

Translate this page into:
Molar space closure: To do or not to do?
*Corresponding author: Chung-Chen Jane Yao, Department of Orthodontics and Dentofacial Orthopedics, Graduate Institute of Clinical Dentistry, National Taiwan University, Taipei, Taiwan. janeyao@ntu.edu.tw
-
Received: ,
Accepted: ,
How to cite this article: Ratanasereeprasert N, Weng C, Yang SY, Chen Y, Yao CJ. Molar space closure: To do or not to do? APOS Trends Orthod 2022;12:61-8.
Abstract
Missing or compromised permanent molars can complicate orthodontic treatment planning and mechanics. Molar extraction should be considered in appropriate situations, but clinicians must decide between closing and regaining the edentulous space. Several factors should be taken into consideration to achieve appropriate molar space management, such as the need for space, asymmetry, periodontal status, sinus pneumatization, and the terminal molar position. Herein, three sample cases are reported to demonstrate the treatment options for molar space closure and maintenance with these factors taken into consideration during treatment planning. The understanding of mechanics played a crucial role in anchorage preparation and side effect prevention. If the third molar substitution was managed in advance and adequate space between the ramus and third molar was obtained via second molar protraction, the tooth spontaneously erupted in a favorable position without requiring further treatment. This case series can aid clinicians in molar space management. Regardless of whether the space is to be closed or regained, the treatment plan should conform to the patient’s expectations and improve occlusion with minimal side effects and treatment duration.
Keywords
Molar space closure
Diagnosis and treatment planning
Edentulous space management

INTRODUCTION
First molars are the most commonly lost teeth owing to their high susceptibility to caries, which is related to early eruption, anatomical features, and the posterior location in the oral cavity.[1] Approximately 60% of adult patients have lost at least one first molar, which is the highest prevalence compared to other teeth.[2] The consequences of missing first molars are the tipping and drifting of adjacent teeth, supra-eruption of opposing teeth, narrowing of the alveolar ridge, and formation of bone defects on the mesial side of the second molars.[3] Therefore, effective treatment is needed to restore periodontal health and occlusion.
One of the treatment options for missing molars is fixed prosthodontic bridges or implants that replace the missing natural teeth. Orthodontic space closure of edentulous sites is an alternative treatment option that patients prefer because the procedure helps eliminate the need for restoration, preserve natural healthy teeth, and reduce treatment fees. However, molar space closure is a challenging process in orthodontics, particularly in adult patients; it is more technically complex because of the large space to be closed within the narrow alveolar ridge, and tooth movement is slower than in younger patients.[4] Furthermore, anchorage is critical, particularly in cases requiring prolonged treatment time, because it provides greater control of orthodontic mechanics to reduce unwanted tooth movement during space closure.[5]
Attempting space closure via protraction of molars into edentulous sites without anchorage reinforcement bears the risk of anchorage loss, thereby leading to compromised occlusion. Consequently, temporary skeletal anchorage devices (TSADs) have been introduced to the field of orthodontics as effective tools for providing absolute anchorage for molar movement.[6-8] Another consideration is whether to close the first or second molar space; the morphology of third molars is critical because they will also be protracted forward. Hence, cone-beam computed tomography must be included in the treatment plan to investigate the morphology and location of the third molar to determine whether the second molar should be moved instead.
Because closing the molar space is not appropriate in every case, this article reports three patients who had at least one molar space that needed treatment for hopeless molars or edentulous spaces resulting from previous molar extraction, and the factors that should be thoroughly considered during treatment planning to achieve successful results.
PATIENTS AND TREATMENT MODALITIES
Case 1
Case characteristics
A 22-year-old male patient sought orthodontic treatment to close the space resulting from the extraction of a hopeless mandibular left first molar. He had skeletal Class I malocclusion with a high mandibular plane angle. The pre-treatment records showed anterior crowding, midline deviation to the right, a hopeless mandibular left first molar, and a mesially tipped mandibular left second molar.
Treatment plan
The mandibular left first molar was extracted and the space was closed via reciprocal force to relieve anterior crowding and to the protract mandibular left second and third molars.
