

Translate this page into:
The use of Korat-modified nasoalveolar molding devices in patients with unilateral complete cleft lip and palate with a 5-year follow-up


-
Received: ,
Accepted: ,
How to cite this article: Virarat P, Nirunrungrueng P, Techalertpaisarn P, Ungvijanpunya N. The use of Korat-modified nasoalveolar molding devices in patients with unilateral complete cleft lip and palate with a 5-year follow-up. APOS Trends Orthod. doi: 10.25259/APOS_150_2023
Abstract
The nasoalveolar molding (NAM) appliance has been the appliance of choice for pre-surgical orthopedics to improve nasal and lip morphology, and optimally align the alveolar segments before cheiloplasty. However, the appliance has some limitations, including its complexity and long clinical chair time for appliance adjustments. In this case report, we present a patient treated for a right complete cleft lip and palate using three types of Korat modification for NAM with a 5-year follow-up. This study demonstrated that the Korat-NAM improved the aforementioned issues and was suitable for patients at different stages before and after lip and palate repair.
Keywords
Korat-NAM
Nasoalveolar molding
Cheiloplasty
Rhinoplasty
Cleft lip and palate

INTRODUCTION
Patients with a cleft lip and palate (CLP) need to undergo multiple surgeries to correct their abnormalities.[1] Due to multiple factors, revision surgery is typically required to further correct nose and lip deformities with tension and scars.[2,3]
The nasoalveolar molding (NAM) appliance is widely used for pre-surgical orthopedics to prepare the soft tissue position and morphology to be appropriate for lip and palate repair.[4,5] However, using this appliance is challenging because it requires a meaningful amount of laboratory time, long clinical chair time, cooperation from the patients and parents, parents’ understanding of how the appliance should be worn, and frequent follow-up visits.[6]
Nakhon Ratchasima province (Korat) is located in the northeastern part of Thailand with an incidence of patients with cleft palate of 1.4:1,000 live births.[7] In this region, there are a limited number of hospitals that can provide comprehensive care to CLP patients. Most of the CLP patients in this area are referred to our Cleft Center Maharat Nakhon Ratchasima Hospital. Considering the pre-surgical orthopedic treatment for CLP patients, there are concerns about the number of hospital visits, parents’ understanding of the appliance care and adjustments, and treatment costs. In addition, there are an increasing number of patients admitted to our Cleft Center. Therefore, we have been modifying our protocol to efficiently provide comprehensive treatment, including NAM appliances and surgical techniques.
In this case report with a 5-year follow-up, we present a patient with a right complete CLP. We explain our protocol for using the NAM appliance with three types of modification at our Cleft Center Maharat Nakhon Ratchasima Hospital (Korat-NAM) together with modified cheiloplasty, primary rhinoplasty, and palatoplasty surgical techniques. Each type of Korat-NAM that was prescribed to the unilateral complete CLP (UCLP) patients at different time points is explained in detail.
THE TREATMENT PROTOCOL OF THE CLEFT CENTER MAHARAT NAKHON RATCHASIMA HOSPITAL, NAKHON RATCHASIMA, THAILAND FOR PATIENTS WITH UCLP
A timeline of the treatment protocol at our Cleft Center for patients with UCLP is illustrated in [Figure 1]. Ideally, patients are accepted to our center within a few days after birth for the initial visit that includes an examination and taking an impression for an active obturator to be inserted on the same day. When the patients are approximately 1 month old, another impression is taken for the KoratNAM I (explained in detail later) that will be worn until the patients are ready for the primary correction (cheiloplasty and primary rhinoplasty). During this time, the patients come to our clinic for a Korat-NAM I adjustment every 2 weeks. Primary correction is performed when the patients are approximately 6 months old. Immediately after surgery, the customized nasal conformer is sutured with the nostril and retained for 3 weeks. Upon conformer removal, the Korat-NAM II is inserted, worn, and adjusted monthly until the patients are ready for palatoplasty at approximately 1 year and 6 months old. Three weeks after surgery, the patients are instructed to wear the Korat nasal molding appliance III (Korat-NM III) for a minimum of 2 h a day. The patients come to the clinic to adjust the appliance every 3 months.
