

Translate this page into:
Investigation of the correlation of midpalatal suture maturation stage with chronological age and cervical vertebral maturation stage


*Corresponding author: Chen-Jung Chang, Department of Stomatology, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan City, Taiwan. zoechang0405@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Yang C, Chen M, Liu J, Chang C. Investigation of the correlation of midpalatal suture maturation stage with chronological age and cervical vertebral maturation stage. APOS Trends Orthod. 2024;14:164-9. doi: 10.25259/APOS_86_2023
Abstract
Objectives:
The first aim of this study was to investigate the correlation between chronological age, cervical vertebral maturation (CVM) stage, and midpalatal suture (MPS) maturation stage. The second aim was to assess the relationship between the prognosis for rapid maxillary expansion (RME) and age, CVM stage, and MPS maturation stage.
Material and Methods:
We divided 109 participants into three age groups: <15 years, 15–25 years, and >25 years. The participants had undergone both cone-beam computed tomography (CBCT) and lateral cephalometric X-ray examination. Their MPS maturation stage was classified as A to E and CVM stage as cervical stage 1 (CS1) to CS6, according to a previously proposed method. We used the weighted kappa coefficient to assess intra-examiner agreement and Spearman’s correlation coefficient, to evaluate the correlations of MPS maturation stage with age and CVM stage.
Results:
The weighted kappa coefficients were 0.849 and 0.923 for the identification of MPS maturation stage and CVM stage, respectively. There were significant, but weak correlations between MPS maturation stage and age (r = 0.313, P = 0.001) and, CVM stage (r = 0.287, P = 0.002). MPS stage C was the most prevalent across all age groups and all CVM stages.
Conclusion:
Chronological age and CVM stage may not accurately predict MPS maturation stage, especially in older patients. Further, the prognosis for RME may not be strongly related to either CVM or MPS maturation stage. We recommend using CBCT X-rays for individual MPS assessments before selecting the type of maxillary expansion treatment.
Keywords
Palatal expansion technique
Suture
Cone-beam computed tomography
Malocclusion
Bone screw

INTRODUCTION
Maxillary transverse deficiency can lead to several orthodontic problems, including dental crowding, unilateral or bilateral posterior crossbite, functional shift, mandible deviation, and even nasal airway obstruction.[1-3] The prevalence of maxillary transverse deficiency is approximately 23.3% in the primary dentition and approximately 30% in the permanent dentition.[4]
Rapid maxillary expansion (RME) has long been used to correct maxillary transverse deficiency. The maxilla in the permanent dentition can be expanded using three methods: Conventional tooth-borne, micro-implant-assisted, and surgically assisted RME. Although conventional RME does not require surgery, it uses the teeth for anchorage, involves less skeletal expansion, and can lead to unwanted side effects as interdigitation of the midpalatal suture (MPS) occurs. Surgically assisted RME ensures skeletal expansion but involves invasive surgery and general anesthesia. Mini-screw-assisted RME or micro-implant-assisted rapid palatal expansion (MARPE) was recently introduced and has been shown to expand the MPS in adult patients. However, the prognosis for MARPE remains unpredictable. Moreover, clear guidelines regarding the type of RME to be selected by the clinician are lacking. Chang et al. conducted a finite element study and concluded that MPS ossification plays a key role in determining the reaction force of bone-anchored RME.[5] Furthermore, according to the results of Persson’s study, orthopedic treatment should be effective in patients with an MPS obliteration index of <0.5.[6] Therefore, assessment of MPS ossification or obliteration is essential for decision-making. Chronological age has traditionally guided the clinical decision between conventional RME and surgically assisted RME. However, several histological studies have found no signs of suture fusion in patients aged 27, 32, 54, or even 71 years,[7,8] and the youngest patient with obliteration in the posterior part of the MPS was a 15-year-old girl.[6] The results of studies related to the correlation between chronological age and the MPS maturation stage remain controversial.[6-9]
Angelieri et al. proposed a classification method for identifying an individual’s MPS maturation stage through cone-beam computed tomography (CBCT). This method was proposed to predict the prognosis of conventional RME, and avoid unnecessary surgically assisted RME for adolescents and young adults.[10] According to the results of their research, RME can successfully expand the MPS without surgical intervention when the patient is in maturation stages A–C.[11] However, performing a CBCT scan in orthodontic patients involves exposure to radiation, which hinders its routine usage, especially in adolescents or young adults. A lateral cephalometric radiograph has long been a routine procedure for orthodontic diagnosis and treatment planning. It is not only used for skeletal and dental analyses but also provides information about cervical vertebral morphology on the same film. Baccetti et al. presented six stages of cervical vertebral maturation (CVM) that have been proven to predict the patient’s growth status.[12] To reduce radiation exposure during CBCT, some studies have attempted to correlate CVM stage with Angelieri’s MPS maturation stage. However, this correlation remains controversial.[13-17] In this study, therefore, we evaluated whether a simple diagnostic index – age or CVM stage – could predict MPS maturation stages by investigating the correlation between the patient’s age, CVM stage, and MPS maturation stage. We also assessed the relationship between the prognosis for RME and these three factors.