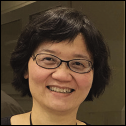
In this case, closing the mandibular left first molar was appropriate because of moderate crowding in the mandibular arch, a midline shift to the opposite side of the protracting molars, and a Class III canine and molar relationship on the space closure side. In addition, because the patient was young and the extraction socket was fresh, bone remodeling was expected to be favorable. Nevertheless, the angulation of the mandibular left second molar was not suitable for protraction, and the mechanics of uprighting the second molar made the protraction more difficult to achieve. Consequently, during mid-treatment, the dental midline was deviated to the left with a Class II canine and molar relationship on the left side. Midline elastics and Class II elastics were used to correct the malocclusion. Appropriate occlusion was achieved with bilateral molar and canine Class I relationships. The treatment records are presented in [Figure 1].

- Case 1: (a) Initial records; (b) Mid-treatment records, metal brackets (Ormco, CA, USA) with 0.018-in slots for the anterior teeth and 0.022-in slots for the posterior teeth. The initial wires were 0.016-in NiTi and 0.016 × 0.022-in NiTi, the working wire was 0.016 × 0.022- in SS, and the finishing wire was 0.017 × 0.025-in TMA; (c) Post-treatment records.
Case 2
Case characteristics
A 35-year-old female patient presented to our clinic with dental crowding and crossbite. She had skeletal Class III malocclusion with a high mandibular plane angle. The pretreatment records showed a narrow maxillary arch, posterior crossbite, midline deviation, multiple fixed dental prostheses, and a hopeless mandibular right first molar.
Treatment plan
Starting with transverse correction, palatal expansion was performed using a NiTi (nickeltitanium) palatal expander. The edentulous space at the maxillary right first molar was maintained, whereas the space at the maxillary right lateral incisor was regained to improve the morphology of the prosthesis. The mandibular right first molar was extracted and the space was closed via reciprocal force to correct the mandibular midline and protract the mandibular right second and third molars.
In this case, space closure was appropriate at the mandibular right first molar but not at the maxillary right first molar. Reciprocal space closure at the mandibular right first molar was an appropriate option because the mandibular midline was shifted to the left with a Class III canine and molar relationship on the right, the mandibular right second and third molars were positioned with favorable angulation, and the extraction wound was fresh. Conversely, the space at the missing maxillary right first molar was maintained for a future prosthesis because it was a healed wound and the position of the maxillary right third molar was not suitable for protraction. In addition, because the maxillary arch was narrow, palatal expansion was needed to correct posterior crossbite. However, the expansion increased the edentulous space and impeded space closure. Because the miniscrew-assisted rapid palatal expander was not available at that time, a NiTi palatal expander and posterior cross elastics were used to correct the transverse discrepancy. Hence, palatal expansion was achieved via dental movement during mid-treatment and buccal tipping of the posterior teeth was observed. Buccal root torque was applied to the maxillary posterior teeth. Although posterior crossbite was not completely corrected at the end of treatment, the patient was satisfied with the results. The treatment records are presented in [Figure 2].

- Case 2: (a) Initial records; (b) Mid-treatment records, metal brackets (Ormco, CA, USA) with 0.018-in slots for the anterior teeth and 0.022-in slots for the posterior teeth. The initial wires were 0.016-in NiTi and 0.016 × 0.022-in NiTi, the working wire was 0.016 × 0.022- in SS, and the finishing wire was 0.017 × 0.025-in TMA; (c) Post-treatment records.
Case 3
Case characteristics
A 49-year-old female patient presented for orthodontic treatment for malaligned teeth. She had skeletal Class I malocclusion with an average mandibular plane angle. The pretreatment records showed a narrow edentulous ridge, multiple fixed dental prostheses, sinus pneumatization, and generalized chronic periodontitis.
Treatment plan
The maxillary right second premolar was extracted and the extraction space was closed along with the edentulous space at the maxillary left first molar via moderate anchorage. The space at the mandibular left first molar was closed via reciprocal force, but the atrophic edentulous space at the mandibular right posterior area was maintained for a prosthesis.
In this case, large space closure was not appropriate because of the patient’s age and periodontal status. Furthermore, all three edentulous spaces had anatomical limitations, such as large sinus pneumatization at the maxillary left first molar extraction space, mesial crown tipping of the mandibular left second molar, and a long narrow alveolar ridge at the mandibular right posterior edentulous space with mesial crown tipping of the mandibular right third molar. Because the patient was concerned about dental protrusion and expected minimal prosthetic replacements, space closure was performed to reduce the protrusion and the need for prostheses, except for the atrophic edentulous space in the mandibular right posterior area, which was maintained. During mid-treatment, left deviation of the mandibular dental midline was noted as a side effect of unilateral space closure. Left Class II elastics were used to correct the deviation. Favorable occlusion was obtained and the mandibular right edentulous space was restored using dental bridges. The treatment records are presented in [Figure 3].
