

Translate this page into:
Orthodontic treatment of a patient with pycnodysostosis

*Corresponding author: Peter Ngan, Department of Orthodontics, West Virginia University, Morgantown, West Virginia, United States. pngan@hsc.wvu.edu
-
Received: ,
Accepted: ,
How to cite this article: Ngan P, Kim D, Guan G. Orthodontic treatment of a patient with pycnodysostosis. APOS Trends Orthod. 2025;15:86-92. doi: 10.25259/APOS_56_2024
Abstract
Pycnodysostosis (PYCD) is a rare lysosomal storage disease of the bone caused by a mutation in the gene that codes the enzyme cathepsin K. Patients diagnosed with PYCD demonstrate certain physical characteristics, including deformity in craniofacial structure for which patients seek orthodontic treatments to improve occlusal functions and esthetics. In addition, growth hormone therapy is indicated for these patients due to their short stature. This article is the first to report on the successful completion of the non-surgical orthodontic treatments of a patient diagnosed with PYCD. The patient was treated in two phases due to a waiting period for growth hormone therapy. However, superimposition of pre-and post-treatment radiographs showed no evidence of accelerated skeletal growth at the conclusion of the hormonal therapy. The rate of orthodontic tooth movement for Phase I with conventional appliance and Phase II treatment with clear aligners was similar with healthy individuals treated with four premolars extraction. Surgical exposure of the impacted permanent molars was contraindicated as no posterior dentition was available as anchorage for molar uprighting. Extraction of impacted molars in the mandible was performed with care due to the high risk of fracture. Orthognathic surgery treatment carries an increased risk of osteomyelitis for these patients due to dense bone with poor vascularity. Therefore, non-surgical camouflage orthodontic treatment can be the best option to achieve functional occlusion for patients diagnosed with PYCD.
Keywords
Craniofacial deformity
Hypoplastic mandible
Orthodontic treatment
Osteochondrodysplasia
Pycnodysostosis

INTRODUCTION
Pycnodysostosis (PYCD) is a rare metabolic bone disorder from osteoclast dysfunction.[1-4] It is inherited in an autosomal recessive pattern, and its prevalence is approximately 1:1.7 million with an equal sex predilection. About 30% of the studied cases are from consanguineous marriages.[5] The etiology of the disorder is a biallelic inactivating mutation in a gene that encodes Cathepsin K (CTSK), located in chromosome 1q21. CTSK is a lysosomal cysteine metalloproteinase enzyme involved in the degradation of protein matrix during bone resorption.[6,7] Mutation in this gene disturbs the bone-modeling process and leads to osteosclerosis, bone fragility, and susceptibility to pathologic fractures of the whole skeleton. The term PYCD was first coined by Maroteaux and Lamy in 1962 as a variant of osteopetrosis. The disorder is also known as Toulouse–Lautrec syndrome after a French artist, Henry de Toulouse Lautrec, who Maroteaux and Lamy suspected to have been affected by the disorder based on his self-portraits and descriptions of his physical characteristics in other documents.[8] Affected individuals display short stature (average adult height under 5 feet) with short limbs and a relatively large head with frontal and parietal bossing. Short stubby hands and feet, bulbous terminal phalanges due to acro-osteolysis, and dystrophic nails are characteristic of the disorder. Facial bones tend to be hypoplastic with an obtuse angle of the mandible. It is common for the maxilla to be more hypoplastic than the mandible, with a narrow palate that results in cross-bite.[5,9-11] Typical dental anomalies are oligodontia, retained deciduous dentition, delayed eruption of permanent dentition, crowded or malposed teeth, enamel hypoplasia, abnormal tooth morphology, dilacerated and hypoplastic root apices, and poor oral hygiene. The radiographic findings of osteosclerosis, particularly in long bones, the spine, and the base of the skull, can differentiate the condition from other similar conditions, such as achondroplasia and cleidocranial dysplasia.[1,9] Additional radiographic features are delayed closure of cranial sutures with patent fontanelles and hypoplastic or absent paranasal sinuses. Tapering of the distal phalanges of the fingers and toes and absence or poor development of the ungual tufts may also be shown. Life expectancy is normal. However, affected individuals tend to suffer from many different conditions throughout their lifetime. Commonly reported systemic conditions include respiratory symptoms, obstructive sleep apnea, and hearing loss.[2,12] Particularly concerning to dental practitioners are hypoplastic maxilla and mandible, dental anomalies, bone fragility, and osteosclerosis complicating dental extractions and post-operative healing.[10,13]
Despite consistent findings in occlusal and craniofacial abnormalities, there are few reports about comprehensive and successful orthodontic treatments for PYCD patients. Among the reported cases, maxillary expansion has frequently failed to create adequate space for dental alignment and optimal occlusion.[2,14,15] A case of the initial phase of treatment with slow expansion was reported successful, but the report was made right after the expansion and during active treatment, and no long-term outcome was available.[16] One report demonstrated an unconventional prosthetic approach to improve esthetics for a patient whose orthodontic treatments did not succeed in improving both mastication functions and esthetics.[14] In the present case report, we present a case with PYCD that was successfully treated with comprehensive orthodontic treatment without orthognathic surgery.