MATERIAL AND METHODS
This retrospective study was conducted after approval from the Institutional Review Board of our institution had been received (IRB No. B-ER-103-290). In total, 109 participants (age: 7–43 years; 54 males and 55 females) were included in the study. To be included, participants had to have undergone both CBCT and lateral cephalometric X-ray examination. Patients who had undergone previous orthodontic treatments, such as RME and orthognathic surgery were excluded, as were those with any developmental or genetic anomaly related to the craniofacial region, such as cleft lip and palate. Patients with poor-quality images were also excluded from the study.
According to a previous study, the average age of peak velocity of growth in body height is approximately 14 years for males and 12 years for females.[18,19] Surgically assisted RME has, thus, been recommended for patients older than 16 years[20] or 25 years.[21] We, therefore, divided the participants into three age groups: under 15 years, between 15 and 25 years, and older than 25 years. All CBCT images were taken using a DCT 100 (Taiwan CareTech, Kaohsiung, Taiwan), and the settings were as follows: 120 kV, 5.0 mA, field of view of 15 × 9 cm, voxel size 0.25 mm, and exposure time 11 s. The lateral cephalometric X-ray examination was conducted with the patient holding their head in its natural position using an ASAHI Hyper-X CM (Asahi Roentgen, Kyoto, Japan). Image reading was performed using Planmeca Romexis image software (Planmeca, Helsinki, Finland). The CBCT image slices were obtained according to the following protocols: The median sagittal plane was aligned with the nasal septum, and the horizontal plane was aligned with the hard palate [Figure 1]. For those patients in whom the palate had a pronounced curvature or was very thick, two distinct axial image slices were obtained.[10] The MPS maturation stage was classified (from A to E) using the Angelieri et al. method,[10] and the CVM was classified (from cervical stage -CS1 to CS6) according to the method of Baccetti et al.[12]
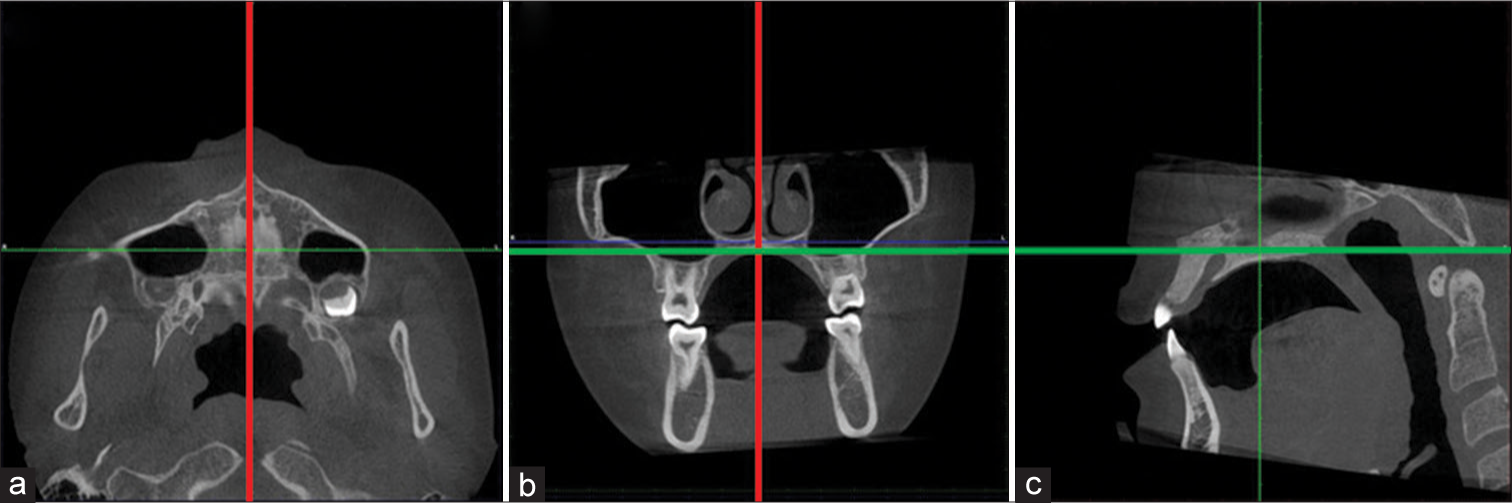
- Cone-beam computed tomography slices obtained using the following protocols: (a and b) The median sagittal plane (red line) was aligned with the nasal septum. (b and c) The horizontal plane (green line) was aligned with the hard palate.
