

Translate this page into:
Management of skeletal Class III malocclusion with unilateral crossbite on a growing patient using facemask-bonded rapid palatal expander and fixed appliances
Address for correspondence: Dr. Tinnie Effendy, Department of Orthodontics, Faculty of Dentistry, University of Indonesia, Salemba Raya No 4, Building B-2nd floor, Jakarta 10430, Indonesia. E-mail: tinnie.effendy@gmail.com
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Facemask (FM) and bonded rapid palatal expander (RPE) are part of growth modification treatments for correcting skeletal Class III pattern with retrognathic maxilla. This orthopaedic treatment is usually preceded by fixed appliances to achieve aesthetic dental alignment and improve interdigitation. This case report reviews treatment of Class III malocclusion with unilateral crossbite in a 12-year-old boy using FM and bonded RPE, followed by fixed appliances. Choice of FM and bonded RPE was in line with indication which was mild Class III malocclusion with retrognathic maxilla. Execution of treatment was made considering treatment biomechanics and patient cooperation. This orthopaedic treatment was followed by orthodontic treatment specifically aimed to correct unilateral crossbite, canine relationship yet to reach Class I, lower midline shift, as well as unintended dental consequences of using bonded RPE, namely posterior open bite and deepening curve of spee. Posttreatment facial profile and smile are more esthetic. Occlusion is significantly improved both functionally and aesthetically.
Keywords
Bonded rapid palatal expander
Class III malocclusion
facemask
retrognathic maxilla
unilateral crossbite

INTRODUCTION
The early treatment of Class III malocclusion is one of the most challenging problem faced by orthodontists.[1] Facemask (FM) in conjunction with a rapid palatal expander (RPE) has been used to correct retrognathic maxilla and/or prognathic mandible.[2-4] However, the effectiveness of this management approach remains equivocal.[1,5] This case report demonstrates the orthodontic correction of a Class III malocclusion in an adolescent patient using FM and bonded RPE followed by fixed appliance.
CASE REPORT
A 12-year-old male patient was referred to orthodontic clinic in 2012 for the treatment of anterior crossbites. His medical histories showed no systemic diseases or developmental anomalies and no family history of mandibular prognathism. He had a prognathic profile, mild mandibular asymmetry, deviation of mandibular midlines and unilateral posterior crossbite on the left side, and Class III molar relationship. Patient was able to position his mandible in edge-to-edge bite (centric occlusion-centric relation [CO-CR] deviation). Cephalometrically, his skeletofacial types were classified as Class III with negative ANB angle [Figures 1-4]. Based on Fishman’s hand/wrist skeletal maturation indicators (SMI)[6], his SMI was at stage 4 [Figure 5].

- Pretreatment extra-oral photographs

- Pretreatment intraoral photographs

- Pretreatment lateral cephalometric radiograph

- Pretreatment panoramic radiograph

- Pretreatment hand/wrist radiograph
Treatment objectives
Maxillary protraction-growth modification.
Anterior and posterior crossbite correction.
Correct the CO-CR shift by guiding the mandible in a downward and backward position.
Correct midline shift.
Treatment alternatives
Treatment plans were discussed with the patient and his parents. The first option was to delay treatment until all permanent teeth have erupted and then use fixed appliance either passive self-ligating system or conventional bracket. The second option was to use a FM and RPE to protract maxilla, correct the crossbite, and improve facial esthetics followed by fixed appliance to adjust occlusion. Both patient and parents agreed the latter.
Treatment progress
Upper and lower alginate impressions were made, continued by a bite registration in edge-to-edge bite. A bonded RPE was fabricated in the maxilla with hooks between canine and first premolar region. A hyrax expander was soldered and a posterior bite plane was added with acrylic onto it to facilitate bite jumping. The appliance was then cemented with glass ionomer cement [Figure 6]. The patient was instructed to turn the screw a quarter every day for the 1st month. The next visit, a Petit FM (Ormco Corporation, Glendora, California) was fitted in his forehead and chin, elastic were placed in both side of the hooks. A 500 g force was directed 30° from the occlusal plane crossing the center of resistance of the maxilla [Figure 7]. Patient was encouraged to wear FM for 12 h a day. The appliance was removed after 7 months when a +3.5 mm overjet was achieved and his profile was improved.

