

Translate this page into:
Evaluation of apical root resorption in orthodontic patients with maxillary anterior intrusion using utility arches and mini screws: A comparative clinical trial
Address for correspondence: Dr. Muraleedhara Bhat, Department of Orthodontics, Coorg Institute of Dental Sciences, Virajpet Coorg District, Karnataka, India. E-mail: drmurali13@rediffmail.com
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Objectives
The purpose of this study was to compare the amount of apical root resorption in orthodontic patients undergoing maxillary anterior intrusion using utility arches and mini screws; and to compare the efficacy of mini screws and utility arches in reducing over bite.
Materials and Methods
The study sample consisted of 20 patients, divided in two groups. Group A consisted of ten patients in whom titanium mini-screws were used Group B consisted of 10 patients in whom utility arches made of 0.017 × 0.25″ TMA were used. Diagnostic records (study models and radiovisiography [RVG]) were taken at 2 time intervals, T1 (just before implant/utility arch placement) and T2 (at the end of intrusion 6 months later). The pre and post radiographic images were measured from incisal tip to the root apex with the help of intrascan DC software. Root resorption was computed as the difference between the pre-treatment total tooth length and the post treatment total tooth length. These values were subjected to statistical analyses using SPSS 16.00 statistical software. (Statistical Package for the Social Sciences, IBM Corporation, December 2007)
Results
The results showed that root resorption was seen in both groups. Amount of resorption seen was higher in mini implant group than utility arch group. Mini implants were more efficient in reducing the overbite when compared to utility arches.
Conclusion
It was concluded from the study that intrusion using mini implant resulted in more root resorption than utility arch; and mini implant was more effective in intruding the incisors than utility arch.
Keywords
Intrusion
mini implant
root resorption
utility arch

INTRODUCTION
Deep bite is one of the most common malocclusions seen in orthodontic patients, it can also occur along with other associated malocclusions.[1]
Graber has defined “deep bite” as a condition of excessive overbite, where the vertical measurement between the maxillary and mandibular incisal margins is excessive when the mandible is brought into habitual or centric occlusion. It is said to be one of the most deleterious malocclusions for long term health of the masticatory apparatus and the dental units.[2] Thus an optimal treatment of deep bite requires a proper diagnosis, a careful treatment plan and an efficient appliance design. Deep bite can be corrected by the intrusion of anterior teeth, extrusion of posterior teeth or a combination of both.[3] Even though intrusion of incisors is said to be stable form of deep bite correction, root resorption can occur as an adverse effect.
In this study, two methods of incisor intrusion, mini implants and intrusion utility arches were compared for root resorption and their efficacy in carrying out intrusion.
MATERIALS AND METHODS
Patients with over bite of more than 3 mm were selected for the study. The sample consisted of 20 patients who were distributed in two groups, Group A and Group B of 10 subjects each. In Group A, intrusion was carried with the help of titanium mini-implants, (Abso Anchor, Dentos, Taegu, Korea) [Figure 1]; and in Group B, intrusion utility arches were used. Forces were measured using Dontrix gauge (Leone, Italy). Intra oral Photographs were taken for the two groups at T1 and T2 [Figures 2-4]
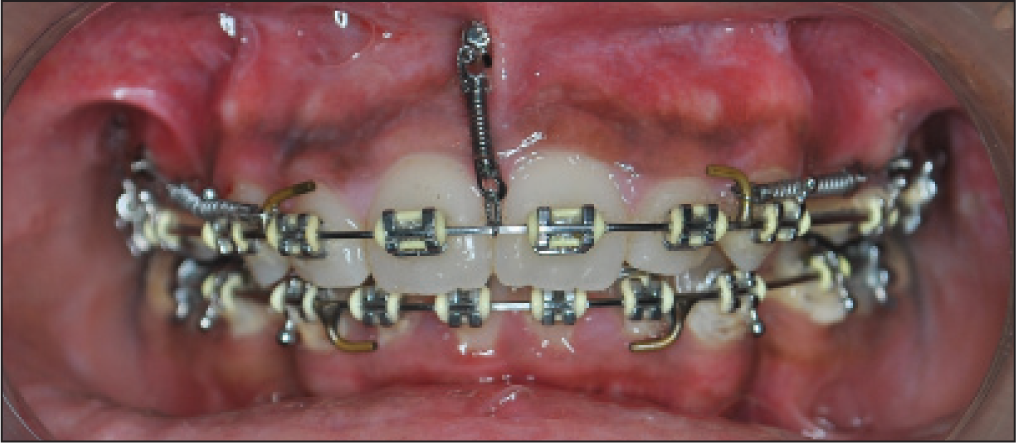
- Intrusion using mini implant at T1