All images were analyzed by a senior orthodontic resident. One month later, the same examiner reclassified all samples in random order. The weighted kappa coefficient was used to evaluate the intra-examiner agreement. Spearman’s correlation coefficient was used to evaluate the correlation of MPS maturation stage with age and CVM stage. Statistical Package for the Social Sciences (SPSS) software version 24 (SPSS, Chicago, IL, USA) was used for statistical analysis, and P < 5% was considered significant.
RESULTS
The weighted kappa coefficients were 0.849 and 0.923 for the classification of MPS maturation stage and CVM stage, respectively. This shows that there was substantial agreement between the two sets of classifications.
MPS maturation stage versus age
The r value for the correlation between MPS stage and age was 0.313, and P < 0.05, which indicates a significant but weak correlation. [Table 1] shows the distribution of MPS maturation stage for the three age groups. Only one participant was in stage A and four participants in the under-15 age group were in stage B. One participant in stage B was in the over-25 age group. [Figure 2] shows that stage C was the most prevalent stage across all age groups. We divided the five MPS maturation stages into two groups: Non-fused (stages A, B, and C) and fused (stage D [partially fused] and stage E [completely fused]). The pie and bar charts [Figures 3 and 4] show the percentage of non-fused and fused sutures in each age group. Both the charts reveal a clear tendency for the percentage of non-fused sutures to decrease with age.
| Chronological age group (years) | MPS maturation stage | Correlation | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| A | B | C | D | E | Total | r | P | |||||||
| n | % | n | % | n | % | n | % | n | % | n | % | |||
| < 15 | 1 | 2.3 | 4 | 9.1 | 26 | 59.1 | 5 | 11.3 | 8 | 18.2 | 44 | 100 | 0.313 | 0.001* |
| 15–25 | 0 | 0 | 0 | 0 | 22 | 48.9 | 16 | 35.6 | 7 | 15.5 | 45 | 100 | ||
| >25 | 0 | 0 | 1 | 5 | 7 | 35 | 6 | 30 | 6 | 30 | 20 | 100 | ||
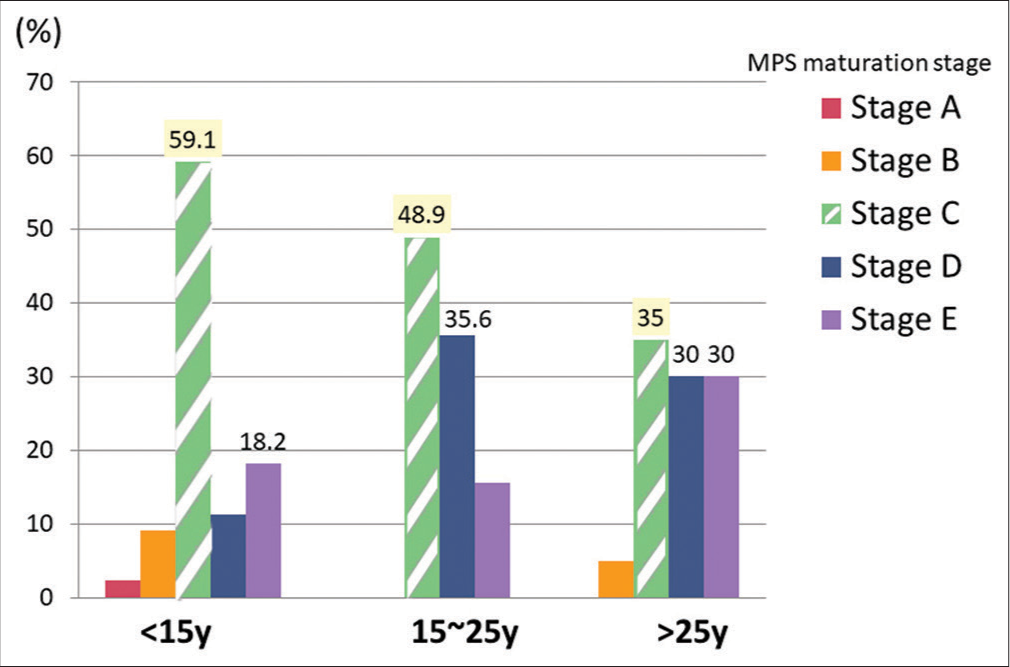
- The distribution of midpalatal suture (MPS) maturation stages across three chronological age groups. Stage C was the most prevalent stage in all age groups.