- Bonded rapid palatal expander cementation photograph

- Petit facemask fitting photograph
After appliance removal, the upper and lower arch was directly bonded with a 0.022 conventional bracket Roth prescription slot (GAC, Dentsply) and buccal tube on the first molar. Leveling and alignment were achieved with a sequence of 0.014 and 0.016 nickel-titanium archwire. These were followed by 0.016 × 0.016 skewed lower archwire to improve asymmetric dental arch form, leading to 0.016 × 0.022 and 0.017 × 0.025 stainless steel archwire. Inter-maxillary Class II, Class III, and anterior diagonal elastics were placed after interproximal reduction on lower teeth to correct midline shift and improve interarch relationship [Figure 8]. Fixed appliances treatment took 13 months, after which essix retainer were inserted.

- Class III elastic on the right side, anterior diagonal elastic and Class II elastic on the left side
TREATMENT RESULT
Facial esthetics
The patient showed an improvement in facial esthetics. The nasolabial angle became more acute and the lower lip came backward in relation to the nose and chin. Maxillary incisor display on smiling is good, with a more symmetric face than before the treatment [Figures 9, 13 and Table 1].
| Cephalometric parameters | Mean | Before treatment | After FM + RPE | After fxed appliance |
|---|---|---|---|---|
| A-P skeletal measurement | ||||
| SNA | 82°±2 | 78° | 79.5° | 79.5° |
| SNB | 80°±2 | 81° | 78° | 78.5° |
| ANB | 2°±2 | −3° | 1.5° | 1° |
| Facial angle | 87°±3 | 84° | 81° | 83° |
| Angle of convexity | 0°±2 | −5.5° | 1.5° | 1° |
| Pg-NB | 4 mm±2 | −0.5 mm | 1 mm | 1 mm |
| Vertikal skeletal measurement | ||||
| Y-axis | 60°±6 | 65.5° | 69.5° | 68° |
| Go angle | 123°±7 | 120° | 120° | 120° |
| SN-MP | 32°±3 | 34° | 35.5° | 34.5° |
| MMPA | 27°±4 | 24.5° | 28° | 26° |
| Incisor measurement | ||||
| Interincisal angle | 130° | 131° | 127.5° | 128° |
| UI-SN | 104°±6 | 104° | 110.5° | 109° |
| UI-PP | 109°±6 | 113° | 118° | 117° |
| Ul-Apg | 4.mm±2 | 4.5 mm | 8 mm | 7 mm |
| Ll-Apg | 2 mm±2 | 9 mm | 3 mm | 3.5 mm |
| LI-MP | 90°±4 | 91.5° | 88° | 90° |
| Soft tissue | ||||
| Upper lip-E line | 1 mm | −1.5 mm | 0 mm | −2 mm |
| Lower lip-E line | 0 mm | 2 mm | 0 mm | −1.5 mm |
FM – Facemask; RPE – Rapid palatal expander

- Posttreatment extra-oral photographs
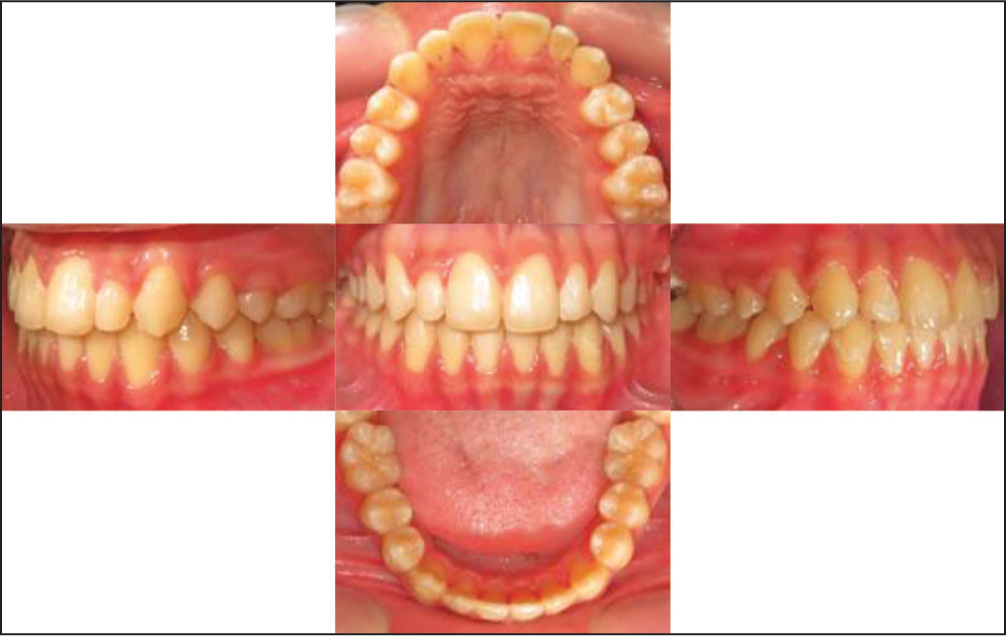
- Posttreatment intra-oral photographs