- Case 3: (a) Initial records; (b) Mid-treatment records, clear brackets (Tomy, Tokyo, Japan) with 0.018-in slots for the anterior teeth and 0.022-in slots for the posterior teeth. The initial wires were 0.016-in NiTi and 0.016 × 0.022-in NiTi, the working wire was 0.016 × 0.022- in SS, and the finishing wire was 0.017 × 0.025-in TMA; (c) Post-treatment records.
DISCUSSION
Considerations when closing molar spaces
Space needed
The simplest method of closing a large space is to use reciprocal force to move anterior teeth backward and move posterior teeth forward. Hence, molar space closure is appropriate in cases of anterior protrusion or crowding.[9,10] If the incisor position is favorable and only pure molar protraction is needed, the treatment time will be lengthened and side effects such as the tilt and rotation of molars are likely.
Alveolar ridge and extraction socket
The rate of alveolar bone resorption is highest during the first several months to 2 years after extraction but decreases thereafter. The amount of post-extraction resorption is far greater on the buccal than on the lingual side in both arches.[11] During the 1st year after tooth extraction, the amount of resorption in the mandible is twice that in the maxilla, and the ratio increases to 4:1 after 7 years.[12] Long- term absence of teeth can cause the cortical bone plate of the buccal or lingual alveolar bone to collapse, thereby impeding the posterior teeth from moving forward across it or causing them to move the surrounding bone with them. Although the teeth can be forcibly pulled toward the shrinking ridge, this may result in the loss of periodontal attachment, root resorption, increased tooth mobility, and even the loss of pulp vitality.[13] Consequently, tooth movement toward a fresh extraction socket is faster and more achievable because the extraction wound can trigger higher osteoclastic activity and metabolic changes in the alveolar bone for up to 4 months, resulting in accelerated orthodontic tooth movement.[14]
Age
Previous studies have shown that adult patients have decreased bone turnover rates during orthodontic force stimulation,[15] which is associated with inactive osteoblasts, fewer progenitor cells, reduced blood vessel formation, and denser bone. Conversely, younger patients have a more active cellular response to orthodontic force, more trabecular bone, and higher cytokine levels, which lead to faster tooth movement.[4]
Periodontal condition
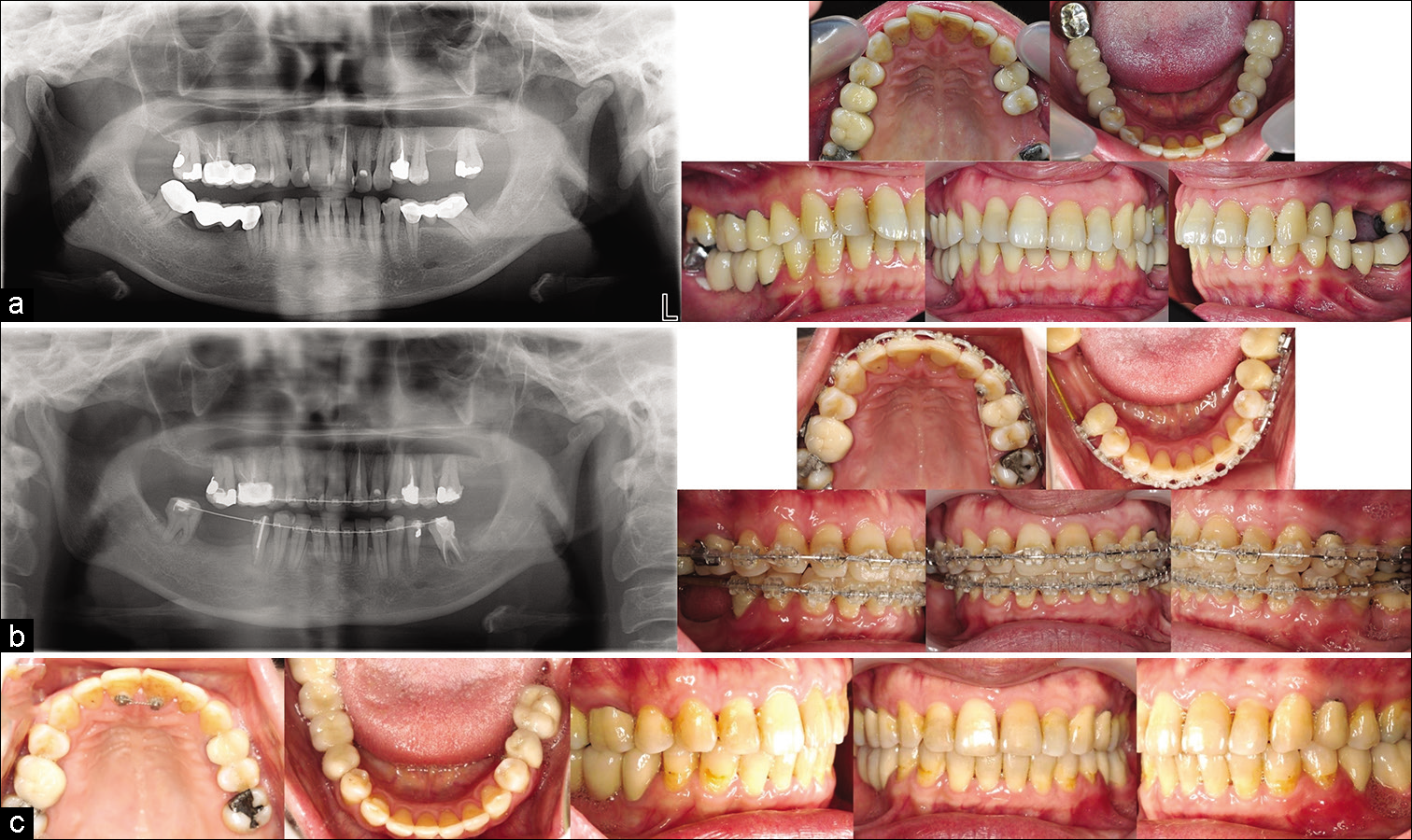