- End of intrusion using mini implant at T2

- Intrusion using utility arch at T1

- End of intrusion using utility arch at T2
The inclusion criteria were:
Patients with overbite more than 3 mm.
Incisor display more than 2 mm at rest.
Patients in the age group of 12-25 years.
The exclusion criteria were:
Patients with active periodontal disease.
Root canal treated anterior teeth.
Patients with mutilated dentition.
Individuals with history of medical conditions such as asthma, hypothyroidism and diabetes.
Measurement of root resorption
Radiovisiography (RVG) technique was used to measure the root resorption. Distance from the object to the sensor was kept constant using paralleling cone technique. RVGs were taken at 2 time intervals; one just before mini implant placement in group A and utility arch placement in Group B (T1), second at the end of intrusion 6 months later (T2) [Figures 5-8]. The pre and post-intrusion radiographic images were measured from incisal tip to the root apex with the help of intrascan DC software (J.D Edwards, Washington DC). Root resorption was computed as the difference between total tooth length at T1 and the total tooth length at T2.

- Pre-treatment radiovisiography for mini implant before intrusion at T1

- After intrusion radiovisiography for mini implant at T2

- Pre-treatment radiovisiography for utility arch before intrusion at T1

- After intrusion radiovisiography for utility arch at T2
Measurement of deep bite correction
Deep bite was measured on study models made at T1 and T2 in both the groups to determine the efficiency of the two intrusion mechanics.
Treatment mechanics
In Group A intrusion was carried out using mini implants, which were placed below the anterior nasal spine region after leveling and alignment. A calculated force of 40 gms was applied using Ni-Ti closed coil spring (GAC, Japan) for intrusion.
In Group B, intrusion was carried out using intrusion utility arch made with 0.017 × 0.025″ TMA (Ormco, USA) archwire after levelling and aligning the incisors. The utility arch was used as a two couple system with the incisal portion engaged onto the bracket slots. The utility arch was activated to generate force of 40 gm at the time of insertion of the wire.
RESULTS
Total lengths of central and lateral incisors in both the groups were measured on the radiographic images at T1 and T2 [Tables 1 and 2]. At T1, mean value of central incisors was 24.50 mm (±1.094) in Group A, 22.85 mm (±0.742) in Group B. At T1, mean value of lateral incisors was 21.91 mm (±0.655) in Group A, 20.86 mm (±0.468) in Group B.
| Group | N | Mean | Standard deviation | Standard error mean |
|---|---|---|---|---|
| Central incisor | ||||
| Mini implant | 20 | 24.50 | 1.094 | 0.245 |
| Utility arch | 20 | 22.85 | 0.742 | 0.166 |
| Lateral incisor | ||||
| Mini implant | 20 | 21.91 | 0.655 | 0.147 |
| Utility arch | 20 | 20.86 | 0.468 | 0.105 |
| Group | N | Mean | Standard deviation | Standard error mean |
|---|---|---|---|---|
| Central incisor | ||||
| Mini implant | 20 | 23.55 | 1.095 | 0.245 |