CASE REPORT
Diagnosis, regional, and systemic characteristics
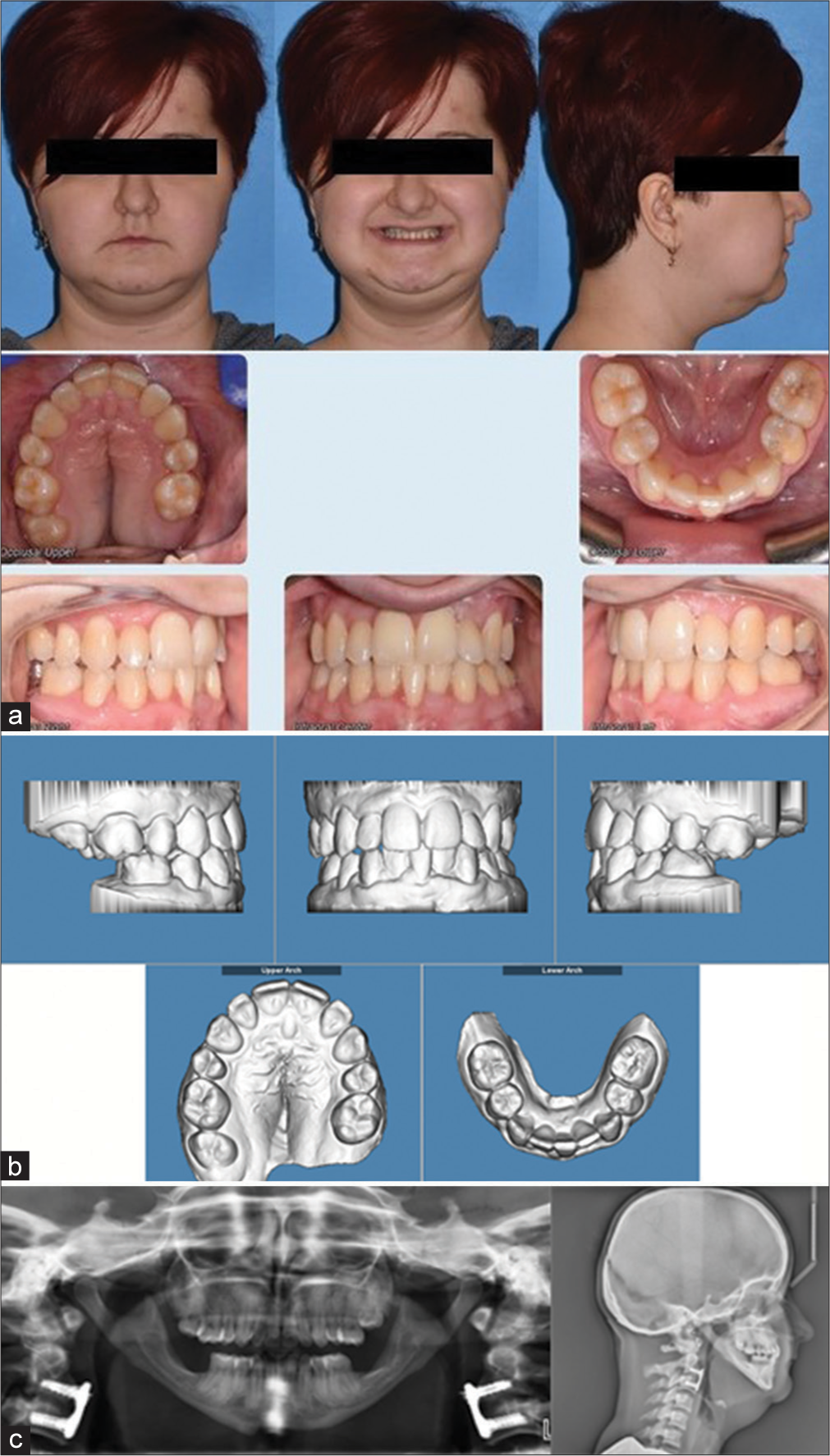
This 10-year-old female patient first presented with a chief concern of “not enough space for the front teeth.” [Figures 1a-c] show the pre-treatment orthodontic records. The patient was brought into the clinic with her grandmother. The patient had not been diagnosed with any syndrome but a history of short stature with a standing height of 120 cm, dysmorphic facies, and failure to thrive. Her digits were short, spoon shaped, stubby with joint laxity, metaphyseal widening, and dystrophic nails. In addition, a sandal gap deformity was seen. A definitive diagnosis of dwarfism and PYCD was diagnosed at age 14. [Figure 2] shows the systemic radiographic findings provided by the physician. The radiographs showed significant diffuse skeletal hyperostosis with sparing of the medullary cavity and scoliosis. Skull X-ray showed widely separated cranial sutures and widely open anterior and posterior fontanel. A retrospective evaluation revealed that the patient was born full-term delivery and normal weight at the hospital. Maternal and neonatal history was uneventful. Immunization was adequate, with normal developmental milestones and intelligence. The grandparent denied any history of trauma or fractures. There was no history of frequent respiratory tract infections, snoring, or tuberculosis contact. No similar symptoms had been found for siblings or parents. The grandparent also reported that the patient was on growth hormone therapy during the pubertal growth spurt due to short stature.