- Posttreatment panoramic radiograph
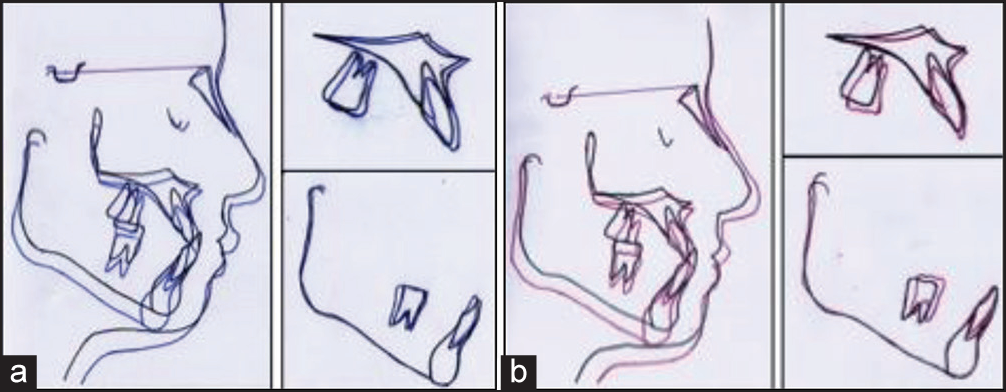
- Superimposition of pretreatment and posttreatment tracings, (a) before treatment and after facemask and bonded rapid palatal expander; (b) before treatment and after fixed appliance treatment (Black: before treatment; blue: after facemask and bonded rapid palatal expander; red: after fixed appliance)
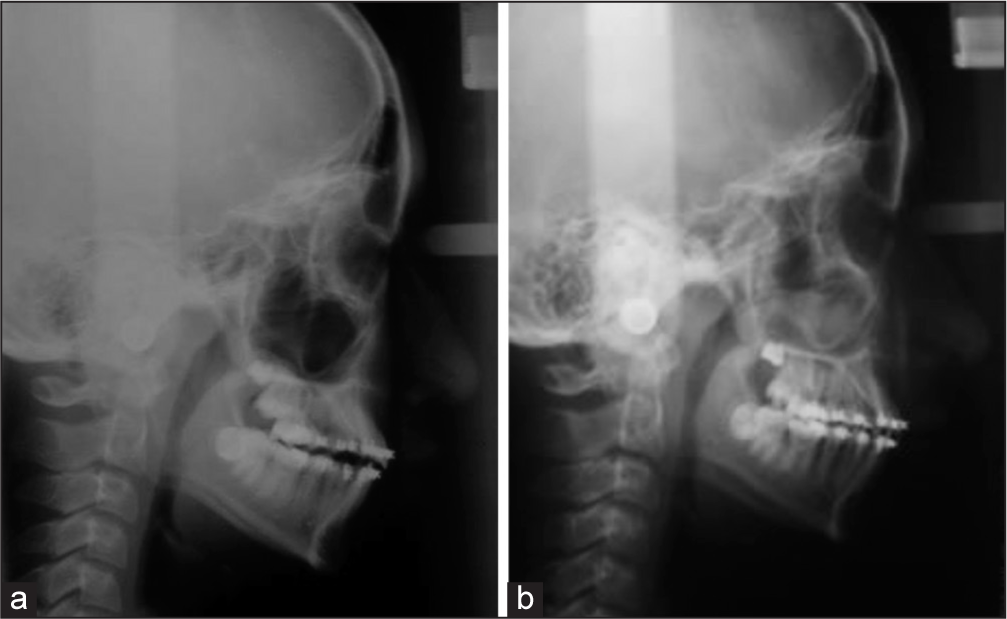
- Posttreatment lateral cephalometric radiographs, (a) after facemask and bonded rapid palatal expander treatment; (b) after fixed appliance treatment
Dentition and occlusion
Maxillary incisors were proclined and extruded. On the contrary, mandibular incisors were slightly retroclined. After first phase, molars were held from their normal eruption from occlusal force on the bonded RPE. After the second phase, maxillary molars were extruded to achieve occlusion. Class I canine and molar relationship were achieved. Moreover, anterior-posterior crossbite and midline shift were corrected. At the end of treatment, the overbite was +2.5 mm from +6 mm and overjet was +2.5 mm from −3.5 mm [Figures 10-12 and Table 1].
Skeletal
Maxilla grew in a downward and forward direction; mandible grew especially in a downward direction. SNA had changed from 78° to 79.5°, SNB from 81° to 78.5° and ANB from −3° to 1° at the end of treatment. Angle of the convexity (N-A-Pg) also increased that affected the improvement of his profile [Figures 12, 13 and Table 1].
DISCUSSION
Effect of FM and bonded RPE treatment on this patient was significant. In addition to growth and optimal treatment time, this result was achievable due to a combination of factors, such as proper execution of FM and bonded RPE biomechanics, as well as patient cooperation. Biomechanical factors considered in this treatment were direction of protraction force with respect to center of resistance of the maxilla complex, magnitude of force, and duration of force application.[5,7] Application of force is done using an elastic attached to a hook located at permanent first premolar region of the upper jaw, about 15 mm above the occlusal plane and at ±30° below the occlusal plane. The direction of this force was estimated to pass through the center of resistance of the maxilla complex to allow normal growth of maxilla downward and forward, which can be seen from upper molar translation downward and forward from superimposition of palatal vault.[7,8] The force magnitude applied in FM treatment on this patient is 500 g on each side. This magnitude was as prescribed by Cha for encouraging separation of inter-maxilla suture and stimulate growth in patients with SMI 4-7.[9] Moreover, FM was used by patient 13-15 h/day. Application of heavy intermittent force was used to induce maxilla protraction.[10]
According to information obtained from patient’s parents, patient was very cooperative in using FM and activating RPE. In addition to high patient motivation, Turley also quotes comfortable FM design as a factor inducing patient cooperation in using FM.[11] Based on this consideration, Petit-type FM was chosen over Delaire-type FM during treatment planning. This choice also considers patient’s habit of sleeping on one side. Delaire-type FM which possesses metallic supporting structure on left- and right-side of face might reduce comfort during sleep. Moreover, fitting of chin pad and forehead cap during installation of FM must also reach a position which the patient finds comfortable for day-to-day use.