| Utility arch | 20 | 22.28 | 0.754 | 0.169 |
| Lateral incisor | ||||
| Mini implant | 20 | 21.22 | 0.610 | 0.136 |
| Utility arch | 20 | 20.38 | 0.440 | 0.098 |
At T2, mean value of central incisors was 23.55 mm (±1.095) in Group A, 22.28 mm (±0.754) in Group B. At T2, mean value of lateral incisors was 21.22 mm (±0.610) in Group A, 20.38 mm (±0.440) in Group B.
Paired Sample tests were performed for central, lateral incisors at T1 and T2 for both the groups [Tables 3 and 4] (Graph 1 and Graph 2).
| Mini screw group | N | Mean (standard deviation) (in mm) | t-value | P value |
|---|---|---|---|---|
| T1 | 10 | 4.35 (0.58) | 11.759 | 0.000 |
| T2 | 10 | 3.05 (0.55) | 0.000 |
| Utility arch group | N | Mean (standard deviation) (in mm) | t-value | P value |
|---|---|---|---|---|
| T1 | 10 | 4.35 (0.58) | 15.492 | 0.000 |
| T2 | 10 | 3.95 (0.57) | 0.000 |
- Paired samples statistics between T1 and T2 (central incisors) in mini implant group and utility arch group
- Paired samples statistics between T1 and T2 (lateral incisors) in mini implant group and utility arch group
Group A
Central incisors
The mean of two groups when tested using t-test showed a t value of 13.42 mm (P = 0.000), which was statistically significant. They were also clinically significant since mini implant produced intrusion and showed root resorption in the central incisors.
Lateral incisors
The mean of two groups when tested using t-test showed a t value of 18.029 (P = 0.000) which was statistically significant. Clinically, they were of significance since mini implant produced intrusion and showed root resorption in lateral incisors.
Group B
Central incisors
The mean of two groups when tested using t-test showed a t value of 37.205 (P = 0.000) which was statistically significant. Clinically, they were of significance since utility arch produced intrusion and showed root resorption in central incisors.
Lateral incisors
The mean of two groups when tested using t-test showed a t value of 20.315 (P = 0.000) which was statistically significant. Clinically, they were of significance since utility arch produced intrusion and showed root resorption in lateral incisors.
Group statistics
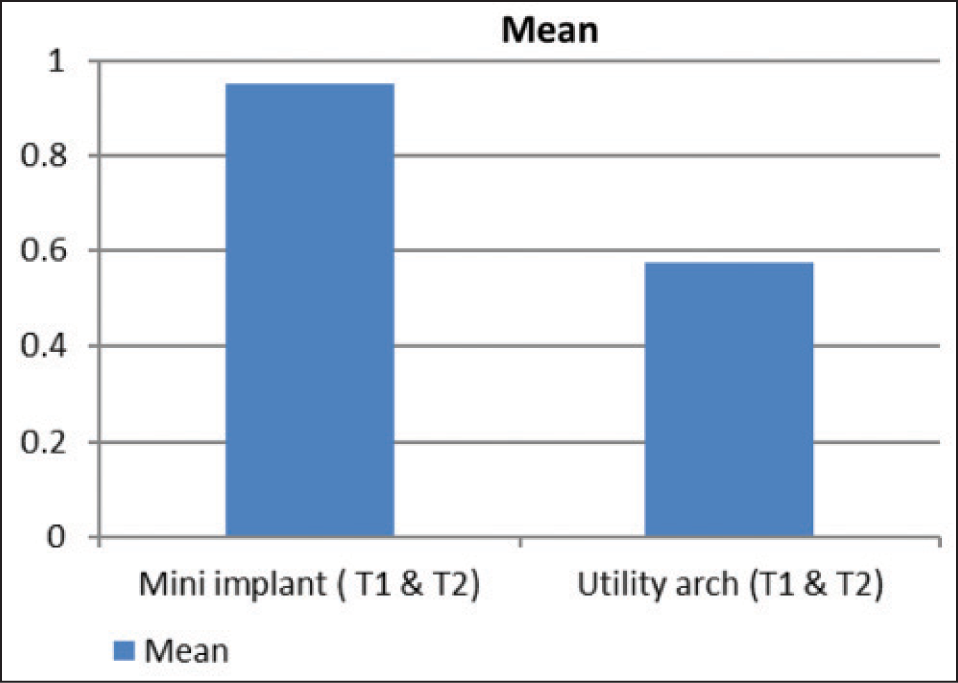
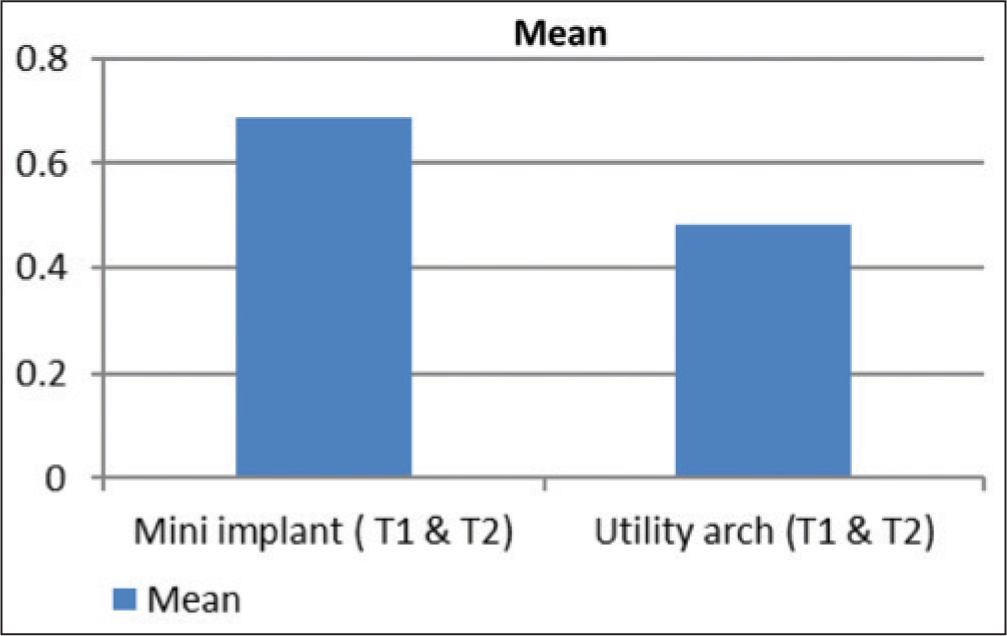
Statistics was performed to asses mean amount of root resorption in groups A and B. In case of central incisor, it was observed that the mean of T1 and T2 in mini implant group was 0.94 mm (±0.31372) and that of utility arch group was 0.57 mm (±0.06924). In case of lateral incisor the mean of T1 and T2 in mini implant group was 0.68 mm (±0.17054) and in utility arch group was 0.48 mm (±0.10611). The mean of two groups when tested using t-test showed a t value of 5.192 (P = 0.000) among central incisor group and a t value of 4.576 (P = 0.000) in lateral incisor group. This showed that the amount of root resorption seen was higher in mini implant group than the utility arch group.
