

Translate this page into:
MK Versatile spring: A Novel approach for intraoral maxillary molar distalization
Address for correspondence: Dr. Manish Kumar Gupta, Department of Orthodontics and Dentofacial Orthopedics, Rungta College of Dental Sciences and Research, Bhilai - 490 024, Chhattisgarh, India. E-mail: drmanish3186@gmail.com
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Molar distalisation is method of choice for gaining space in mild crowding cases as well as non-extraction treatment of patients having Class II Div 1 malocclusion. Through this paper we present a clinical innovation “MK” versatile spring for efficient tooth distalisation and mesialiation by inter-changing the positon of the helices. “MK” spring is made by 0.017˝ × 0.025˝ TMA wire in “M” configuration. It consists of 2 helices, one at the central arm and the other at the arm close to the tooth being mesialized or distalized. The helices are 2 mm in diameter and the length of the arm is 6 mm. The article presents 2 case reports where the effictiveness and efficiency of “MK” spring have been highlighted.
Keywords
Class II malocclusion
molar distalization
non-extraction treatment

INTRODUCTION
Various appliances have been used for distalization of molars either for correction of Class II molar relation or regaining the space lost due to the mesial migration of permanent first molars. Early loss of permanent teeth due to pathological or any other iatrogenic causes preclude the development of normal intra-arch as well as an inter-arch relationship which requires movement of migrated teeth to their respective position either by removable or fixed appliances. This may be time consuming and expensive.
Treatment of Class II malocclusions, without extractions, frequently requires distalization of maxillary molars into Class I relationship by means of extra- or intra-oral forces.[1] For many years, asymmetric headgear was used routinely for the unilateral distalization of maxillary molars.[2-4] It has, however, been shown that such a force delivery system unavoidably contains a lateral component which can result in a posterior cross-bite.[5] Another disadvantage of headgear treatment is the need for patient compliance which is sometimes difficult or impossible to obtain.[6]
Problems related to patient compliance have led many clinicians to prefer intra-oral distalizing systems that minimize dependence on the patient and are under the orthodontist’s control. These intra-oral devices consist schematically of an anchorage unit (usually comprising premolars or deciduous molars and an acrylic Nance button) and an active unit. Various force-generating devices for molar distalization have been proposed, including repelling magnets, coil springs on continuous archwire, superelastic nickel-titanium archwires, coil springs on a sectional archwire (Jones Jig, Distal Jet, and Keles Slider), springs in beta titanium molybdenum alloy (TMA) (pendulum, pendulum with distal screw, K-loop, and intra-oral bodily molar distalizer), and vestibular screws combined with palatal nickel-titanium coil spring (first class) appliances.[7]
The main disadvantages of intra-oral distalizing appliances are that they produce undesirable tipping of the maxillary molars and loss of anterior anchorage during distalization.[1]
To overcome these disadvantages, a new appliance – “MK” versatile spring was designed. This paper describes “MK” versatile spring which can be used for space regaining as well as distalization of molars.
Appliance design
“MK” spring is made from 0.017˝ × 0.025˝ TMA wire in a “M” configuration [Figure 1]. It consists of two helices, one at the central arm, and the other at the arm close to the tooth being mesialized or distalized. The helices are 2 mm in diameter, and the length of the arm is 6 mm. Spring is engaged on the teeth from both buccal and palatal sides into the lingual sheath (0.036˝ × 0.072˝ ). In case of distalization of molars, Nance button is fabricated to aid in the anterior anchorage.
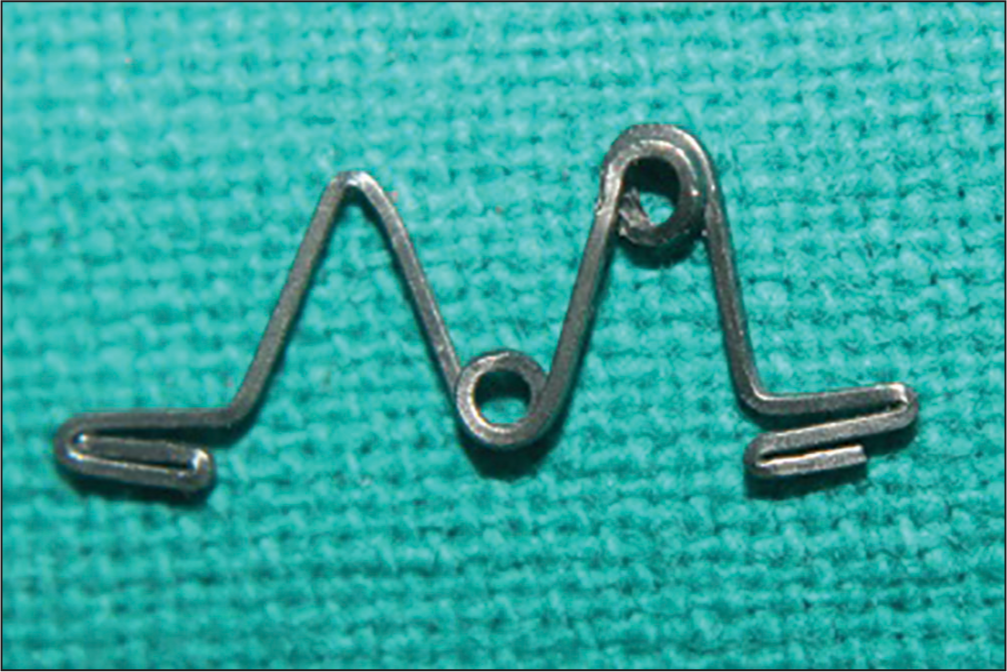
- “MK” spring made of 0.017˝ × 0.025˝ titanium molybdenum alloy wire
Appliance activation
Spring is activated by opening both the helices by 1 mm every 4-6 weeks till the desired teeth movement is achieved [Figure 2].

