

Translate this page into:
Molar Protraction and Uprighting (2nd Molar Protraction in the 1st Molar Missing Site and Uprighting an Impacted 3rd Molar)
Address for correspondence: Dr. Un-Bong Baik, 35-5 Songjung dong Ecopia 7F, Kangbuk-ku, Seoul, Korea. E-mail: baikub222@naver.com
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Recently, with the help of TADs (temporary anchorage devices), substantial 2nd molar protraction has become possible in case of missing posterior teeth. Total 260 cases of U-6 (Upper 1st molar missing), L-6 (Lower 1st molar missing) and L-E (Lower E extraction with the 2nd molar missing, E: deciduous 2nd molar) were finished. After 2nd molar protraction, even a horizontally-impacted 3rd molar can be uprighted. This treatment will become very good treatment modality, replacing implants and bridges in cases of missing posterior teeth.
Keywords
Molar protraction
molar uprighting
third molar
1st molar missing

Introduction
Till date, there has been a lot of attention given to molar distalization while molar protraction has been left out of the discussion for the most part. Molar protraction makes orthodontic closure of missing posterior teeth possible. Recently, with the help of temporary anchorage devices (TADs) or miniscrews, substantial molar protraction has become possible, and the scope of orthodontic closure of missing posterior teeth is widening.[1-9]
There are many kinds of missing posterior teeth: U-E (upper E extraction with the 2nd bicuspid missing) (E: deciduous 2nd molar), U-6 (upper 1st molar missing), and U-7 (upper 2nd molar missing) in the upper arch; and similarly, L-E (lower E extraction with the 2nd molar missing), L-6 (lower 1st molar missing), and L-7 (lower 2nd molar missing) in the lower arch. Lower arch cases are more difficult to treat because the bone is denser in the mandible than in the maxilla. Cases of U-E are extremely rare, and cases of U-7 and L-7 are not so difficult to treat because the 3rd molar easily erupts to the 2nd molar extraction space; therefore, only minor posterior teeth movement is necessary. Accordingly, U-6, L-6, and L-E cases comprise the main theme of this article due to their degree of difficulty as they need a large amount of 2nd molar protraction and control of the 3rd molar.
After the 2nd molar protraction, even a horizontally impacted 3rd molar can be uprighted. The existing research about the 3rd molar has been about the natural 3rd molar development or its movement after 2nd molar extraction. This article is totally different because it deals with research after the 2nd molar protraction rather than extraction.
The number of cases that have been finished up to now is 260 (U-6 = 45, L-6 = 160, and L-E = 55). All of the cases presented have been treated solely by Dr. Un-Bong Baik, while the other author only contributed article writing.
If we can easily do molar protraction for closing missing posterior teeth spaces, this treatment will become very good treatment modality, replacing implants, and bridges. If we can use the 3rd molar, which used to be wasted, the significance of this treatment will become greater.
Classifications of Molar Protraction
Molar protraction can be classified as follows - by the missing area and by the amount of movement of the posterior teeth.
By the missing area
By the amount of movement of the posterior teeth
Pure retraction of anterior teeth: In practice, there are very few cases of pure retraction of anterior teeth because the mesiodistal length of the 1st molar is very long
Reciprocal traction [Figure 2a]: Many cases fall under this category
 Figure 2
Figure 2- (a) Reciprocal traction. (b) Pure protraction of the posterior teeth
Pure protraction of posterior teeth [Figure 2b]: The missing 1st molar space is closed by pure protraction of the posterior teeth. If the 1st molar were intact, these cases could be treated by nonextraction. This is the most difficult type of teeth movement because the distance to be moved is the longest.
Formation of Posterior Occlusion
In this article, the term “Class I molar relationship” has been used to describe the position of the 2nd molars that have been moved into the 1st molar location.
U-6 + L-NE (lower nonextraction): Class I molar relation [Figure 3]
 Figure 3
Figure 3- U-6 + L-NE: Final occlusion should be molar Class I relationship (canine relation: Class I)
U-6 + L-4 (lower bicuspid extraction): Class III molar relation [Figure 4]
 Figure 4
Figure 4- U-6 + L-4: Final occlusion should be molar Class III relationship (canine relation: Class I)
U-6 + L-6: Class I molar relation [Figure 5]
 Figure 5
Figure 5- U-6 + L-6: Final occlusion should be molar Class I relationship (canine relation: Class I)
U-NE + L-6: Class I molar relation [Figure 6]
 Figure 6
Figure 6- U-NE + L-6: Final occlusion should be molar Class I relationship (canine relation: Class I)
U-NE + L-E: Class III molar relation [Figure 7]
 Figure 7
Figure 7- U-NE + L-E: Final occlusion should be molar Class III relationship (canine relation: Class I)
U-4 + L-6: Class II molar relation [Figure 8]
 Figure 8
Figure 8- U-4 + L-6: Final occlusion should be molar Class II relationship (canine relation: Class I)
U-4 + L-E: Class I molar relation [Figure 9].
 Figure 9
Figure 9- U-4 + L-E: Final occlusion should be molar Class I relationship (canine relation: Class I)
Cases
U-6
A 26-year-old male. Maxillary right 1st molar missing space closed completely. Root moved parallelly [Figure 10].