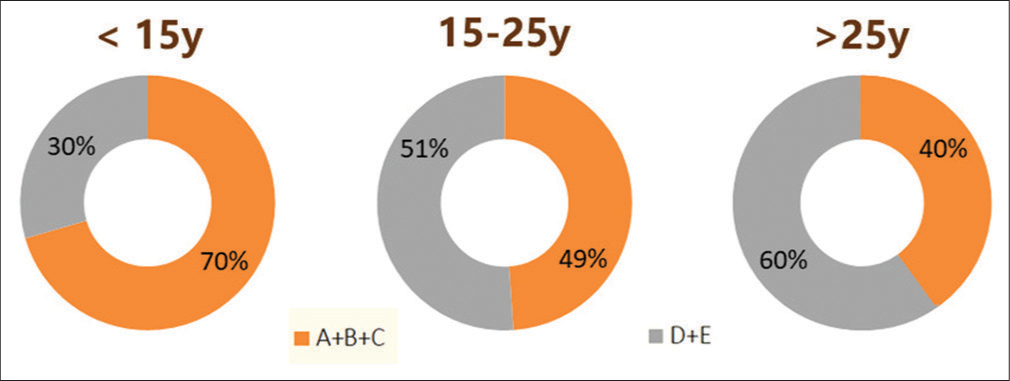
- The percentage of non-fused sutures and fused sutures in each age group. The non-fused sutures included midpalatal suture (MPS) stages (A-C) and the fused sutures included MPS stages (D and E).
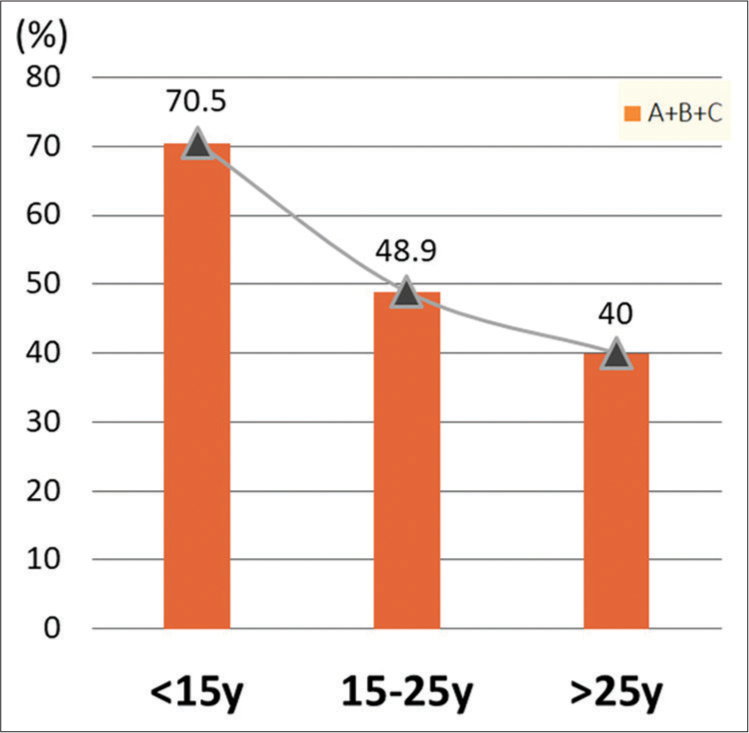
- The percentage of non-fused sutures (midpalatal suture stages A-C) in each age group. There is a clear tendency for the percentage of non-fused sutures to decrease with age.