- Nonactivated and activated form of “MK” spring
Biomechanics
Distalizing force exerted by spring was 60 g/spring upon 1 mm of activation. Total distal force on molar was 120 g. Bodily movement of teeth is achieved by opening both the helices placed opposite to each other. The counter-clockwise tipping moment created by helix on the first arm is canceled out by the clockwise moment created by the helix of the central arm, preventing the tipping movement [Figure 3a]. As the force is applied from both buccal and palatal sides, it will prevent any unwanted rotation of teeth in the transverse plane during the treatment [Figure 3b].

- Mechanism of action (a) in sagittal plane (b) in transverse plane
CASE REPORTS
Case 1
A 20-year-old female patient visited the OPD Department of Orthodontics for adjunctive orthodontic treatment for prosthetic rehabilitation (implant supported prosthesis) of missing maxillary right second premolar. Maxillary right second premolar had been extracted 1-year back due to extensive dental caries.
Clinical examination
Extra-oral examination revealed that she had a mesoprosopic face with a straight profile and competent lips [Figure 4].

- Pre-treatment extra-oral photograph – profile view
Intra-orally, she had midline diastema and spacing of 3 mm between her maxillary right canine and first premolar due to the migration of tooth distally [Figure 5a and b].
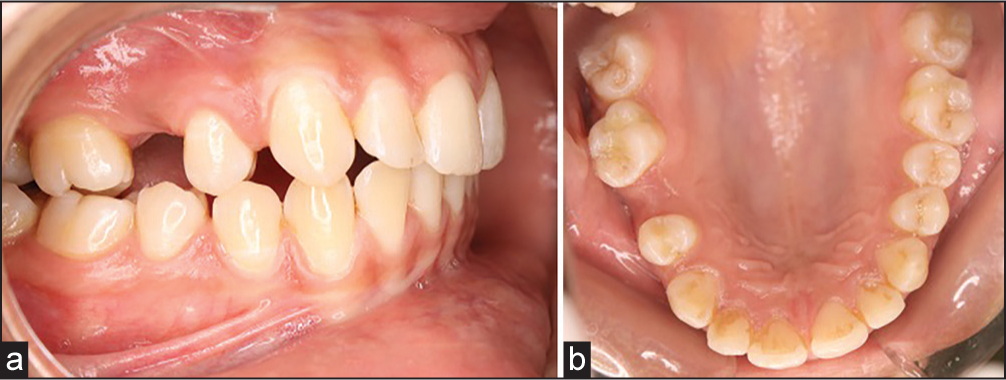
- (a) Intra-oral photograph – right lateral. (b) Intra-oral photograph – right lateral maxillary occlusal view