- (a) Initial, (b) during treatment, (c) debonding, (d) 2 year 3 months after
L-6
A 17-year-old female. Mandibular left 1st molar missing space closed completely. Root moved parallely. Initially, the impacted 3rd molar did not develop well. At the time of debonding, the root of 3rd molar showed good development. After 7 years and 6 months, the missing space did not relapse [Figure 11].

- (a) Initial, (b) during treatment, (c) debonding, (d) 7 years 6 months after
L-E
A 16-year-old male. Mandibular right L-E space closed completely. The root of 1st and 2nd molar moved parallelly [Figure 12].

- (a) Initial, (b) during treatment, (c) debonding, (d) 2 years 4 months after
Uprighting of horizontally impacted 3rd molar
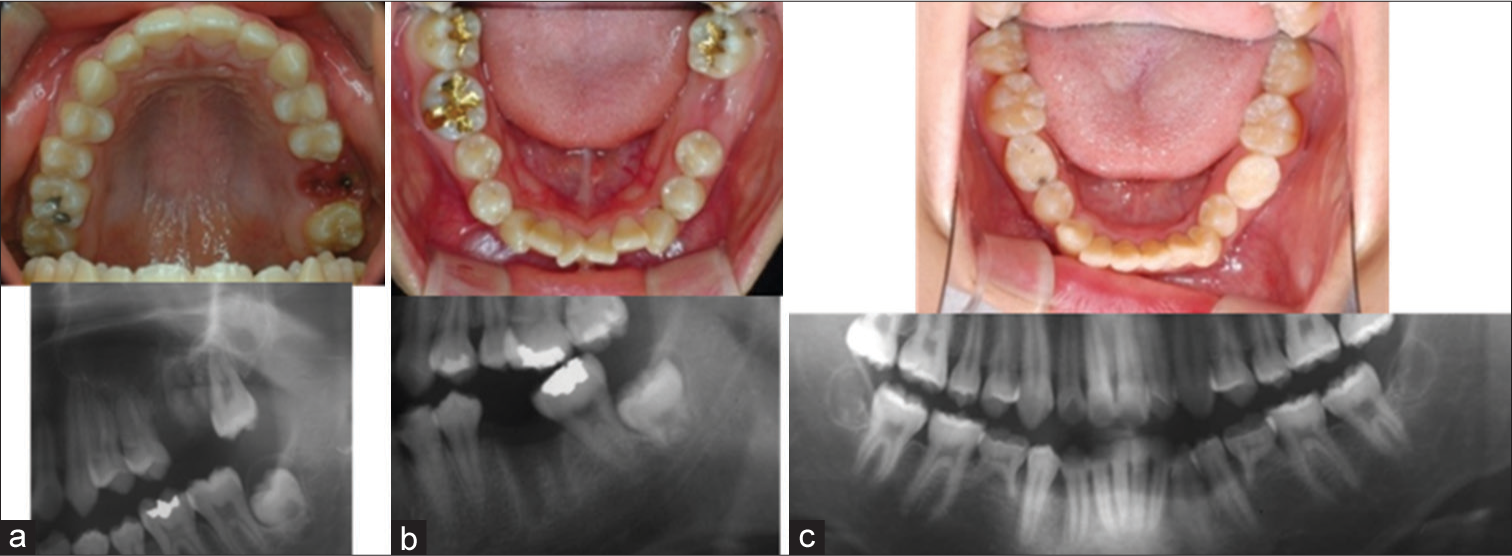
A 29-year-old female. Mandibular right 1st molar missing space closed completely. The root of 2nd molar moved parallelly. At the start of treatment, the 3rd molar was horizontally impacted. After protraction of 2nd molar and uprighting of 3rd molar, the axis of 3rd molar was arranged parallelly [Figure 13].

