

Translate this page into:
Mittal bonded tongue thrusting appliance
Address for Correspondence: Dr. Rekha Mittal, KD Dental College, Mathura, Uttar Pradesh, India. E-mail: drrekhagarg@rediffmail.com
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
These days majority of orthodontist includes bonded molar attachment in their inventory to eliminate the discomfort of molar separation during initial appointment and band spaces left at the end of treatment. This article describes a innovative and economical method of attachment of bonded tongue crib if required during the initial or later stages of treatment along with bonded molar tubes.
Keywords
Bonded tongue crib
habit breaking
lingual button

INTRODUCTION
Majority of present fixed orthodontic mechanotherapy includes bonded molar attachments rather than bands as it eliminates the discomfort of molar separation and also the need for a molar band inventory.[1] Bonded molars have shown less plaque accumulation, gingival inflammation, and interproximal attachment loss than banded molars in both adults and adolescent.[2,3] On the other hand, banded teeth have shown adverse changes in gingival flora and evidence of unfavorable periodontal response, especially in periodontal compromise patient.[4,5] Bonded habit breaking attachment for tongue thrusting and thumb sucking if required at initial or later stages of treatment can be used along with bonded molar tubes thereby eliminating the need of molar bands. This article describes a bonded habit breaking attachment and its applications in orthodontic treatment.
After initial impression making and pouring, bondable lingual button is closely contoured and conformed to the lingual surface of maxillary molars on the working model. Habit breaking wire component which includes tongue crib made in 20 gauge stainless steel [Figures 1 and 2] is placed over the lingual button [Figure 3] and composite is placed to seal the wire component with lingual button. Lingual button is microetched at the chairside immediately before bonding to enhance its retention and bond strength. Once adequate isolation is achieved, etching and sealing of lingual surface of upper molars followed placement of habit breaking attachment with Transbond XT resin (3M Unitek, Monrovia, CA, USA) [Figure 4]. Appliance must be attached adequately by steel ligature to the main archwire, which is cinched back wherever possible after its placement to reduce the risk of accidental ingestion. Dental floss should also be attached to habit breaking attachment during bonding to avoid accidental aspiration or swallowing during its manipulation in the patient’s mouth.[6]
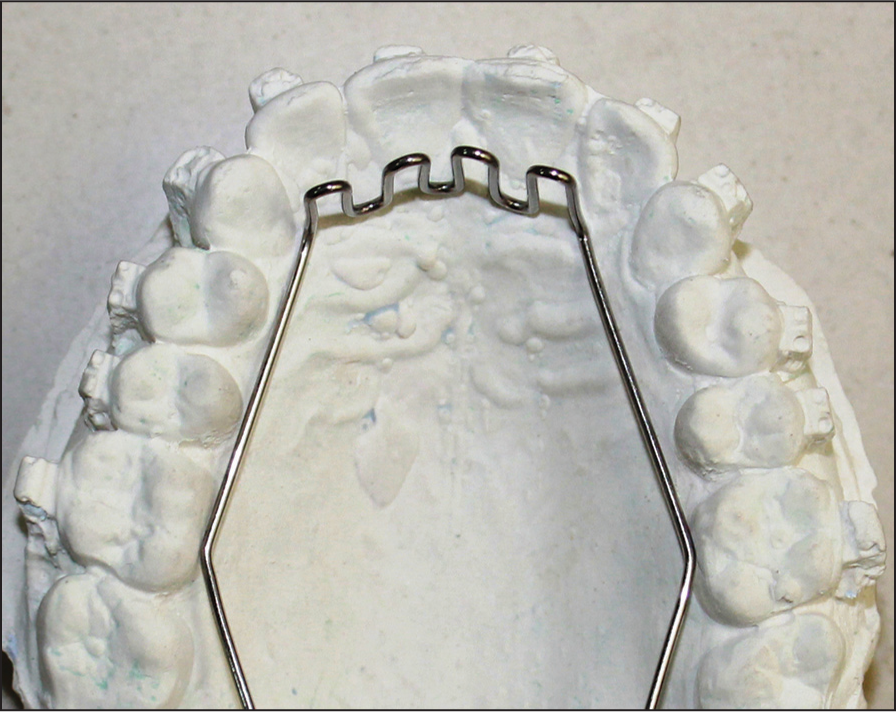
- Tongue crib made with 20 gauge stainless steel wire

- Tongue crib adapted over lingual button

- Bondable tongue crib

- Intraoral photograph showing bonded tongue crib
Source of Support:
Nil.
Conflict of Interest:
None declared.
References
- A technique for direct bonding of orthodontic attachments. J Clin Orthod. 1972;6:681-9.
- [Google Scholar]
- Recent advances in bonding to gold, amalgam, and porcelain. J Clin Orthod. 1993;27:661-75.
- [Google Scholar]
- Changes in gingiva and gingival flora with bonding and banding. Angle Orthod. 1987;57:271-8.
- [Google Scholar]
- Periodontal considerations in the use of bonds or bands on molars in adolescents and adults. Angle Orthod. 1992;62:117-26.
- [Google Scholar]
- Long-term changes in microbiology and clinical periodontal variables after completion of fixed orthodontic appliances. Orthod Craniofac Res. 2014;17:49-59.
- [Google Scholar]
- Laryngeal impaction of an archwire segment after accidental ingestion during orthodontic adjustment. Am J Orthod Dentofacial Orthop. 2012;142:264-8.
- [Google Scholar]