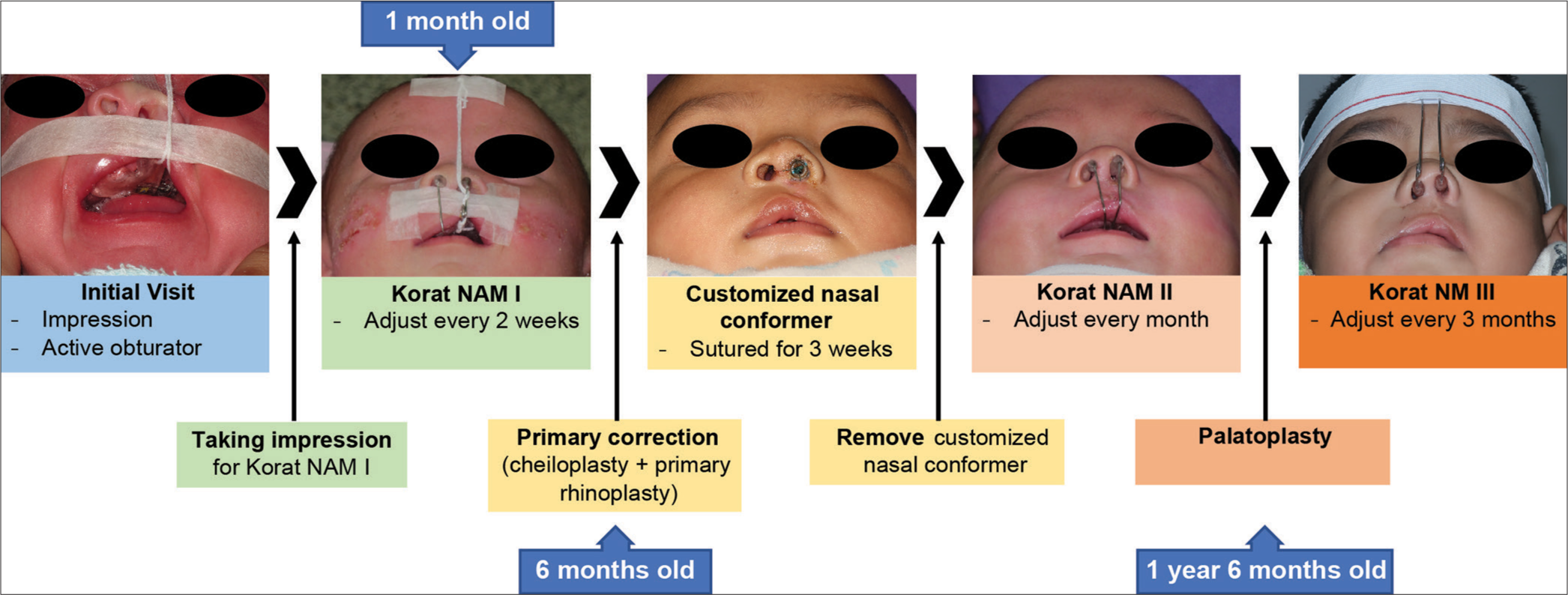
- A timeline of the treatment protocol at our Cleft Center for patients with a left complete cleft lip and palate (consists of photos from several patients). The patient is accepted for the initial visit ideally as soon as possible after birth when the impression is taken for active obturator delivery on the same day. The Korat-NAM I is usually inserted when the patient is 1 month old and a 2-week follow-up for appliance adjustment is required. Primary correction is performed when the patient is ~6 months old. A customized nasal conformer is sutured and retained for 3 weeks immediately after the surgery. On nasal conformer removal, the Korat-NAM II is delivered to the patient and adjusted once a month. Later, the patient undergoes palatoplasty at ~1 year and 6 months old. Approximately 3 weeks after palatoplasty, the patient is instructed to wear the Korat-NM III and comes to the clinic for appliance adjustment every 3 months. Please note that the time points may vary slightly among patients. NAM: Nasoalveolar molding, NM: Nasal molding.
THREE TYPES OF MODIFICATION OF THE NAM APPLIANCE BY THE CLEFT CENTER MAHARAT NAKHON RATCHASIMA HOSPITAL (KORAT-NAM) AND INVOLVED SURGERIES
The appliances presented in this section are for patients with a left complete CLP. Written informed consent was obtained from all parents of patients who were included in this report.
Active obturator
Patients are first assessed for the need to wear an active obturator before Korat- NAM I. If a cleft size is more than 10 mm, the patient is prescribed an active obturator with a retraction screw to align the alveolar segments and decrease the cleft size. Patients with a large cleft may need two obturators for the stepwise reduction of the alveolar cleft. It is used with micropore surgical tape across the cheeks to reduce the cleft size on the upper lip.
Korat-NAM I
There are two components of the Korat-NAM I [Figure 2a]. The first component is a passive obturator. The second component is the nasal part that projects into the nostrils.

- (a) Components of the Korat-NAM I (a1) are a passive obturator with acrylic bite block on both sides, (a2) extending arm on the cleft side with a coil that allows additional activation, (a3) extending arm on the non-cleft side, (a4) nasal acrylic piece on the cleft side, and (a5) nasal acrylic piece on the non-cleft side. (b) The acrylic nasal piece is 11–15 mm long with 6–8 mm inside the nostril. When the patient wears the Korat-NAM I, a thread is used to reinforce appliance retention and guide the appliance insertion and removal. (c, arrow) Both legs of the thread are wrapped around the extending wire on the cleft side and end toward the medial side. (d) The two extending arms (arrowhead) help maintain the nipple in place and squeeze the milk out during feeding. NAM: Nasoalveolar molding.
If the cleft size is more than 4 mm but <10 mm, a set-up model is required to align the alveolar segment when fabricating the obturator part of Korat-NAM I. With a cleft size <4 mm, a set-up model is not required. In this obturator part, there is an acrylic bite block [Figure 2a-1], which is a bite registration fabricated from an impression of the opposing alveolar ridge of the posterior teeth region at the physiologic rest position (2–3 mm apart). This bite block is placed for stabilizing the appliance when the patient bites and sucks on the bottle, increasing appliance retention.