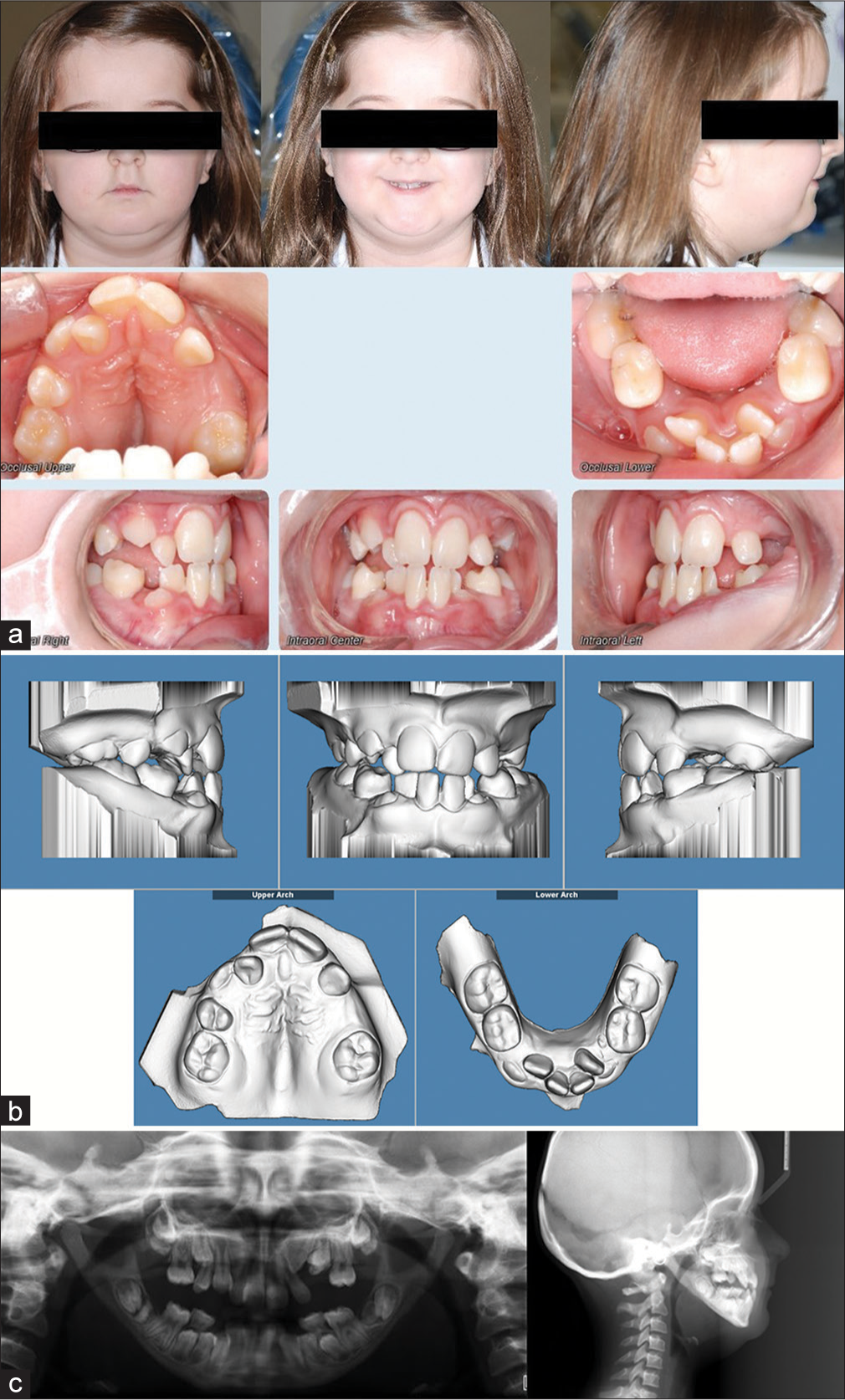
- (a) Phase I pre-treatment extraoral and intraoral photographs. (b) Phase I pre-treatment models. (c) Phase I pre-treatment panoramic radiograph, lateral cephalogram.

- Systemic radiographs for diagnosis of pycnodysostosis.
Craniofacial and dental examinations revealed a chubby face with mandibular retrognathism [Figure 1a]. Panoramic radiograph revealed a hypoplastic maxilla and mandible with a very obtuse angle of the mandible, causing complete horizontal impaction of the mandibular second and third molars [Figure 1c]. Intraoral examination revealed a Class III malocclusion with severe crowding of anterior teeth, maxillary transverse deficiency, and edge to edge incisal bite [Figures 1a and b]. Pretreatment models demonstrate her remarkably small mandible that is comparable in size to a US quarter [Figure 3]. A cephalometric radiograph revealed a normal maxilla and confirmed a hypoplastic mandible with mandibular retrognathism [Figure 1c]. The mandible was hypoplastic; the condylar neck was long and narrow with an obtuse gonial angle and hyperdivergent growth pattern. The skeletal maturation was determined to be pre-peak pubertal growth around Stage 2 of cervical vertebral maturation.