Treatment plan
The patient was only concerned regarding the prosthetic replacement of missing tooth, so it was decided to mesialize the first premolar with “MK” versatile spring and regain space for implant supported prosthesis.
Treatment
“MK” versatile spring was fabricated chairside as described earlier to mesialize the premolar. The mesial and distal arms of the spring were engaged to the lingual sheaths of the first premolar and first molar on buccal and palatal sides. Spring was activated by opening both the helices by 1 mm [Figure 6a-c]. After 2 months of activation, the desired space for prosthesis was gained [Figure 7a and b].
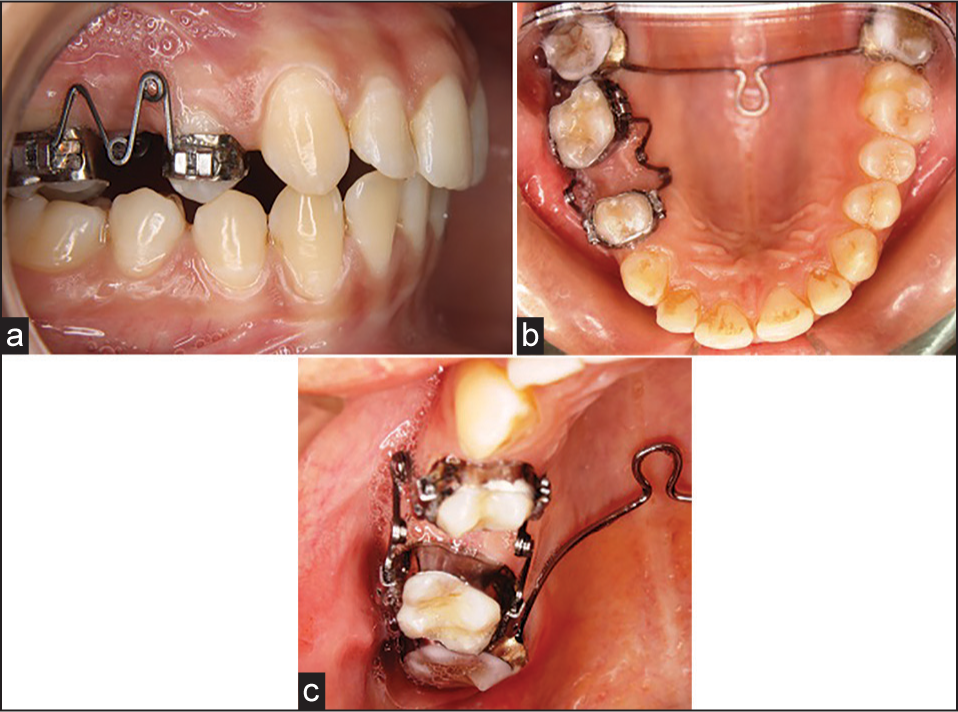
- (a) “MK” spring on the day of placement – right lateral. (b) “MK” spring on the day of placement – maxillary occlusal view. (c) “MK” spring on the day of placement – maxillary occlusal view (close up)

- (a) Intra-oral photograph at the end of treatment – right lateral. (b) Intra-oral photograph at the end of treatment – occlusal view
Radiographic evaluation
Intra-oral periapical revealed that the roots of the maxillary right first premolar was upright and parallel to adjacent teeth, having sufficient space for the placement of implant between the roots of the first premolar and the first molar [Figure 8a-c]. In the space gained, implant supported prosthesis was placed successfully [Figure 9].
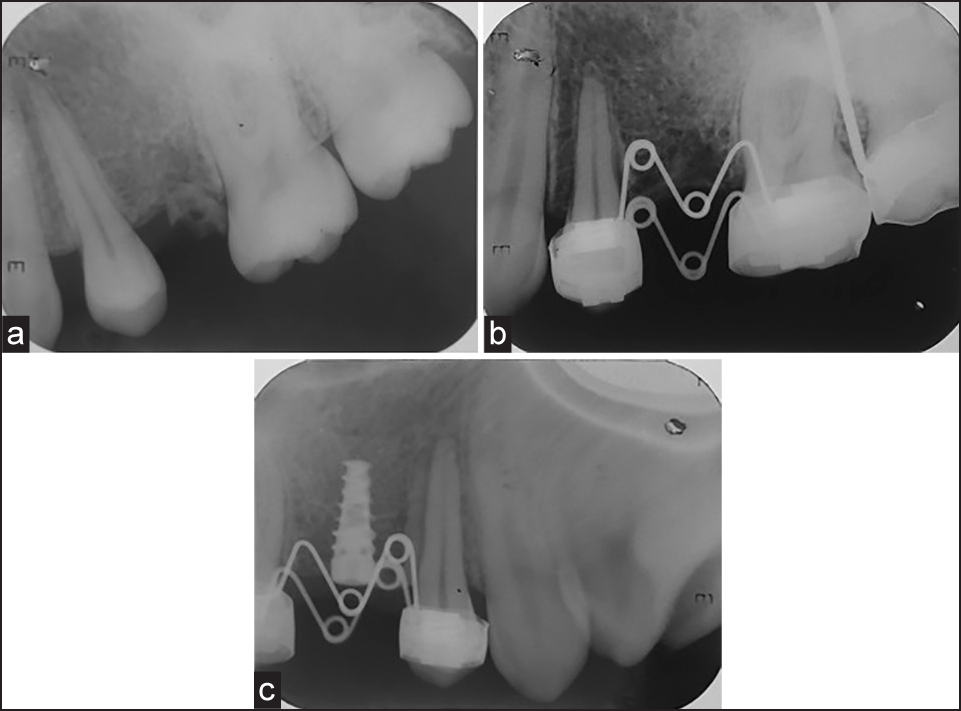
- (a) Pretreatment intra-oral periapical. (b) Posttreatment intra-oral periapical. (c) Postimplant placement intra-oral periapical