If the periodontal condition is poor before orthodontic tooth movement, once the teeth are pulled forward, bone remodeling around the existing inflammation results in worsening periodontal status.[16] Second molar protraction is time-consuming, making this option viable only when the periodontal health of the second molar is not compromised and patients have good oral hygiene.[10] [Figure 4] shows that although no bony defect was observed at the mandibular left second molar before orthodontic treatment, after its protraction toward the extraction socket, a vertical bony defect was found at the mesial root of the mandibular left second molar resulting from the longer treatment time and inadequate oral hygiene in this area.
- A vertical bony defect was found at the mesial root of the mandibular left second molar after the protraction.
Midline position and transverse dimension
A factor that must be considered in advance is that unilateral space closure will affect the midline position and the transverse dimension of the dental arch because the intermolar width will be reduced by the consolidation of the extraction space.[17] For example, in the case of midline deviation and asymmetric arch width with a missing molar on the narrower side, the recommendation is not to close the molar space but to create molar space, widen the dental arch, and correct the problem of the midline deviating to the edentulous side.
Sinus pneumatization
When the maxillary teeth have been missing for a long time, the paranasal sinus may increase in volume via a physiological process called sinus pneumatization. The inferior cortical bone of the sinus lowers closer to the root of the posterior teeth, which may affect their root movement. Some studies have reported that the missing tooth space can still be closed smoothly even in the presence of sinus pneumatization,[18-20] but other studies have shown that moving teeth toward the sinus floor cause root resorption[21] and that greater dental tipping is achieved than bodily movement, depending on the depth or surface area of the maxillary sinus recess.[22,23]
Opposing tooth, terminal molar morphology, and position
One of the main factors that determine whether a space should be closed or regained is the presence of opposing teeth. After the protraction of molars, occlusion with the antagonist dentition is necessary, particularly the terminal molars.[17]
The shape, size, and position of the terminal molars also play a vital role. Improving the occlusion and periodontal status of teeth is not beneficial if they have a poor crown-to-root ratio, are abnormally shaped, are supra-erupted, or exhibit mesial crown tilting.[17]
The factors determining molar space management are summarized in [Table 1].