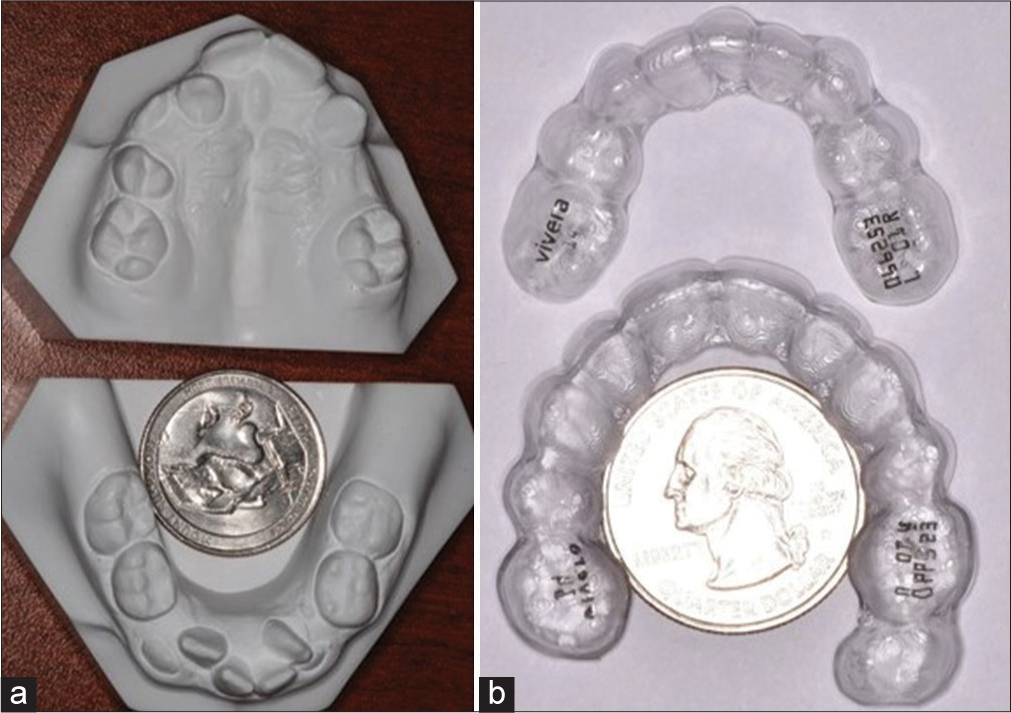
- (a) Phase I pre-treatment models and (b) Phase II post-treatment retainer comparing the size of the dental arches to a United States quarter coin.
Orthodontic treatment objectives
The initial treatment objectives for this patient included space maintenance before a decision on the extraction of permanent teeth, orthodontic treatment to correct the maxillary transverse discrepancy, eliminating dental crowding, establishing overbite and overjet for proper occlusal function, and improvement of soft-tissue profile.
Treatment alternatives
Consultation with oral surgery confirmed that orthognathic surgery treatment was not an option due to the weak hypoplastic mandibular structure. Camouflage orthodontic treatment was the only viable option to provide a functional occlusion. Comprehensive Phase I orthodontic treatment with full fixed appliance and rapid palatal expansion appliance was planned to correct the maxillary transverse deficiency and Class II elastics were used to improve the overjet and molar relationship. The patient was judged to have an upward and forward growth of the mandible. Due to growth hormone therapy, the comprehensive orthodontic treatment was rendered in two phases since growth changes of the maxilla and mandible were not predictable during hormonal therapy. The first phase of treatment included the extraction of permanent teeth to relieve crowding and to correct anterior cross-bite. The second phase of treatment was rendered after the pubertal growth spurt and growth hormone therapy to achieve proper overjet and overbite.
Treatment progress
A transpalatal bar was placed at age 11 for space maintenance. After a diagnosis of PYCD was confirmed with the physician, a Phase I comprehensive orthodontic treatment was initiated. The patient was treated with a rapid maxillary expansion appliance and extraction of the upper and lower first premolars and a lower left central incisor.
After 36 months of active treatment, a decision was made not to complete orthodontic treatment until the completion of pubertal growth and hormonal therapy. All fixed appliances were debonded or debanded. A clear retainer was placed in both the maxillary and mandibular arches [Figure 4a and b].

- (a) Phase I post-treatment extraoral and intraoral photographs. (b) Phase I post-treatment panoramic radiograph and lateral cephalogram.