The nasal part consists of two 0.8-mm spring-hard stainless-steel arms extending from the plate to the nostril on the cleft and non-cleft sides.
On the cleft side
The arm [Figure 2a-2] extends from the plate with a 4-mm coil. The end of this wire is folded as retention for an acrylic piece which is kidney-shaped with a curved end to support the dome-shaped nasal cartilage on the medial side [Figure 2a-4, 2b]. This arm is adjusted to stretch the nostril 1–2 mm (the alar tissue becomes pale).
On the non-cleft side
The arm [Figure 2a-3] extends from the plate without a coil and then projects upward with a 2-mm longer distance than on the cleft side. The acrylic part is smaller and positioned closer to the columella than on the cleft side to support the columella [Figure 2a-5]. This arm also provides additional retention to the appliance.
The Korat-NAM I appliance is used with micropore surgical tape across the cheeks to reduce the cleft size on the upper lip. A small hole is drilled through the plate to insert the thread and a knot is tied using both ends. Both legs of the thread are wrapped around the extending wire on the cleft side [Figure 2c-arrow] and are attached to the patient’s forehead to reinforce the appliance retention and easily guide the parents on how to insert and remove the appliance. The two extending arms also help maintain the nipple in place and squeeze the milk out during feeding [Figure 2d-arrowhead].
At each follow-up appointment, the two arms are adjusted to support the columella on the non-cleft side and stretch the nostril on the cleft side upward 1–2 mm, or until pale skin is observed.
Primary correction (cheiloplasty with primary rhinoplasty)
At our center, we use a combination of surgical techniques modified based on Millard’s rotation advancement method[8,9] with the goals of creating equal distance from the oral commissure to the cupid bow on both sides, a faint white roll line, an appropriate vermillion thickness, and an elongated and lifted columella base on the cleft side. An additional flap similar to Fisher’s cheiloplasty[10] method and a lateral V Noordhoff flap[11] are performed. Based on the paradigm of treating the lip and nose as one unit, we perform a primary rhinoplasty at the time of cheiloplasty. Following Tajima’s method,[12] the reverse-U incision is performed. Thereafter, we maintain the nostril shape with the customized nasal conformer that is fabricated from an endotracheal tube. The conformer is sutured and held with the nasal septum behind the columella for 3 weeks. In addition, we transfix the mucosa of the lateral nasal wall and the alar base with the dermis using one suture each to reduce hematoma and swelling. At 3 weeks post-surgery, we remove the customized nasal conformer and continue with the Korat-NAM II to maintain the nostril and alar rim and prevent relapse.
Korat-NAM II
Before primary correction, an impression is taken for fabricating the Korat-NAM II to replace Korat-NAM I which begins to wear down by this time. Three weeks after primary correction [Figure 3a], the customized nasal conformer is removed, the nostril is cleaned, and the Korat-NAM II is inserted. The Korat-NAM II is similar to the Korat-NAM I, except that there is no coil on the extending arm on the cleft side since it is mainly used as a nostril shape retainer (less activation is needed than the Korat-NAM I) [Figure 3b-1]. Moreover, without a coil on the cleft side, the extension arm can curve upward smoothly to avoid pressing on the lip after surgery. In addition, denture adhesive is required to retain the appliance with the upper arch. The alveolar ridge of the anterior teeth area part of the acrylic plate is removed to accommodate the erupting primary teeth during monthly follow-up visits. The Korat-NAM II is used to maintain the nose morphology after primary correction until before the palatoplasty [Figure 3c and d].