MPS maturation stage versus CVM stage
The distribution of MPS maturation stages according to CVM stages is shown in [Table 2]. The correlation coefficient was 0.287 and P < 0.05, which indicates a significant but weak correlation. [Figure 5] shows the following patterns: CVM stages 1–3 generally corresponded to MPS stages A–C, and CVM stages 4–6 generally corresponded to MPS stages C–E. MPS maturation stages A and B were mainly distributed in CS1–CS3. However, one 29-year-old female participant was at CVM stage 5 but exhibited MPS maturation stage B.
| CVM stage | MPS maturation stage | Correlation | ||||||
|---|---|---|---|---|---|---|---|---|
| Stage A | Stage B | Stage C | Stage D | Stage E | Total | r | P | |
| CS1 | 0 | 2 | 7 | 0 | 0 | 9 | 0.287 | 0.002* |
| CS2 | 1 | 1 | 1 | 0 | 1 | 4 | ||
| CS3 | 0 | 1 | 9 | 2 | 1 | 13 | ||
| CS4 | 0 | 0 | 6 | 4 | 4 | 14 | ||
| CS5 | 0 | 1 | 14 | 7 | 7 | 29 | ||
| CS6 | 0 | 0 | 18 | 14 | 8 | 40 | ||
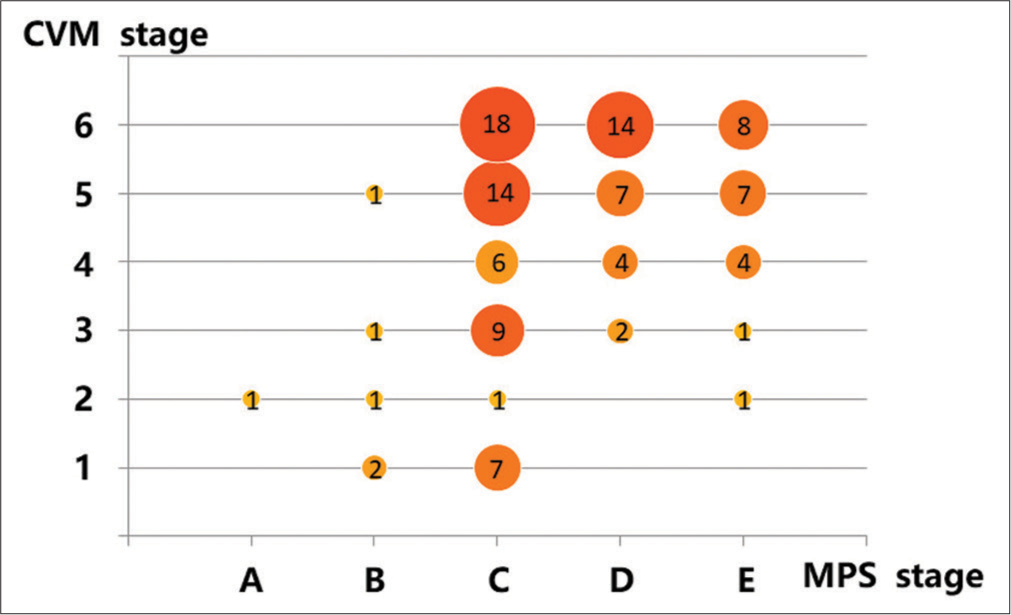
- Distribution of midpalatal suture (MPS) maturation stages according to cervical vertebral maturation (CVM) stage. CVM stages 1–3 generally corresponded to MPS stages (A-C), and CVM stages 4–6 generally corresponded to MPS stages (C-E).
Age, CVM stage, and MPS maturation stage versus RME treatment outcome
Of the 109 participants, 14 received RME treatment. All successful cases for whom conventional RME was used were in stage C. One participant in stage E was successfully treated with MARPE, and MARPE failed in one participant who was in stage D [Table 3].