- Lateral view – after placement of implant supported prosthesis
Case 2
A 13-year-old girl reported to the Department of Orthodontics with the chief complaint of irregularly placed teeth.
Clinical examination
Extra-oral examination revealed that she had a mesoprosopic face, straight profile, and competent lips [Figure 10].
- Pretreatment extra-oral photographs
Intra-orally, moderate maxillary (6 mm) and mild mandibular (3 mm) crowding was present with angle’s Class I molar relation on the right side and end on molar relation on the left side. She had an overjet of 4 mm and overbite of 4.5 mm [Figure 11].

- Pretreatment intra-oral photographs
Treatment plan
Considering the patient’s straight profile with normal nasolabial angle, it was decided to treat the case as nonextraction by distalizing maxillary left molar to gain the space for relieving the crowding and simultaneously to achieve angle’s Class I molar relation on left side.
Treatment
“MK” spring was fabricated and placed on the first molar and second premolar with helix placed close to the molar tooth. Nance button was placed as an anchorage unit. Mesial and distal arms were engaged to the lingual sheath to deliver the force to distalize the molar [Figure 12a]. Spring was activated by 2 mm on the day of placement and later 1 mm/month by opening both the helices. 7 mm of space was gained in a period of 5 months [Figure 12b and c].
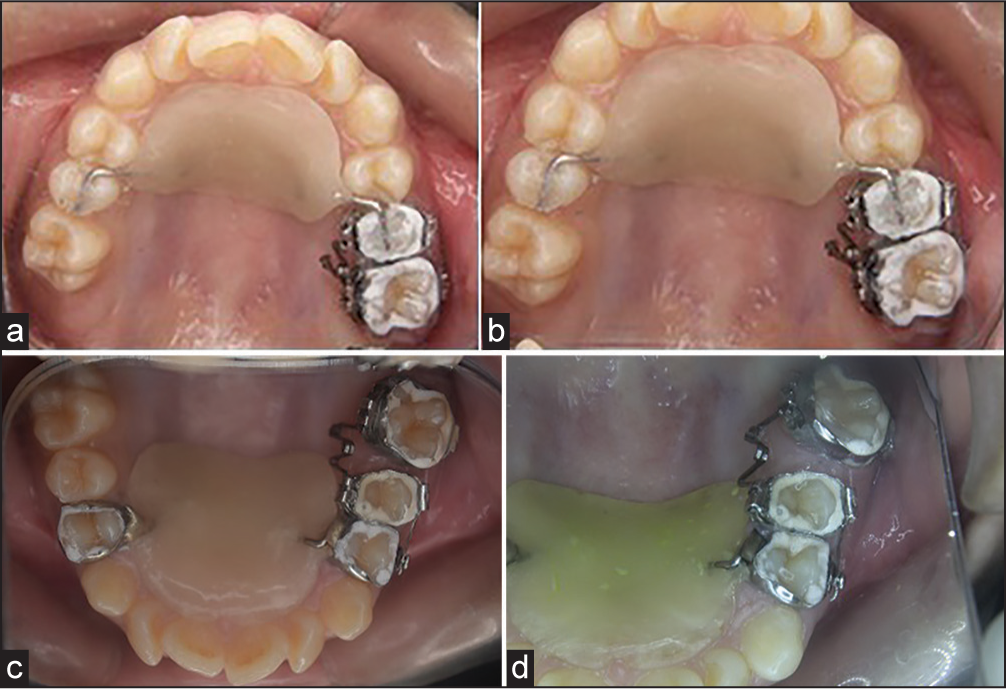
- (a) Intra-oral photographs maxillary occlusal view – on the day of appliance placement. (b) Maxillary occlusal view – 1-month later. (c) Maxillary occlusal view - 3 months later
Leveling and alignment of the maxillary arch were started postdistalization, once the desired amount of space was gained. Figure 13 shows Angle’s class I molar relationship on left side post-distalization after leveling and alignment.