| Space closure | Maintaining or regaining space | |
|---|---|---|
| Anterior crowding/protrusion | Yes | No |
| Alveolar ridge | Wide | Narrow |
| Extraction socket | Fresh | Healed |
| Age | Young | Old |
| Periodontal status | Healthy | Poor |
| Midline or transverse correction | Midline is shifted away from the space closure side without transverse discrepancy | Midline is shifted toward the edentulous space with deficient arch width |
| Posterior molar morphology and position | Normal morphology and position, or distal crown tipping of the molar | Poor morphology, short roots, mesial crown tipping of the molar |
| Sinus pneumatization | Possible, but careful biomechanics and unwanted side effects must be considered. | Yes |
BIOMECHANICS
Prevention of unwanted side effects
Tipping of posterior teeth
During molar protraction, a full-slot archwire, an uprighting spring, a long buccal hook placed at the uprighting tooth, or a reverse curve wire can be used to prevent posterior dental tipping by appropriately modifying the moment-to-force ratio.[24]
Mesial rotation and buccal sweeping
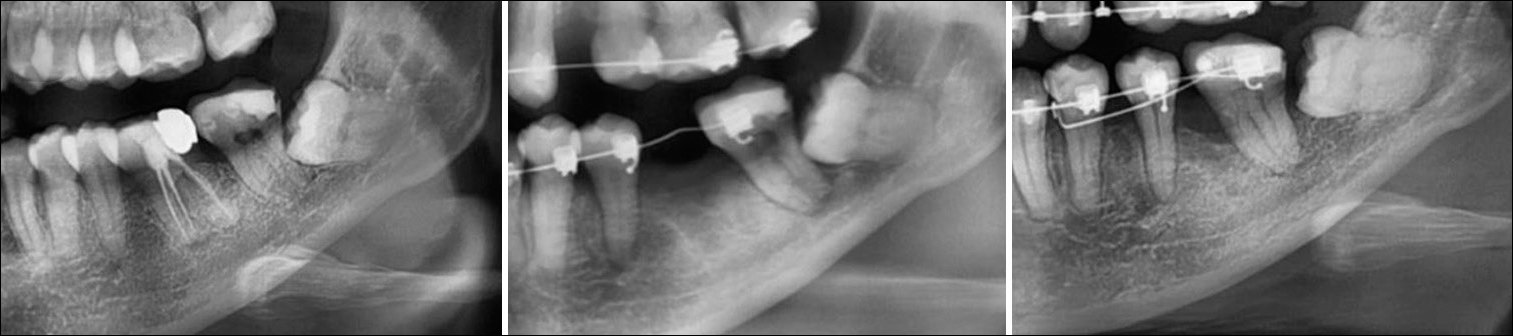
A toe-in bend in the posterior part of a wire, a balancing lingual force, or incorporation of the terminal molar into the archwire can prevent side effects such as mesial rotation of posterior teeth, buccal sweeping, or posterior crossbite resulting from the protraction force swinging the second molars buccally.[3,25] The mechanics of a toe-in bend are illustrated in [Figure 5].
- The toe-in bend prevents mesial rotation and buccal sweeping of the mandibular second molar: Blue arrows, moments generated by the protracting forces; yellow arrows, couples designed to counteract the moments.
Finite element analysis demonstrates that a molar tube with a 10-mm extension arm and a lingual force of half or equal magnitude to the buccal force are ideal to protract molars with fewer side effects, but these types of mechanics cannot be applied clinically in the posterior area because of anatomic limitations, such as the depth of the buccal sulcus.[26]
Anchorage preparation
Mandibular molar protraction has been reported as a challenging procedure because of the large root surface area of the molars, density of mandibular bone, and considerable anchorage demands. Without TSADs to enhance anchorage, unilateral mandibular protraction can be performed by adding 5–10° of labial crown torque to the mandibular incisors to maintain anterior anchorage and cinching back the archwire on the passive side to form an anchor unit.[25]
Extraoral appliances (e.g., chincap, facemask, or headgear) and intraoral appliances (e.g., transpalatal arch, lingual holding arch, or Forsus) are alternatives for anchorage reinforcement during second molar protraction.[5]
Without patient cooperation, TSADs are the best option to avoid anchorage loss. To pull the molars forward, these skeletal anchorage appliances are mostly placed on the side where molar protraction is required.[6-8] Nevertheless, the optimal approach is to wait until a canine Class I relationship is achieved with favorable root divergence between the canine and premolar teeth to facilitate TSAD placement for protracting the posterior teeth.