The patient was recalled at age 19. The patient’s grandmother reported that the patient had an occasional fracture of bones in the legs. Panoramic radiograph showed the presence of horizontally impacted lower molars. Orthodontic uprighting of the impacted molars was deemed impossible due to the lack of orthodontic anchorage, and the successful placement of microimplants as anchorage was questionable. Consultation with oral surgery recommended removal of impacted molars with caution due to hypoplastic mandible. After completion of growth hormone therapy, Phase II comprehensive orthodontic treatment was initiated [Figure 5a and b]. After 18 months of comprehensive orthodontic treatment with clear aligners, a stable occlusion with proper overjet and overbite was achieved and the patient had been given clear retainers for retention [Figure 6a and b]. The patient was recalled in 1 year at age 21 for post-treatment stability. Occlusion was found stable with acceptable esthetic results [Figure 7a-c].
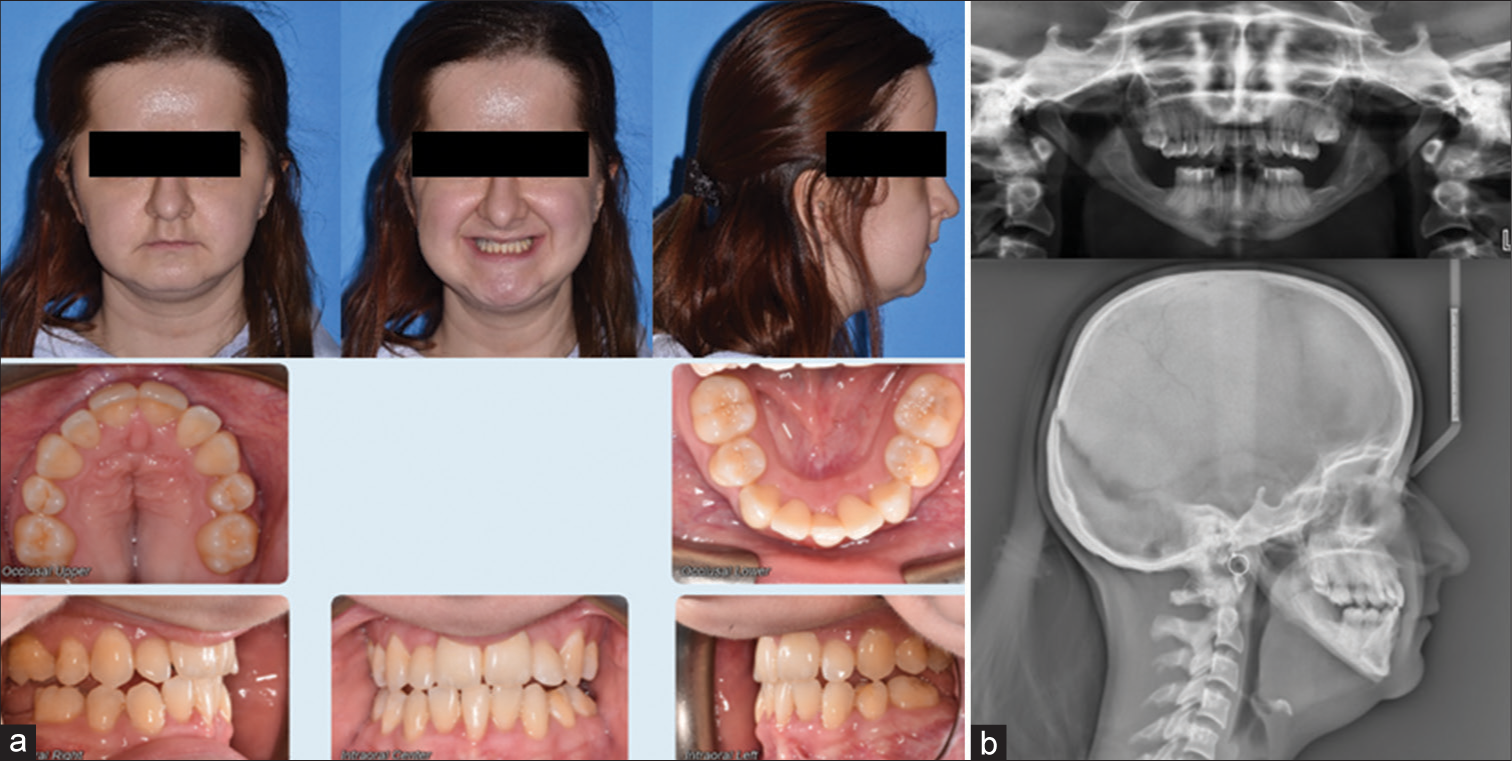
- (a) Phase II pre-treatment extraoral and intraoral photographs. (b) Phase II pre-treatment panoramic radiograph and lateral cephalogram.