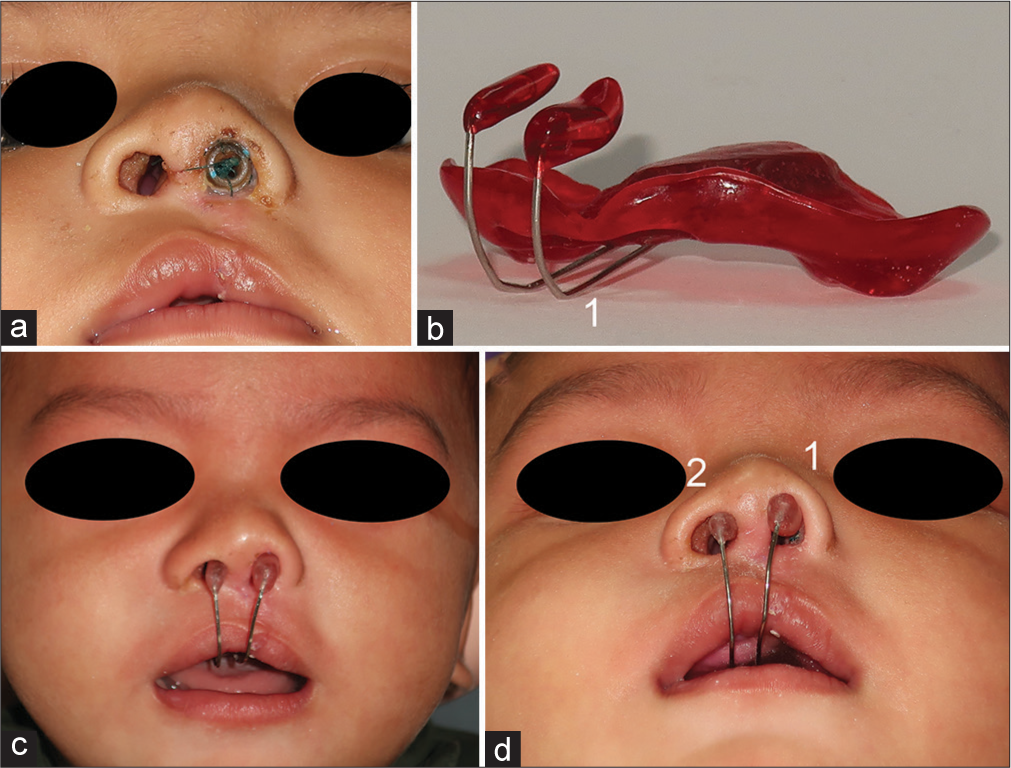
- (a) The customized nasal conformer before removal from the repaired nose on the cleft side. (b) The Korat-NAM II is different from the Korat-NAM I because there is no coil on the extending arm on the cleft side (b-1). (c) The Korat-NAM II in place at frontal view and (d) submentovertex view. (d-1) Notice the stretching force by the extending arm on the cleft side (d-2) while the extending arm on the non-cleft side only supports the columella and nostril. NAM: Nasoalveolar molding.
Palatoplasty
We use a standard two-flap palatoplasty in conjunction with Furlow’s double opposing Z-plasty[13] and perform a gingivoperiosteoplasty to close the alveolar cleft with a one-layer mucoperiosteal flap (nasal side). The procedure is considered successful if there is a complete separation between the oral and nasal cavity. In addition, the soft palate and pharyngeal muscle can function normally. After palatoplasty, the patient is instructed to wear the Korat-NM III for maintaining the nostril and alar contour for at least 2 years.
Korat-NM III
The Korat-NM III is an extraoral appliance in a head strap design, unlike the Korat-NAM I and II. Before palatoplasty, an impression of the patient’s forehead is taken. A 1-mm spring-hard stainless steel wire is bent to fit the forehead. The width between the two legs is approximately the width of the widest part of the columella. Each leg is curved to be slightly in front, of the nose, and turned 90° at the same level of the upper edge of the nostril on the cleft side, and 2 mm below the upper edge of the nostril on the non-cleft side to form a 4-mm coil on both sides [Figure 4a]. The end of each leg then projects into the nostril with kidney-shaped acrylic on both sides. The shorter leg on the cleft side [Figure 4a-1] pulls the nostril upward, while the other leg [Figure 4a-2] only passively supports the columella [Figure 4b]. The forehead wire part is sewn on an elastic head strap. The appliance is adjusted every 3 months since the wires become loose from repetitive removal and wearing and to compensate for nasal morphology changes. Adjustments were made to maintain nasal morphology with no active force. The adjustment visits last at least 2 years after the palatoplasty.
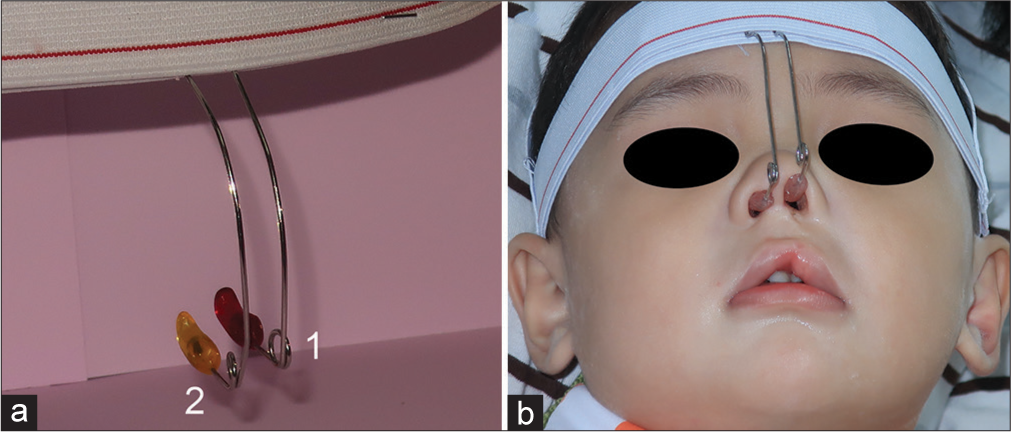
- (a) The Korat-NM III is an extra-oral appliance connected with an elastic head strap. Each wire leg is curved slightly to be in front of the nose with the coil that allows adjustment to accommodate the patient’s facial growth. Notice the slightly shorter leg on the cleft side (a-1) than the non-cleft side (a-2) to pull up the nostril (b) on the cleft side slightly. NM: Nasal molding.