- (a) Initial, (b) during treatment, (c) debonding
Uprighting of horizontally impacted 3rd molar
A 22-year-old female. Left 2nd molars showed scissor bite. Mandibular left 1st molar missing space closed completely. Initially, deeply impacted 3rd molar was arranged parallelly. This case was selected as case of the month of AJODO in March 2017 [Figure 14].[8]

- (a) Initial, (b) during treatment, (c) debonding, (d) 9 months after
Closure of long missing space (#35, 36 simultaneous missing)
A 22-year-old female. Mandibular left 2nd bicuspid and 1st molar were damaged. Those teeth were extracted simultaneously. Long missing space closed successfully and roots moved parallelly. After 1 year 11 months, the missing space did not relapse. This case was published in JCO in June 2017 [Figure 15].[9]

- (a) Initial, (b) during treatment, (c) debonding, (d) 1 years 11 months after
Possible Problems and Biomechanics
Because the missing space of U-6, L-6, and L-E is long, the biggest problem is tipping. Meticulous traction and light force are important for parallel movement of the adjacent teeth.
Mesial rotation and swinging into the buccal side of the protracted molars is another problem during 2nd molar protraction [Figure 16]. It can create a posterior crossbite. To prevent this, a rigid lingual arch and a lingually placed miniscrew can be used. However, the lingual arch may not only cause discomfort to the patient but also interfere with any further movement of the protracting of the molars. In addition, the lingual arch needs to be remade when it touches the lingual side of the anterior teeth. Lingual placement of the miniscrew is very difficult due to poor visibility and accessibility. Other methods are placing an elastic chain from the lingual side of the molars to a button on the canine, or a sliding band with a lingual arch. Among the cases I have personally encountered, this problem was minimized by inserting an anti-rotation bend in the posterior portion of the archwire.

- Protraction force (B) produced buccal force (A). This swung the posterior dentition into a unilateral crossbite
During protraction, the extrusion of the posterior teeth is another problem. It causes an anterior open bite [Figure 17]. The entire arch rotates around the center of rotation of the dentition in the miniscrew retraction system. As a result, when the posterior teeth are protracted, the molars become extruded, causing an anterior open bite. To solve these problems, the following methods can be used: (1) A long hook can be attached to the second molar brackets to pass the protracting force near the center of rotation; (2) The maxillary and mandibular molar intrusion can be done by miniscrews. None of the presented cases showed these problems.

- The center of rotation of the entire arch (A) is located under the TADS (red point). Protraction of the posterior teeth caused the extrusion of the posterior tooth (B) and intrusion of the anterior teeth (C)
Among 260 cases of U-6, L-6, and L-E, 4 cases had failed. All of the failed cases were due to periodontal problems. Most of the cases did not exhibit tilting or an open bite, and only a few cases resulted in a buccal crossbite.
Development of Lower 3rd Molar
There have been so many reports about the 3rd molar. Most of them have been about normal development or movement after 2nd molar extraction.[10-17] Meanwhile, there has not been sufficient research on the eruption of the 3rd molar after 2nd molar protraction. The reason is that TADs is essential for molar protraction, but they have only been utilized in the past 10–15 years.
The number of cases of U-6, L-6, and L-E that have been finished up to now is 260. Among them, the number of cases that had an impacted 3rd molar at the time of the start of treatment was 100. Using these materials, many new research studies are possible. At first, studies about the vertical eruption patterns of impacted mandibular third molars after protraction of 2nd molars were done and published in Angle Orthodontists in 2016.[18] It showed most impacted mandibular third molars spontaneously erupt after 2nd molar protraction without any appliances, even in adults. Even in such cases where the root formation was slightly insufficient at the initial stage, the root developed well, and the tooth erupted [Figure 18]. Among the adults as well, after root development was complete, the 3rd molar also erupted well in most of the cases. In that research, age, gender, Nolla stage, and angle of the third molars did not show significant correlations with the vertical change of the impacted third molars, whereas the depth of third molar impaction and available space showed significant correlations.