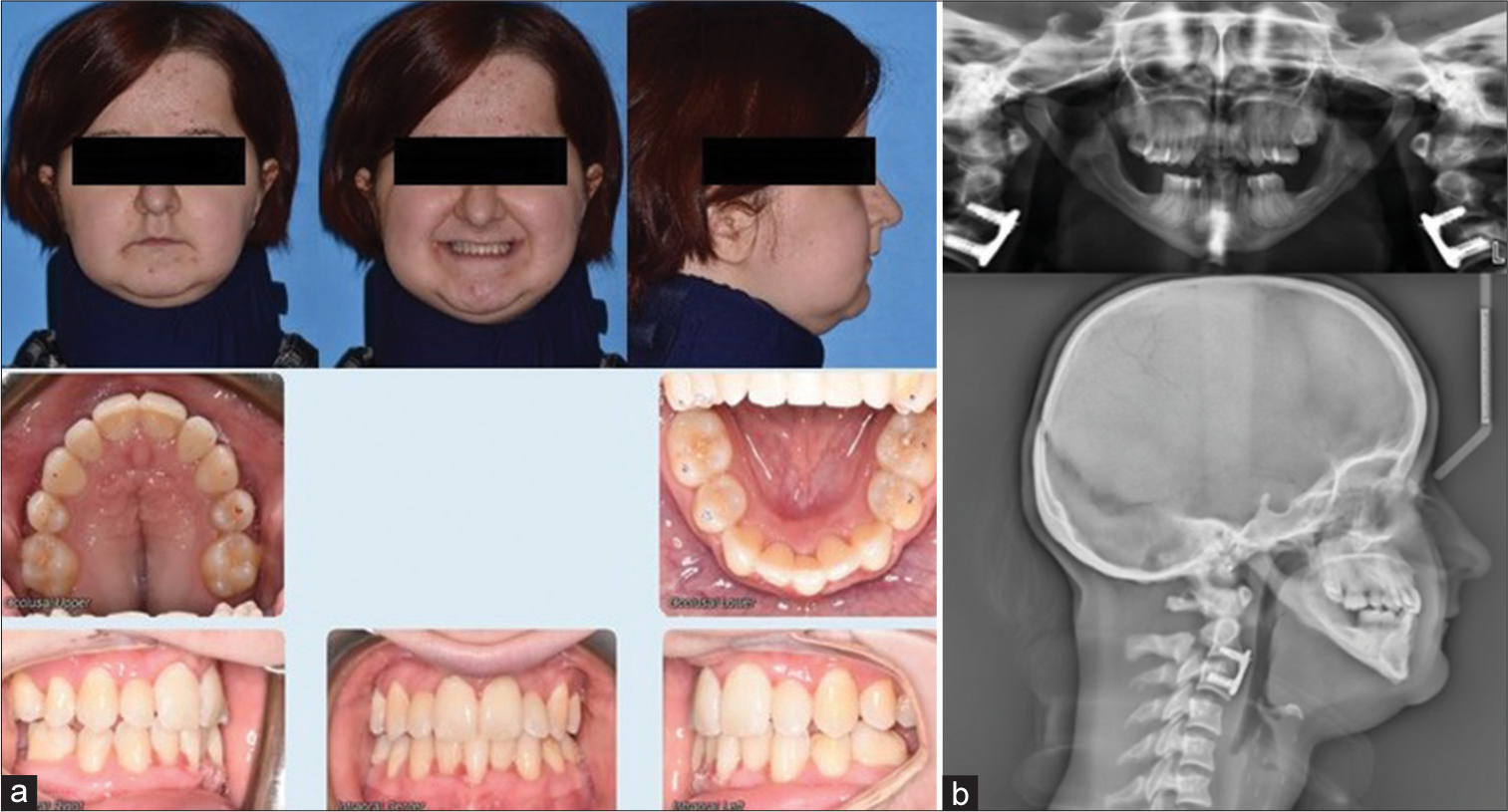
- (a) Phase II post-treatment extraoral and intraoral photographs. (b) Phase II post-treatment panoramic radiograph and lateral cephalogram.
- (a) One-year post Phase II treatment extraoral and intraoral photographs. (b) One-year post Phase II treatment models and (c) 1-year post Phase II treatment panoramic radiograph and lateral cephalogram.
Treatment results
A stable occlusion was achieved despite asymmetric extraction of one lower central incisor. The overbite and overjet were improved. The anterior cross-bite was eliminated. The patient was satisfied with the esthetic outcome. The post-treatment panoramic radiograph indicated well aligned roots with minimal root resorption [Figure 7c]. Superimposition of the Phase I pre-treatment lateral cephalogram and Phase II post-treatment lateral cephalogram revealed a downward growth of the maxilla and a forward growth of the mandible [Figure 8]. The growth magnitude of the maxilla and mandible was significantly smaller than unaffected Class I individuals. The maxillary incisors were maintained at 104 degrees to sella-nasion and the mandibular incisors at 77 degrees to the mandibular plane [Table 1].