Third molar substitution
The successful replacement of second molars by third molars depends on the tooth morphology, angulation, eruption space, root developmental stage, and periodontal status of the third molars.[27] If spontaneous eruption of third molars is expected, the available space between the ascending ramus and the second molar should be prepared in advance.
The eruption of third molars after second molar extraction
Maxillary third molars are widely known to mostly erupt well, whereas complete eruption of the mandibular molars shows a wide variation of approximately 66–96%.[28,29] However, patients who had second molars extracted during or before orthodontic treatment mostly had their mandibular third molars uprighted and the second molars were successfully replaced. The unsuccessful eruption of mandibular third molars was due to excessive mesial tilting or the lack of proximal contact.[29]
The eruption of third molars after first molar extraction
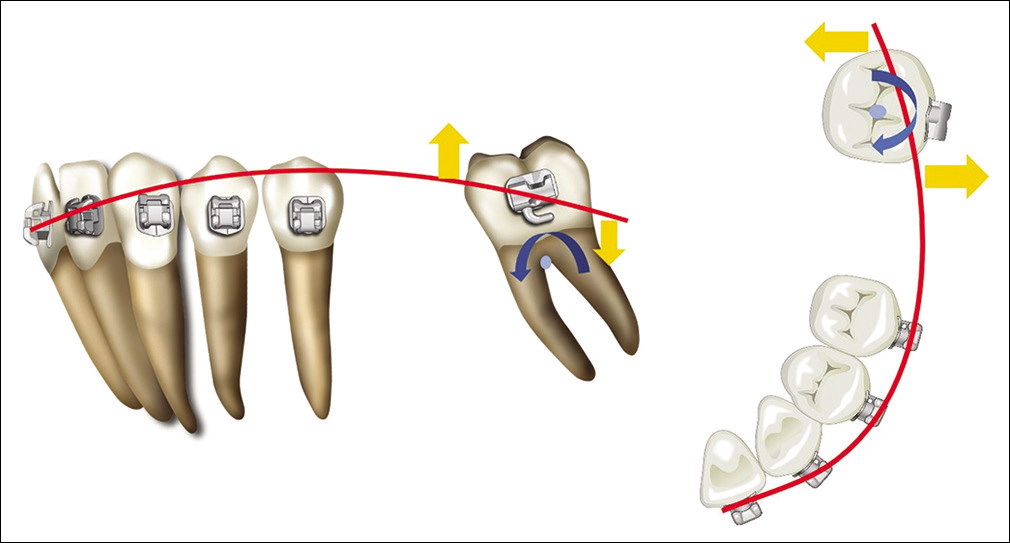
In the case of first molar extraction, space must be gained via second molar protraction, and the third molar will then erupt vertically.[30] The movement of the crown should be observed regardless of whether the third molar angulation is vertical or horizontally impacted, as long as the distance between the ramus and third molar is adequate. The radiographic records of the different results of impacted third molar eruption after second molar protraction are presented in [Figure 6].

- (a) No spontaneous eruption of the horizontally impacted third molar after second molar protraction. (b and c) Spontaneous eruption of the vertically impacted third molar.
CONCLUSION
Missing molar space can be managed by closing or opening the space with careful orthodontic assessment. To achieve a successful outcome, the decision-making process must be based on the aforementioned factors and orthodontic treatment must be based on rational biomechanical principles. Nevertheless, even with perfect planning and mechanics, the management of permanent molar absence is a major challenge. Hence, prevention and early interdisciplinary treatment are vital.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Evidence-based clinical recommendations for the use of pit-and-fissure sealants: A report of the American dental association council on scientific affairs. J Am Dent Assoc. 2008;139:257-68.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiological survey on prevalence of missing first molar due to caries: A case study. J Pharm Sci Res. 2015;8:1065-9.
- [Google Scholar]
- Molar protraction: Orthodontic substitution of missing posterior teeth In: Kim KB, ed. Temporary Skeletal Anchorage Devices. A Guide to Design and Evidence-Based Solution. Berlin, Heidelberg: Springer; 2014. p. :119-60.
- [CrossRef] [Google Scholar]
- Age effect on orthodontic tooth movement rate and the composition of gingival crevicular fluid. J Orofac Orthop. 2020;81:113-25.
- [CrossRef] [PubMed] [Google Scholar]
- Anchorage reinforcement with a fixed functional appliance during protraction of the mandibular second molars into the first molar extraction sites. Am J Orthod Dentofacial Orthop. 2015;148:165-73.