| No. of subjects | Chronological age | CVM stage | MPS maturation stage | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Treatment outcome | Type of expansion | <15 | 15–25 | >25 | 1 | 2 | 3 | 4 | 5 | 6 | A | B | C | D | E |
| Success | Conventional | 6 | 0 | 0 | 3 | 0 | 0 | 2 | 1 | 0 | 0 | 0 | 6 | 0 | 0 |
| MARPE | 2 | 5 | 0 | 0 | 0 | 0 | 0 | 4 | 3 | 0 | 0 | 2 | 4 | 1 | |
| Failure | Conventional | ||||||||||||||
| MARPE | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | |
MARPE: Micro-implant-assisted rapid maxillary expansion, CVM: Cervical vertebral maturation, MPS: Midpalatal suture, RME: Rapid maxillary expansion
DISCUSSION
The first aim of this study was to identify a simple diagnostic index – age or CVM stage – to help orthodontists assessing MPS maturation stages before selecting maxillary expansion appliances. However, both correlations were significant, they were weak, especially for the oldest age group. Angelieri et al. found great variability in the distribution of MPS stages in patients older than 11 years.[11] The previous studies, which included younger patients, reported a moderate to strong correlation,[14,16,17] while studies including older patients[15,22,23] found no significant correlation or only weak correlations. In our study, 88% of the participants were older than 11 years. The age distribution of our sample may explain the weak correlation between MPS maturation stage and age. Further, Angelieri et al.[10] and Ram and Kannan[24] found that it was mostly patients younger than 13 years who were in MPS maturation stages A and B. We obtained a similar result, in that most of the stages A and B patients were under 12 years, except the one 29-year-old female.
In our study, stage C was the most prevalent stage in all age groups. However, the percentage of non-fused sutures decreased with increasing age. This finding is similar to those of the previous studies involving individuals aged <15 years.[14,25] However, the results of some studies were contradictory to ours; these studies reported stage E as the most prevalent stage in patients older than 15 years.[22,23] Those findings remind us that the correlation between MPS maturation stage and chronological age becomes weaker with increasing age.
Angelieri et al.[13] and Jang et al.[14] revealed a strong positive correlation between CVM and MPS maturation stage, while Lee and Mah[16] and Mahdian et al.[17] found only moderate correlations and Gorucu-Coskuner et al.[15] reported no significant correlation. However, our study produced a contradicting result: A significant but weak correlation. In the studies by Jang et al.[14] and Lee and Mah,[16] CVM stages 1–3 corresponded to MPS stages A–C, except in one participant who was in stage D. In our study, CS1– CS3 also corresponded to MPS stages A–C, except in two patients who were in stage D and two patients who were in stage E. However, other studies have found considerable percentages of non-fused sutures (27–61.9%) in CS5 and CS6 patients.[14-16] We found 51.7% and 45.0% of non-fused sutures in CS5 and CS6 patients, respectively. These findings suggest that even when the patients were in CVM stage 5 or 6, some percentage of non-fused sutures still existed, and suture opening without surgical intervention was still possible.
In this study, all the cases in which conventional RME was successful were at MPS maturation stage C. Similar to the study conducted by Angelieri et al., expanding the maxilla with conventional RME is possible until stage C.[11] In the study of Jesus et al.,[26] which included 25 patients, all patients classified as MPS maturation stage B or C were successfully treated with micro-implant-assisted RME. In contrast, in stages D and E, both failed and successful cases were observed. These findings were similar to those of our study, which was that one patient in stage E was successfully treated with mini-implant-assisted RME while the same treatment failed in one patient in stage D.
CONCLUSION
After a comprehensive investigation, the following conclusions can be drawn:
Significant but weak correlations were observed between MPS maturation stage and age and CVM stage. Therefore, neither patient age nor CVM stage appears to be an accurate index for predicting MPS maturation stage
MPS stage C was the most prevalent stage in all age groups
45–51% of non-fused sutures were found in patients in CVM stage 5 or 6
The prognosis for micro-implant-assisted RME may not be related to MPS maturation stage or CVM stage
Using CBCT X-rays for individual MPS assessment before selecting the maxillary expansion treatment is still recommended and, therefore, cannot be deemed as unnecessary radiation exposure.
Ethical approval
This retrospective study was conducted after approval from the Institutional Review Board of our institution had been received, number (IRB No. B-ER-103-290).
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The author(s) confirms that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Longitudinal study and cost-benefit analysis of the effect of early treatment of posterior cross-bites in the primary dentition. Eur J Orthod. 1992;14:173-9.
- [CrossRef] [PubMed] [Google Scholar]
- A longitudinal study on malocclusion in relation to signs and symptoms of cranio-mandibular disorders in children and adolescents. Eur J Orthod. 1990;12:399-407.
- [CrossRef] [PubMed] [Google Scholar]
- The role of rapid maxillary expansion in the promotion of oral and general health. Prog Orthod. 2015;16:33.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of posterior crossbite for orthodontic treatment timing. J Clin Pediatr Dent. 2016;40:422-4.