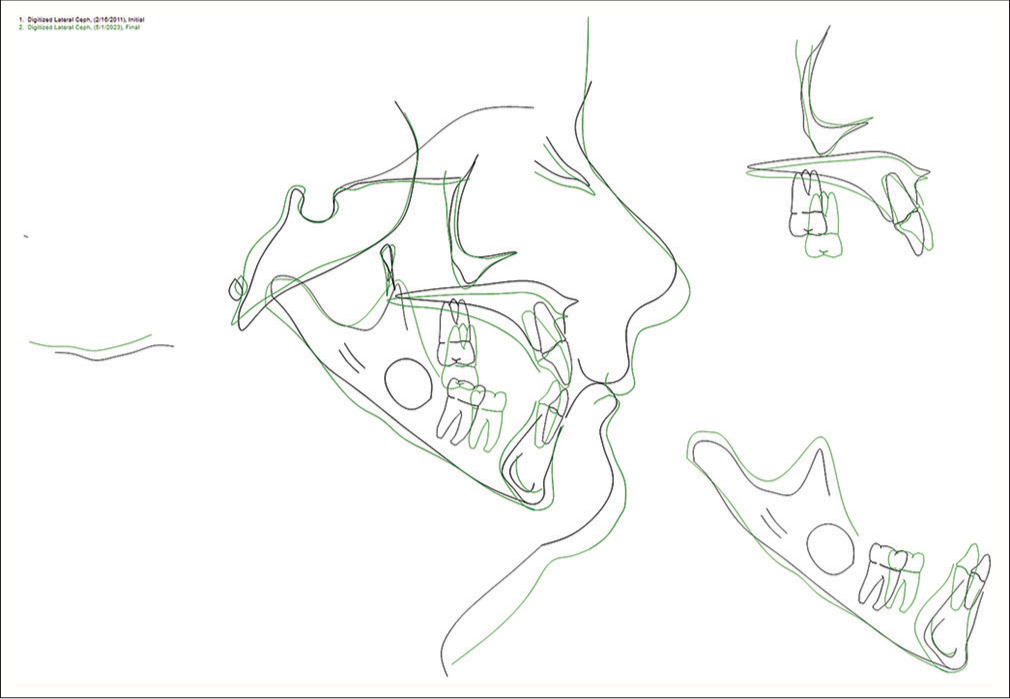
- Superimposition of Phase I pre-treatment at age 10 and 1-year-after Phase II post-treatment at age 21 radiographs. Black line: Pre-treatment at age 10; Green line: Post-treatment at age 21.
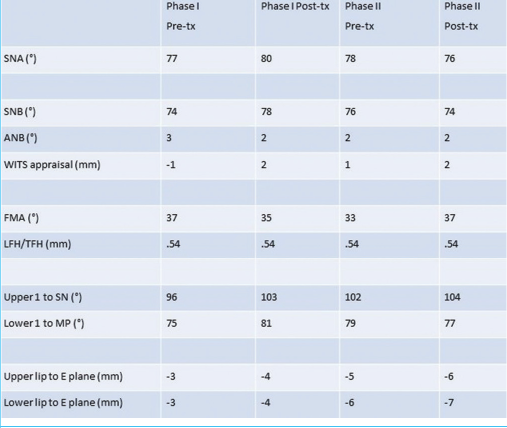 |
FMA: Frankfurt Mandibular Plane Angle, LFH: Lower Face Height, ANB: Point A-Nasion-Point B, TFH: Total Face Height, SNA: Sella Nasion/A point, SNB: Sella Nasion/B point
DISCUSSION
PYCD is an inherited disorder of the bone caused by a mutation in the gene that codes the enzyme CTSK. This enzyme is important for osteoclasts to resorb and build new bone.[6,7] Individuals with this disorder have abnormally dense and brittle bones because of insufficient bone resorption and are often present with occasional fractures of bones in the extremities.
The patient in the current report was diagnosed solely by clinical findings. Genetic tests are available but not supported by the patient’s insurance policy. Various bone diseases should be considered in the differential diagnoses of PYCD that also demonstrate reduced bone resorption including cleidocranial dysostosis, acroosteolysis, osteogenesis imperfecta, and osteopetrosis.[1,9,10] Dentists should be aware of the clinical manifestations of PYCD, such as short stature, large head and frontal bossing, underdeveloped facial bones, dental anomalies, short and broad hands, and feet with dystrophic nails and trunk deformities such as scoliosis.[1,2,7] Malocclusions in these patients are often severe and cause not only esthetic concern but also disruption in mastication for which they receive orthodontic treatments.[14-19] Typical craniofacial phenotypes are hypoplastic mandible, maxillary and mandibular jaw discrepancies, high and narrow palate, downward and backward rotation of the mandible, anterior cross-bite, crowding of the maxillary, and mandibular dentition due to small dental arches.[5,9-11]
To improve skeletal growth, treatment with growth hormone therapy during the puberty growth period is often recommended. Comprehensive orthodontic treatment that is usually carried out during the growth period may need to be postponed due to unpredictable growth of the maxilla and mandible during hormonal therapy. In the present case report, the patient was treated in two phases before and after hormonal therapy. However, superimposition of the pre- and post-treatment radiographs showed no increase in skeletal growth from the hormonal therapy.