- 18 years old female (a) Initial, (b) During treatment, (c) Debonding, (d) 5 years 8 months after
Now, more research is being done about angular change, horizontal movement, and alveolar bone changes.
A 17-year-old female. Mandibular left 1st molar missing space closed completely. Root moved parallelly.
Evaluation
Till date, 260 cases of U-6, L-6, and L-E have been finished, out of which only four L-6 cases have failed. The reason for failure was mainly due to periodontal problems. In the future, more meticulous case selections and periodontal therapy will decrease the rate of failure.
When there are missing teeth, bridges or implants have been the traditional treatment method; however, orthodontic space closure is another good option. Some patients may choose orthodontic treatment despite the lengthy treatment time. If bridges or implants have been applied previously, orthodontic treatment becomes very complex and difficult. Accordingly, when there are missing teeth, orthodontic evaluation is the top priority.
Prosthodontic, endodontic, or periodontic doctors may have more chances to meet patients who have missing teeth than orthodontic specialists do. Therefore, not only orthodontists but also the other dental doctors should take this orthodontic treatment into consideration. Moreover, patients, as well as dentists, must be aware of various treatment options, including orthodontic treatment methods.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Rigid implant anchorage to close a mandibular first molar extraction site. J Clin Orthod. 1994;28:693-704.
- [Google Scholar]
- Miniscrew anchorage used to protract lower second molars into first molar extraction sites. J Clin Orthod. 2003;37:575-9.
- [CrossRef] [Google Scholar]
- Titanium screw anchorage for protraction of mandibular second molars into first molar extraction sites. Am J Orthod Dentofacial Orthop. 2008;134:583-91.
- [Google Scholar]
- Mandibular molar protraction with temporary anchorage devices. J Clin Orthod. 2008;42:351-5.
- [Google Scholar]
- Protraction of mandibular second and third molars into missing first molar spaces for a patient with an anterior open bite and anterior spacing. Am J Orthod Dentofacial Orthop. 2012;141:783-95.
- [CrossRef] [PubMed] [Google Scholar]
- Molar Protraction: Orthodontic Substitution of Missing Posterior Teeth. Charleston, SC, USA: CreateSpace; 2013.
- Temporary Skeletal Anchorage Devices: A Guide to Design and Evidence-Based Solution. Heidelberg, Germany: Springer; 2014. p. :119-60.
- [CrossRef]
- Orthodontic uprighting of a horizontally impacted third molar and protraction of mandibular second and third molars into the missing first molar space for a patient with posterior crossbites. Am J Orthod Dentofacial Orthop. 2017;151:572-82.
- [Google Scholar]
- Correction of bimaxillary protrusion after extraction of hopeless mandibular posterior teeth and molar protraction. J Clin Orthod. 2017;51:353-9.
- [Google Scholar]
- Second molar extraction in orthodontic treatment. Am J Orthod. 1977;72:599-616.
- [CrossRef] [Google Scholar]
- Effects on lower third molars after extraction of second molars. Angle Orthod. 1977;47:55-8.
- [Google Scholar]
- Clinical experience with third molar orthodontics. Am J Orthod Dentofacial Orthop. 1989;96:453-61.
- [Google Scholar]
- Late lower arch crowding: The effect of second molar extraction. Am J Orthod Dentofacial Orthop. 1990;98:242-6.
- [Google Scholar]
- Lower third molar development subsequent to second molar extraction. Am J Orthod Dentofacial Orthop. 1993;104:566-74.
- [CrossRef] [PubMed] [Google Scholar]
- Eruption of third permanent molars after the extraction of second permanent molars. Part 2: Functional occlusion and periodontal status. Am J Orthod Dentofacial Orthop. 2001;119:239-44.
- [Google Scholar]
- Spontaneous third-molar eruption after second-molar extraction in orthodontic patients. Am J Orthod Dentofacial Orthop. 2006;129:337-44.
- [Google Scholar]
- Effects of early loss of permanent first molars on the development of third molars. Am J Orthod Dentofacial Orthop. 2006;130:634-8.
- [CrossRef] [PubMed] [Google Scholar]
- Vertical eruption patterns of impacted mandibular third molars after the mesialization of second molars using miniscrews. Angle Orthod. 2016;86:565-70.
- [Google Scholar]