A CASE REPORT OF A PATIENT WITH RIGHT COMPLETE CLP WITH A 5-YEAR FOLLOW-UP
A female patient with a right complete CLP was accepted to the Cleft Center Maharat Nakhon Ratchasima Hospital at 3 days old [Figure 5a-c]. She presented with a 13-mm wide alveolar cleft. Therefore, an active obturator with a retraction screw was worn until she was ready for the Korat-NAM I (when the alveolar cleft size is <3 mm). The Korat-NAM I was inserted and adjusted every 2 weeks. After 6 months, the alveolar cleft was closed and the cleft width on the upper lip was further decreased [Figure 5d-f]. The patient underwent cheiloplasty at 7 months old and retained a customized nasal conformer sutured with the nostril for 3 weeks [Figure 5g-i]. Subsequently, the customized nasal conformer was removed, and the KoratNAM II was inserted. The patient came to the center every month for follow-up appointments until she was ready for palatoplasty [Figure 5j-l]. She underwent palatoplasty at 1 year and 8 months old. Three weeks after palatoplasty, she was instructed to wear the Korat-NM III with a minimum of 2 h a day. Follow-up appointments for appliance adjustments were every 3 months. This patient has been back to the Cleft Center for follow-up appointments for 5 years [Figure 5m-o]. The measurements of nostril height ratio, nostril sill width ratio, and columella angle showed that nasal symmetry between cleft and non-cleft side had been improved, since Korat-NAM 1 was worn. It was overcorrected after primary correction, and had a slight relapse with good stability while wearing KoratNAM II and Korat-NM III [Figure 6 and Table 1].
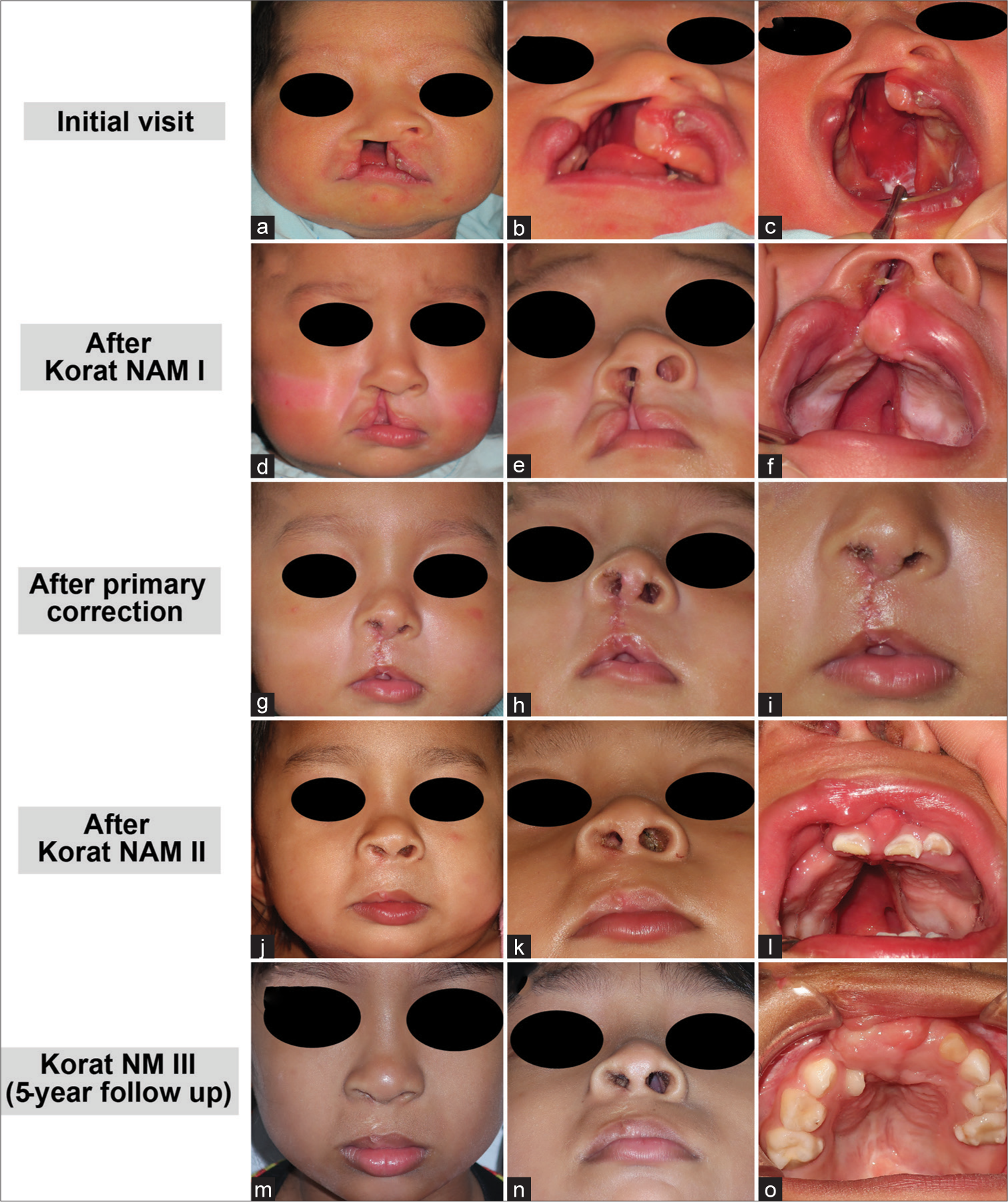
- A case report with a 5-year follow-up: (a-c) A 3-day-old female patient initially presented with a right complete cleft lip and palate. (d-f) She wore the Korat-NAM I until immediately before primary correction. (g-i) Right after primary correction, a customized nasal conformer was sutured and retained for 3 weeks. (j-l) After that she wore the Korat-NAM II until immediately before palatoplasty. (m-o) After palatoplasty, she was instructed to wear the Korat-NM III. NAM: Nasoalveolar molding, NM: Nasal molding.
