:133-40.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical management of impacted maxillary canines. Semin Orthod. 1998;4:87-98.
- [CrossRef] [PubMed] [Google Scholar]
- A review of impacted permanent maxillary cuspids--diagnosis and prevention. J Can Dent Assoc. 2000;66:497-501.
- [Google Scholar]
- Etiology of maxillary canine impaction: A review. Am J Orthod Dentofacial Orthop. 2015;148:557-67.
- [CrossRef] [PubMed] [Google Scholar]
- Incisor resorption caused by maxillary cuspids. A radiographic study. Angle Orthod. 1987;57:332-46.
- [Google Scholar]
- Radiographic examination of ectopically erupting maxillary canines. Am J Orthod Dentofacial Orthop. 1987;91:483-92.
- [CrossRef] [PubMed] [Google Scholar]
- Resorption of incisors after ectopic eruption of maxillary canines: A CT study. Angle Orthod. 2000;70:415-23.
- [Google Scholar]
- Incisor root resorptions due to ectopic maxillary canines imaged by computerized tomography: A comparative study in extracted teeth. Angle Orthod. 2000;70:276-83.
- [Google Scholar]
- Resorption of maxillary lateral incisors caused by ectopic eruption of the canines. A clinical and radiographic analysis of predisposing factors. Am J Orthod Dentofacial Orthop. 1988;94:503-13.
- [CrossRef] [PubMed] [Google Scholar]
- Three-dimensional localization of maxillary canines with cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2005;128:418-23.
- [CrossRef] [PubMed] [Google Scholar]
- Two-versus three-dimensional imaging in subjects with unerupted maxillary canines. Eur J Orthod. 2011;33:344-9.
- [CrossRef] [PubMed] [Google Scholar]
- A novel 3D classification system for canine impactions--the KPG index. Int J Med Robot. 2009;5:291-6.
- [CrossRef] [PubMed] [Google Scholar]
- The validation of a novel index assessing canine impactions. Eur J Dent. 2013;7:399-404.
- [CrossRef] [PubMed] [Google Scholar]
- The KPG index--a novel 3D classification system for maxillary canine impactions. Tex Dent J. 2012;129:265-74.
- [Google Scholar]
- Canine impaction identified early with panoramic radiographs. J Am Dent Assoc. 1992;123:91-2, 95-7
- [CrossRef] [PubMed] [Google Scholar]
- Cone-beam computed tomography findings of impacted upper canines. Imaging Sci Dent. 2014;44:287-92.
- [CrossRef] [PubMed] [Google Scholar]
- Impacted maxillary canines and root resorption of adjacent teeth: A retrospective observational study. Med Oral Patol Oral Cir Bucal. 2016;21:e743-50.
- [CrossRef] [PubMed] [Google Scholar]
- Comparative analysis of traditional radiographs and cone-beam computed tomography volumetric images in the diagnosis and treatment planning of maxillary impacted canines. Am J Orthod Dentofacial Orthop. 2010;137:590-7.
- [CrossRef] [PubMed] [Google Scholar]
- Resorbed lateral incisors adjacent to impacted canines have normal crown size. Am J Orthod Dentofacial Orthop. 1993;104:60-6.
- [CrossRef] [PubMed] [Google Scholar]
- Maxillary canine impaction increases root resorption risk of adjacent teeth: A problem of physical proximity. Orthod Fr. 2015;86:169-79.
- [CrossRef] [PubMed] [Google Scholar]
- Predictors of root resorption associated with maxillary canine impaction in panoramic images. Eur J Orthod. 2016;38:292-9.
- [CrossRef] [PubMed] [Google Scholar]
- Maxillary incisor root resorption in relation to the ectopic canine: A review of 26 patients. Eur J Orthod. 1997;19:79-84.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of 6 cone-beam computed tomography systems for image quality and detection of simulated canine impaction-induced external root resorption in maxillary lateral incisors. Am J Orthod Dentofacial Orthop. 2011;140:e129-39.
- [CrossRef] [PubMed] [Google Scholar]
- The position of maxillary canine impactions and the influenced factors to adjacent root resorption in the Korean population. Eur J Orthod. 2012;34:302-6.
- [CrossRef] [PubMed] [Google Scholar]