Paired t-test was performed among study model overbite measurements at T1 and T2 in mini implant group for determining the efficacy of intrusion. It was observed that the mean of T1 in mini implant group was 4.35 mm (±0.58) and in T2 was 3.05 mm (±0.55). This showed that deep overbite reduction was significant in mini implant group.
Independent t-test showing the mean amount of overbite correction was calculated. It was observed that the mean amount of overbite correction in mini implant group was 1.30 mm, which was significantly higher than 0.40 mm, in the utility arch group.
DISCUSSION
Excessive overbite is a complex orthodontic problem that may involve a group of teeth or whole dentition, alveolar bone, maxillary and mandibular basal bones and/ or soft-tissue of the face.[4] When a tooth is intruded, optimum force of 15 gm should be used since the force is concentrated over a small area at the apex.[5]
Mini-implants have been used to intrude incisors since 1983, when Creekmore and Eklund reported using a metal implant to correct deep overbite. Mini implants have the advantages of immediate loading, multiple placement sites, uncomplicated placement and removal procedures and minimal expense for patients.[6]
The intrusion utility arch is a two-couple system, created by engaging the rectangular wire into the incisor brackets; in which the precise magnitude of forces and couples cannot be known, especially if torque bends or cinch back are incorporated in the archwire.[7] Inflammatory root resorption is a side-effect related to the biological tissue response that enables teeth to be moved during orthodontic treatment.[8]
In our study, we compared the root resorption and efficiency of intrusion of two most commonly used intrusion mechanics, namely the mini implant and the intrusion utility arch. In our study, we used the two couple system design of the intrusion utility arch, created by engaging the rectangular wire into the incisor brackets.
Our study showed that root resorbtion was seen in both mini implant and utility arch group, but more for the mini-implant group. The continuous force applied by the mini implant, Ni-Ti coil spring and the lesser force degradation of the coil spring might be the reason for the increased root resorption seen in the mini implant group.
Our results showed that the mini implant was more effective in intruding the incisors compared to the utility arch. Though the force levels used were the same in both the groups, the possible reasons for the increased efficiency of the mini-implant in terms of intrusion may be:
Point of force application more closer to the center of resistance of the incisor tooth.
More of a continuous type of force applied by the Ni-Ti coil spring implant system.
Force degradation less in implant intrusion.
In our study, we noticed some amount of flaring of the incisors in both the study groups. This may be attributed to the application of force buccal to the centre of resistance of the incisors. The flaring was minimal in the intrusion utility arch group, the possible reason being the cinch back of the utility arch in the molar region. Since we have used a two couple system utility arch for our study the precise magnitude of forces and couples cannot be known. The comparison of a similar two couple system with a one couple system is a topic for future research.