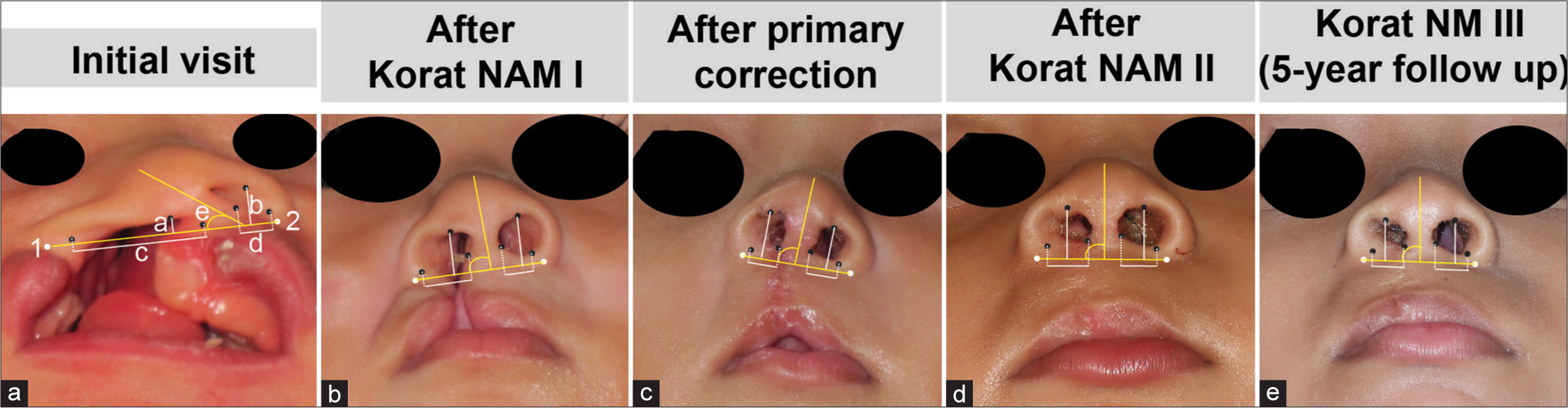
- Measurements of nose on the cleft side (right nostril) and non-cleft side (left nostril) are shown. (a) Measurements were performed at the initial visit, (b) after wearing Korat NAM I until before the primary correction, (c) after primary correction, (d) after wearing Korat NAM II until before palatoplasty, and (e) after wearing Korat NM III for 5 years. (a-a and b) The nostril height, (a-c and d) the nostril sill width, and (a-e) the columella angle of the cleft side (a1-2) were measured to the line connecting between left and right mid-alar bases. NAM: Nasoalveolar molding, NM: Nasal molding.
| Nostril height | Nostril sill width | Columella angle (degrees) | |||||
|---|---|---|---|---|---|---|---|
| Cleft side (C) | Non-cleft side (N) | Ratio (C/N) | Cleft side (C) | Non-cleft side (N) | Ratio (C/N) | ||
| Initial visit | 151.38 | 363.04 | 0.417 | 1212.77 | 319.65 | 3.794 | 40 |
| After Korat NAM I | 386.23 | 467.72 | 0.826 | 460.97 | 256.59 | 1.797 | 85 |
| After primary correction | 414.24 | 362.89 | 1.142 | 249.31 | 242.01 | 1.03 | 97 |
| After Korat NAM II | 352.47 | 359.98 | 0.979 | 327.8 | 253.14 | 1.295 | 88 |
| Korat NM III (5-year follow-up) | 371.53 | 406.42 | 0.914 | 346.58 | 285.79 | 1.213 | 85 |
NM: Nasal molding after NAM: Nasoalveolar molding, NAM: Nasoalveolar molding, NM: Nasal molding
DISCUSSION
Korat modification of NAM appliance
The original NAM appliance mainly consists of acrylic that has to be thick enough to achieve adequate strength. Our Korat-NAM replaces the acrylic extension arms with wires that reduce the bulkiness of this part of the appliance for patients’ acceptance and comfort. In addition, these wires extend from the occlusal surface of the plate instead of the labial surface like other previously modified NAM appliances.[14] This is possible because the thickness of the acrylic bite block, which is a unique design of Korat-NAM, allows freeway space. This wire position also helps with feeding by locking the nipple in place and squeezing out the milk. The force during sucking and biting could be transferred from the plate to the extending arms toward the acrylic nostril part that can stretch the nostril, especially on the cleft side. In addition, it could also stretch the upper lip forward that may reduce the compression force on the maxilla and allow forward maxillary growth (forward displacement of the maxilla).[15] However, these effects require further studies to validate these hypotheses.