Notably, the patient presented in this case report did not require modification in the rate of tooth movements. The rate of orthodontic tooth movement in patients diagnosed with PYCD was not available in the literature. In the current case report, the treatment period for both Phase I with conventional orthodontic appliance and Phase II with clear aligner treatment was similar to a healthy patient with extraction of four premolars. This may owe to the fact that patients with PYCD have shown residual resorptive capacity. The mutation in the CTSK gene results in CTSK deficiency and causes disruption in osteoclast activity but does not cause problems with the development of osteoclasts. Patients with PYCD have normal numbers of differentiated osteoclasts, and it is speculated that other unaffected proteases in their osteoclasts may provide resorptive activity.[20] In our current case report, after active orthodontic treatments, the patient was given removable clear retainers. No relapse in alignment of teeth was noted during retention.
Several non-surgical orthodontic cases have been reported in the literature with attempts on improving masticatory functions and esthetics but no cases with completed treatments or clinically successful outcomes have been presented.[14-16] The failures may be accounted for by the fact that the discrepancies were too severe to sufficiently correct by conventional orthodontic approaches that did not employ orthognathic surgeries. A few cases with orthognathic surgeries have been reported with fair to good outcomes.[17,18] However, orthognathic surgeries may still pose a greater risk of osteomyelitis postoperatively for these patients afflicted with PYCD and may not be desired by the patients.[13,19] For this reason, extraction of malposed posterior teeth should be prescribed with caution due to the brittle jawbone. Surgical exposure of mandibular second molars was not chosen in this case for lack of more posterior teeth to use as anchorage for the treatment. This case report demonstrates that camouflage orthodontic treatment is an alternative and conservative approach for patients to obtain functional occlusion with acceptable esthetic outcomes.
CONCLUSION
This case report presented the clinical, radiographic, and dental manifestation of a rare inherited disorder of the bone, e.g. PYCD. Awareness and understanding of the differential diagnosis of this disorder are essential to dental practitioners, including orthodontists. Orthodontic treatment of these patients may include more than one phase of comprehensive orthodontic treatment due to hormonal therapy and the unpredictable growth rates and direction of the jaws. Successful orthodontic treatment of these patients is possible with good communication among the orthodontist, pediatric dentist, and physician.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Pycnodysostosis; a rare disease case report. J Ayub Med Coll Abbottabad. 2022;34:216-19.
- [CrossRef] [PubMed] [Google Scholar]
- Pycnodysostosis, a lysosomal disease caused by cathepsin K deficiency. Science. 1996;273:1236-8.
- [CrossRef] [PubMed] [Google Scholar]
- Pycnodysostosis In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Bean LJ, eds. GeneReviews®. Seattle, WA: University of Washington, Seattle; 1993-2024.
- [Google Scholar]
- Pycnodysostosis: The disease of Henri de Toulouse-Lautrec. Eur J Orthop Surg Traumatol. 2018;28:1569-72.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical and cephalometric analysis of three cases with pycnodysostosis: Case reports. J Istanb Univ Fac Dent. 2015;49:51-5.
- [CrossRef] [PubMed] [Google Scholar]
- Pycnodysostosis: A case report and literature review concerning oral and maxillofacial complications and their management. Oral Surg Oral Med Oral Pathol Oral Radiol. 2021;132:e127-38.
- [CrossRef] [PubMed] [Google Scholar]
- Pycnodysostosis in an adult: A case report and review of the literature. Ear Nose Throat J. 2019;98:627-8.
- [CrossRef] [PubMed] [Google Scholar]
- Pycnodysostosis presenting as atypical stridor. Eur Ann Otorhinolaryngol Head Neck Dis. 2016;133:87-90.
- [CrossRef] [PubMed] [Google Scholar]
- Osteomyelitis of the jaws in patients with pycnodysostosis: A systematic review. Braz J Otorhinolaryngol. 2021;87:620-8.
- [CrossRef] [PubMed] [Google Scholar]
- Alternative method for full oral rehabilitation in patients with pycnodysostosis syndrome: A case report. Clin Cosmet Investig Dent. 2020;12:131-9.
- [CrossRef] [PubMed] [Google Scholar]
- Pycnodysostosis with special emphasis on dentofacial characteristics. Case Rep Dent. 2015;2015:817989.
- [CrossRef] [PubMed] [Google Scholar]
- Challenges in the orthodontic treatment of a patient with pycnodysostosis. Cleft Palate Craniofac J. 2014;51:735-9.
- [CrossRef] [PubMed] [Google Scholar]
- Orthognathic surgery in pycnodysostosis: A case report. Int J Oral Maxillofac Surg. 2011;40:110-3.
- [CrossRef] [PubMed] [Google Scholar]
- Maxillary distraction osteogenesis in a patient with pycnodysostosis: A case report. J Oral Maxillofac Surg. 2004;62:1037-40.
- [CrossRef] [PubMed] [Google Scholar]
- Mandibular reconstruction in a patient with pyknodysostosis. J Oral Maxillofac Surg. 1996;54:513-7.
- [CrossRef] [PubMed] [Google Scholar]
- Pycnodysostosis: Role and regulation of cathepsin K in osteoclast function and human disease. Curr Mol Med. 2002;2:407-21.
- [CrossRef] [PubMed] [Google Scholar]