In addition to the factors mentioned above, the importance of second-phase treatment with fixed appliance should also be emphasized for several reasons. One, positive effects of FM and bonded REP treatments are usually accompanied by a negative effect, namely formation of posterior teeth open bite and deepening of the curve of spee. Two, dental malocclusion present during initial examination can still be found after FM treatment. For example, posterior crossbite on the left-side and midline shift of lower incisor that were still found after treatment with FM and bonded RPE in this case.
CONCLUSION
The success of early treatment of Class III malocclusion with FM and bonded RPE can be obtained through proper consideration of treatment biomechanics and motivation to improve patient cooperation in diligently using it beside optimal treatment time and patient’s growth potential. Moreover, second phase treatment using fixed appliance may at times be important to improve dental malocclusion resulting from use of FM and bonded RPE as well as dental malocclusions present prior to treatment.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- The effectiveness of protraction face mask therapy: A meta-analysis. Am J Orthod Dentofacial Orthop. 1999;115:675-85.
- [Google Scholar]
- Skeletal effects of early treatment of class III malocclusion with maxillary expansion and face-mask therapy. Am J Orthod Dentofacial Orthop. 1998;113:333-43.
- [Google Scholar]
- Orthodontic correction of a class III malocclusion in an adolescent patient with a bonded RPE and protraction face mask. Am J Orthod Dentofacial Orthop. 1999;116:177-83.
- [Google Scholar]
- The effects of maxillary protraction therapy with or without rapid palatal expansion: A prospective, randomized clinical trial. Am J Orthod Dentofacial Orthop. 2005;128:299-309.
- [Google Scholar]
- Optimal force for maxillary protraction facemask therapy in the early treatment of class III malocclusion. Eur J Orthod. 2014;36:586-94.
- [Google Scholar]
- Radiographic evaluation of skeletal maturation. A clinically oriented method based on hand-wrist films. Angle Orthod. 1982;52:88-112.
- [Google Scholar]
- Skeletal and dental considerations in orthodontic treatment mechanics: A contemporary view. Eur J Orthod. 2012;54:1-10.
- [Google Scholar]
- Skeletal changes of maxillary protraction in patients exhibiting skeletal class III malocclusion: A comparison of three skeletal maturation groups. Angle Orthod. 2003;73:26-35.
- [Google Scholar]
- Degree of stability following experimental alteration of midfacial growth with heavy intermittent force [proceedings] Proc Inst Med Chic. 1978;32:50-1.
- [Google Scholar]
- Managing the developing class III malocclusion with palatal expansion and facemask therapy. Am J Orthod Dentofacial Orthop. 2002;122:349-52.
- [Google Scholar]