- [CrossRef] [PubMed] [Google Scholar]
- Investigation the role of midpalatal and circummaxillary sutures in bone-anchored rapid maxillary expansion using a verified finite-element model. Am J Orthod Dentofacial Orthop. 2023;163:198-209.
- [CrossRef] [Google Scholar]
- Palatal suture closure in man from 15 to 35 years of age. Am J Orthod. 1977;72:42-52.
- [CrossRef] [PubMed] [Google Scholar]
- Age-related changes in the midpalatal suture. A histomorphometric study. J Orofac Orthop. 2004;65:467-74.
- [CrossRef] [PubMed] [Google Scholar]
- Age-dependent three-dimensional microcomputed tomography analysis of the human midpalatal suture. J Orofac Orthop. 2007;68:364-76.
- [CrossRef] [PubMed] [Google Scholar]
- Palatal growth studied on human autopsy material: A histological micro-radiographical study. Am J Orthod. 1975;68:42-54.
- [CrossRef] [PubMed] [Google Scholar]
- Midpalatal suture maturation: Classification method for individual assessment before rapid maxillary expansion. Am J Orthod Dentofacial Orthop. 2013;144:759-69.
- [CrossRef] [PubMed] [Google Scholar]
- Prediction of rapid maxillary expansion by assessing the maturation of the midpalatal suture on cone beam CT. Dental Press J Orthop. 2016;21:115-25.
- [CrossRef] [PubMed] [Google Scholar]
- The cervical vertebral maturation (CVM) method for the assessment of optimal treatment timing in dentofacial orthopedics. Semin Orthod. 2005;11:119-29.
- [CrossRef] [Google Scholar]
- Diagnostic performance of skeletal maturity for the assessment of midpalatal suture maturation. Am J Orthod Dentofacial Orthop. 2015;148:1010-6.
- [CrossRef] [PubMed] [Google Scholar]
- Relationship between maturation indices and morphology of the midpalatal suture obtained using cone-beam computed tomography images. Korean J Orthod. 2016;46:345-55.
- [CrossRef] [PubMed] [Google Scholar]
- Relationship between midpalatal suture maturation and age and maturation of cervical vertebrae: Radiographic evaluation. Acta Odontol Turc. 2018;35:69-74.
- [CrossRef] [Google Scholar]
- Evaluation of midpalatal suture maturation using cone-beam computed tomography in children and adolescents. J Korean Acad Pediatr Dent. 2019;46:139-46.
- [CrossRef] [Google Scholar]
- Correlation assessment of cervical vertebrae maturation stage and mid-palatal suture maturation in an Iranian population. J World Fed Orthod. 2020;9:112-6.
- [CrossRef] [PubMed] [Google Scholar]
- Growth diagnosis: Selected methods for interpreting and predicting physical development from one year to maturity Chicago: University of Chicago Press; 1959.
- [Google Scholar]
- Transverse maxillary deficiency dentofacial deformities: Integrated orthodontic and surgical correction United States: Mosby; 1980.
- [Google Scholar]
- The relationship of rapid maxillary expansion to surgery with special reference to midpalatal synostosis. Br J Oral Surg. 1981;19:180-96.
- [CrossRef] [PubMed] [Google Scholar]
- Cone beam computed tomography evaluation of midpalatal suture maturation in adults. Int J Oral Maxillofac Surg. 2017;46:1557-61.
- [CrossRef] [PubMed] [Google Scholar]
- Classification of the midpalatal suture maturation in individuals older than 15 years: a cone beam computed tomographic study. Surg Radiol Anat. 2020;42:1043-9.
- [CrossRef] [PubMed] [Google Scholar]
- A novel classification method for midpalatal suture morphology in Indian population--A CBCT study. Indian J Public Health Res Dev. 2019;10:1749-53.
- [CrossRef] [Google Scholar]
- Midpalatal suture maturation in 11-to 15-year-olds: A cone-beam computed tomographic study. Am J Orthod Dentofacial Orthop. 2017;152:42-8.
- [CrossRef] [PubMed] [Google Scholar]
- Would midpalatal suture characteristics help to predict the success rate of miniscrew-assisted rapid palatal expansion? Am J Orthod Dentofacial Orthop. 2021;160:363-73.
- [CrossRef] [PubMed] [Google Scholar]