For patients with initial cleft size larger than 10 mm, we used an active obturator with retraction screw before prescribing the Korat-NAM I, while for patients with initial cleft size between 4 and 10 mm, we used a set-up model to align the alveolar segments during Korat-NAM I wearing. This set-up model reduces the chair time for appliance adjustment visits, since the addition and removal of acrylic is not required like other NAMs.
Another modification that could be an advantage is that the Korat-NAM also has an extending arm that goes into the non-cleft side nostril to support the columella, unlike other NAMs. It supports columella with no active push force. We experienced that without this supporting arm on the non-cleft side, the columella tended to collapse to the non-cleft side when stretching the nostril on the cleft side. Therefore, this could reduce the asymmetry between the cleft and non-cleft sides due to relapse and tension. In addition, the thread ends in the Korat-NAM I that projects towards the medial side could pull the nostril on the cleft side medially, which may counteract the tension force direction from relapse. Furthermore, having two extended arms increases appliance retention and helps lock the nipple during feeding.
We use traditional acrylic without soft acrylic for fabricating the Korat-NAM to achieve high strength, improve its hygiene, and eliminate chair-side adjustments. In terms of overall cost per appliance, our Korat-NAM is cheaper because no soft denture liner (soft acrylic) is required, unlike the conventional NAM appliance. However, a small amount of denture adhesive is required in the Korat-NAM II.
In addition to maintaining nasal morphology after primary correction, Korat NAM II serves as an obturator while the patient is waiting for palatoplasty that also improves tongue position and function,[16] unlike other kinds of nasal conformer.
Clinical chair time is decreased with our Korat-NAM because the nasal acrylic part is prefabricated and the appliance is quite easy for doctors and parents to insert. Therefore, the Korat-NAM can be delivered on the same day to reduce the number of clinic visits. However, an extensive amount of laboratory work is still required. Therefore, the laboratory technician is a key person in fabricating this appliance. Although digital NAM is becoming more popular nowadays,[17,18] we experience that not all hospitals can afford the cost of an intraoral scanner and a 3D printer. Therefore, the conventional way of fabricating NAM is still essential.
Longer NAM usage may accommodate cheiloplasty and minimize relapse after surgery
The NAM is usually used early when the cartilage is soft enough to be molded before primary correction. This molding is possible due to the effect of high levels of estrogen and hyaluronic acid early after birth.[19,20] A previous study demonstrated that the NAM could be used at a later age; however, the molding result was not as good as when its use began earlier.[21] At our center, we start using the Korat-NAM in CLP patients early after birth. However, the main difference in the Korat-NAM use is the duration. The Korat-NAM also has modifications that can be used after primary correction and palatoplasty, unlike other NAMs that are indicated to be used only before primary correction. We observed a decrease in postsurgical relapse, and improvement in symmetry between the cleft and non-cleft side in patients with a full course of Korat-NAM appliance use together with modified surgical techniques at our center (ongoing data collection and analysis).
After primary correction, some patients are prescribed a nasal conformer to maintain their nose morphology and prevent relapse due to scar tissue and muscle force. However, typically, it is maintained for a short period that may not be enough to prevent relapse after surgery, and a revision surgery is required. In addition, the nasal conformer can be easily removed by the patients because it is removable and small. Other centers recommend using a nasal conformer for a maximum of 6 months after primary correction.[22] The Korat-NAM II is prescribed to be used after primary correction until the patients undergo palatoplasty, which is longer than 6 months. In addition, the Korat-NAM II can be worn more easily than the nasal conformer because the patients previously wore the Korat-NAM I. Furthermore, we use a customized nasal conformer for 3 weeks to effectively maintain the nasal morphology before switching to the Korat-NAM II. This customized nasal conformer is made from an endotracheal tube instead of a commercial nasal conformer, which can reduce cost. Subsequently, the KoratNM III is recommended to be used as long as the patients can tolerate it (the longest period we have observed is 10 years) to maintain nose morphology and prevent relapse. However, we instruct patients to strictly wear it at least for 2 years after surgery since the rate of relapse is high in the 1st year after surgery.[23] After that we experienced that most patients could not wear Korat-NM III as expected due to social activities which changed with age. Patients wanted to play outside with friends, and they no longer wanted to wear the appliance. Therefore, we designed as a head strap to be easily worn and encouraged them to wear only 2 h a day while they were home. The exact amount of wearing time to perfectly maintain the nostril shape after surgery still requires further studies.