- Postdistalization intra-oral photographs
Figure 14 shows comparison of pre and post distalization molar relationship.

- Pre- and post-distalization maxillary left lateral view
Post treatment lateral cephalogram was taken to evaluate the efficiency of MK spring [Table 1].
| Parameter | Pretreatment | Posttreatment |
|---|---|---|
| Upper 1 to NA (angle) | 37° | 27° |
| Upper 1 to NA (linear) | 4 mm | 5 mm |
| Upper 1 to SN | 106° | 113° |
| Interincisal angle | 122° | 117° |
| Lower 1 to NB (angle) | 31° | 30° |
| Lower 1 to NB (linear) | 5 mm | 6 mm |
DISCUSSION
The intra-oral molar distalization appliances are an excellent substitute for patients who are noncompliant to wear headgear. “MK” spring is made up of 0.017˝ × 0.025˝ beta titanium (TMA) wire. It produces less than half the force when compared to the one made with stainless steel and can be activated twice as much as stainless steel before it undergoes permanent deformation. It also provides constant distal force near the center of the resistance of molar, thus, reducing the moment of force. Kalra’s K-loop and Karad’s Integrated Distalizing System (KIDS) are other appliances used to distalize molars which utilize the properties of TMA wire.[8,9] The KIDS consists of two gingivally positioned helices and one occlusally positioned helix.[9]
“M” configuration of spring helps to deliver constant force near the center of resistance of teeth. By changing the position of the helices, the amount of force delivered on the teeth can be altered. The helix which is close to the tooth to be moved provide flexibility to the spring and also provide ease for activation, thus, deliver a low continuous force. On the side of the anchor tooth, the arm of the spring is made without any helix, thus, a rigid arm of the spring is difficult to activate and also does not deliver force on anchor tooth.
“MK” versatile spring is engaged on both the buccal and palatal side, thus, prevents the unwanted rotation of molar during distalization associated with other method of distalization like with pendulum appliance. It provides bodily movement of teeth with better control in all the dimensions.
“MK” versatile spring has following advantages:
Simple yet efficient.
Easy to fabricate chairside and place.
It produces constant and parallel forces.
Unwanted rotation of molar was prevented as forces were applied from both buccal and lingual aspect.
Hygienic and comfortable for the patient.
Requires minimal patient cooperation.
Low cost.
CONCLUSION
Treatment with “MK” versatile spring provides an efficient and effective way to distalize the molars. Force applied on tooth can be controlled by altering the position of the helices, and this can also reduce the reciprocal force on anchor tooth.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Molar distalization with a pendulum appliance K-loop combination. Eur J Orthod. 2010;32:459-65.
- [Google Scholar]
- The mechanics of centric and eccentric cervical traction. Am J Orthod Dentofacial Orthop. 1958;44:236-57.
- [Google Scholar]
- Unilateral headgear: Lateral forces as unavoidable side effects. Am J Orthod. 1980;77:333-40.
- [Google Scholar]
- Nonextraction treatment of unilateral Class II, Division 1 malocclusion with asymmetric headgear. Am J Orthod Dentofacial Orthop. 1998;113:483-7.
- [Google Scholar]
- An experimental evaluation of effects and side effects of asymmetric face-bows in the light of in vivo measurements of initial tooth movements. Am J Orthod Dentofacial Orthop. 1998;113:558-66.
- [Google Scholar]
- A comparison of two intraoral molar distalization appliances: Distal jet versus pendulum. Am J Orthod Dentofacial Orthop. 2005;128:353-65.
- [Google Scholar]