Polat-Özsoy et al.[9] in their study compared the effects of incisor intrusion obtained with the aid of miniscrews and utility arches. Their results showed that by using mini implant overbite correction can be achieved by application of intrusive forces, which is closer to the center of resistance with no counteractive movements in the molars. In the case of utility arches, more of a tipping movement was seen and the intrusive forces were distributed over a wide area. The results of this study were similar to ours. McFadden et al.[10] evaluated the relationship between intrusion with low forces (25 g) using utility arches in the bioprogressive technique and root shortening. The study concluded that there was no relationship between the root resorption and force that is used for intrusion, but is directly related to the duration of the treatment. In our study, the duration of treatment was kept constant and more importance was given to the mechanics of intrusion used. Amasyali et al.[11] compared the intrusive effects of the Connecticut Intrusion Arch (CIA) and the Utility Intrusion Arch (UIA). Their study concluded that the CIA and UIA are both effective in the intrusion of incisors and can be used successfully in the treatment of deep overbite.
CONCLUSIONS
The present study was conducted to evaluate the amount of apical root resorption seen during intrusion of maxillary incisors by mini implants and intrusion utility arches. It was concluded from the study that
Both the mini implant and intrusion utility arch were useful in intrusion of maxillary incisors.
Root resorption was seen in both mini implant and utility arch groups.
Root resorption was more in mini implant group than in the utility arch group.
Mini implants were more efficient in reducing the overbite when compared to utility arches.
Source of Support:
Nil.
Conflict of Interest:
None declared.
References
- Treatment effects of intrusion arches and mini-implant systems in deepbite patients. Am J Orthod Dentofacial Orthop. 2012;141:723-33.
- [Google Scholar]
- A mini-implant for orthodontic anchorage in a deep overbite case. Angle Orthod. 2005;75:444-52.
- [Google Scholar]
- Intrusion of multiradicular teeth and related root resorption with mini-screw implant anchorage: A radiographic evaluation. Am J Orthod Dentofacial Orthop. 2007;132:647-55.
- [Google Scholar]
- Apical root resorption during orthodontic treatment. A prospective study using cone beam CT. Angle Orthod. 2012;82:480-7.
- [Google Scholar]
- Comparison of the intrusive effects of miniscrews and utility arches. Am J Orthod Dentofacial Orthop. 2011;139:526-32.
- [Google Scholar]
- A study of the relationship between incisor intrusion and root shortening. Am J Orthod Dentofacial Orthop. 1989;96:390-6.
- [Google Scholar]
- Intrusive effects of the connecticut intrusion arch and the utility intrusion arch. Turk J Med Sci. 2005;35:407-15.
- [Google Scholar]