- [CrossRef] [PubMed] [Google Scholar]
- Titanium screw anchorage for protraction of mandibular second molars into first molar extraction sites. Am J Orthod Dentofacial Orthop. 2008;134:583-91.
- [CrossRef] [PubMed] [Google Scholar]
- Rigid endosseous implant utilized as anchorage to protract molars and close an atrophic extraction site. Angle Orthod. 1990;60:135-52.
- [Google Scholar]
- Rigid implant anchorage to close a mandibular first molar extraction site. J Clin Orthod. 1994;28:693-704.
- [Google Scholar]
- Treatment considerations for missing teeth In: Dental Anatomy. Rijeka: Intech; 2018. p. :109-20.
- [CrossRef] [Google Scholar]
- Orthodontic Management of Residual Spaces of Missing Molars: Decision Factors. In: Human Teeth-Key Skills and Clinical Illustrations. London: Intech Open; 2019.
- [CrossRef] [Google Scholar]
- Rationale for socket preservation after extraction of a single-rooted tooth when planning for future implant placement. J Can Dent Assoc. 2006;72:917-22.
- [Google Scholar]
- Five-year cephalometric study of mandibular ridge resorption with different posterior occlusal forms. Part I Denture construction and initial comparison. J Prosthet Dent. 1976;36:602-23.
- [CrossRef] [Google Scholar]
- Surgery-first accelerated orthognathic surgery: Postoperative rapid orthodontic tooth movement. J Oral Maxillofac Surg. 2011;69:781-5.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of an adult with several missing teeth and atrophic old mandibular first molar extraction sites. Am J Orthod Dentofacial Orthop. 2011;140:869-78.
- [CrossRef] [PubMed] [Google Scholar]
- Interrelationships between orthodontics and periodontics. Am J Orthod. 1976;70:154-72.
- [CrossRef] [Google Scholar]
- A comparative study of dental arch widths: Extraction and non-extraction treatment. Eur J Orthod. 2005;27:585-9.
- [CrossRef] [PubMed] [Google Scholar]
- Space closure in the maxillary posterior area through the maxillary sinus. Am J Orthod Dentofacial Orthop. 2014;145:95-102.
- [CrossRef] [PubMed] [Google Scholar]
- Knowledge of orthodontic tooth movement through the maxillary sinus: A systematic review. BMC Oral Health. 2018;18:91.
- [CrossRef] [PubMed] [Google Scholar]
- Maxillary molar intrusion with fixed appliances and mini-implant anchorage studied in three dimensions. Angle Orthod. 2005;75:754-60.
- [Google Scholar]
- Effects of maxillary molar intrusion on the nasal floor and tooth root using the skeletal anchorage system in dogs. Angle Orthod. 2003;73:158-66.
- [Google Scholar]
- Maxillary sinus floor extension and posterior tooth inclination in adolescent patients with Class II Division 1 malocclusion treated with maxillary first molar extractions. Am J Orthod Dentofacial Orthop. 2013;143:479-85.
- [CrossRef] [PubMed] [Google Scholar]
- The effect of the maxillary sinus floor on orthodontic tooth movement. Fortschr Kieferorthop. 1990;51:345-51.
- [CrossRef] [PubMed] [Google Scholar]
- Asymmetrical mandibular molar protraction with conventional mechanics. J Clin Orthod. 2015;49:304-11.
- [Google Scholar]
- Finite element analysis of mandibular molar protraction mechanics using miniscrews. Eur J Orthod. 2015;37:95-100.
- [CrossRef] [PubMed] [Google Scholar]
- Vertical eruption patterns of impacted mandibular third molars after the mesialization of second molars using miniscrews. Angle Orthod. 2016;86:565-70.
- [CrossRef] [PubMed] [Google Scholar]
- Eruption of third permanent molars after the extraction of second permanent molars. Part 1. Assessment of third molar position and size. Am J Orthod Dentofacial Orthop. 2001;119:226-38.
- [CrossRef] [PubMed] [Google Scholar]
- Spontaneous third-molar eruption after second-molar extraction in orthodontic patients. Am J Orthod Dentofacial Orthop. 2006;129:337-44.
- [CrossRef] [PubMed] [Google Scholar]
- Lower third molar development subsequent to second molar extraction. Am J Orthod Dentofacial Orthop. 1993;104:566-74.
- [CrossRef] [Google Scholar]