Burden of care
In the viewpoint of the burden of care from using KoratNAM, it is the fact that we cannot avoid it in several aspects including multiple visits, patient discomfort, and financial cost.[6] In terms of multiple visits, we found that every clinic visit for appliance adjustment, helped reinforce parents by seeing improvement in the oral hygiene of their children. As mentioned in the study by Magyar et al., social support is an essential factor for treatment outcomes.[24] In addition, we schedule the adjustment visits so that several parents come in on the same day and help reinforce and share knowledge with each other. Moreover, with Korat-NAM, we can reduce chair time of appliance fabrication and adjustments as mentioned previously. More importantly, patients were also scheduled with other clinics on the same day, such as speech therapy and pediatric dentistry to minimize the overall hospital visits. In terms of patient discomfort, we modified the Korat-NAM appliance to a less bulky design and increased retention to minimize the use of taping that usually causes irritation. In terms of financial cost, Korat-NAM appliance costs and transportation costs to the hospital were covered by the government. Therefore, after weighing risks and benefits, we still recommend using Korat NAM in conjunction with surgery for CLP correction.
Primary correction and palatoplasty
With the Korat-NAM appliance, patients would present with well-aligned alveolar segments with a narrow gap, appropriate nose tip projection, and sufficient lip tissue that improve the esthetics and success of the primary correction. At the skin layer, we use the Millard rotation advancement technique with modification of Fisher’s technique which makes the scar line appear to be a philtrum ridge, and minimizes the scar contraction that may affect the vertical lip height. The key step in primary cleft lip and nose repair is the muscle layer repair. We release the muscle and alar base from the maxilla and nasal aperture rim and completely reconstruct the muscle from the upper to the lower part of the lip. The upper part of the orbicularis muscle is reconstructed to achieve nostril sill fullness and overcorrect the nostril sill width by approximately 20% to prevent relapse from the nasal cleft deformity.[25] For the primary rhinoplasty, we approach using Tajima’s reverse U-incision to realign the lower lateral cartilage on the cleft side and perform suture plication with the unaffected side to achieve nasal tip projection and elongate the columella on the cleft side. This procedure is considered an overcorrection of the nostril height. The customized nasal conformer is retained for 3 weeks to temporarily support the nostril and minimize the nasal mucosa swelling. To maintain the nostril height for a longer period of time, the Korat-NAM II is suggested.
With the Korat-NAM appliance and a well-reconstructed orbicularis muscle, we experienced that patients at ~1.5 years old would present with well-aligned alveolar segments with a narrow gap that accommodates the palatoplasty.
CONCLUSION
Korat-NAM can be an alternative pre-surgical orthopedic appliance for patients with a UCLP with the advantages of reduced clinical chair time, accommodating feeding, ease of appliance insertion, reduced cost, and decreased relapse after surgery.
Acknowledgment
We thank Dr. Kevin Tompkins for critically reviewing and editing the manuscript.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Burden of care: Management of cleft lip and palate. Indian J Plast Surg. 2019;52:343-8.
- [CrossRef] [PubMed] [Google Scholar]
- The burden of care for children with unilateral cleft lip: A systematic review of revision surgery. Cleft Palate Craniofac J. 2016;53:84-94.
- [CrossRef] [PubMed] [Google Scholar]
- Revisional techniques for secondary cleft lip deformities. Semin Plast Surg. 2021;35:65-71.
- [CrossRef] [PubMed] [Google Scholar]
- Nasoalveolar molding for infants born with clefts of the lip, alveolus, and palate. Clin Plast Surg. 2004;31:149-58, vii
- [CrossRef] [PubMed] [Google Scholar]
- Nasoalveolar molding improves long-term nasal symmetry in complete unilateral cleft lip-cleft palate patients. Plast Reconstr Surg. 2009;123:1002-6.
- [CrossRef] [PubMed] [Google Scholar]
- Assessing burden of care in the patient with cleft lip and palate: Factors influencing completion and noncompletion of nasoalveolar molding. Cleft Palate Craniofac J. 2019;56:759-65.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiologic study of oral cleft in maharatnakornratchasima hospital between 2005-2009. J Thai Assoc Orthod. 2010;9:3-13.
- [Google Scholar]
- The millard rotation-advancement cleft lip repair: 50 years of modification. Cleft Palate Craniofac J. 2015;52:e188-95.
- [CrossRef] [PubMed] [Google Scholar]
- Fifty years of the Millard rotation-advancement: Looking back and moving forward. Plast Reconstr Surg. 2009;123:1364-77.
- [CrossRef] [PubMed] [Google Scholar]
- Unilateral cleft lip repair: An anatomical subunit approximation technique. Plast Reconstr Surg. 2005;116:61-71.
- [CrossRef] [PubMed] [Google Scholar]
- Reconstruction of vermilion in unilateral and bilateral cleft lips. Plast Reconstr Surg. 1984;73:52-61.
- [CrossRef] [PubMed] [Google Scholar]
- Reverse-U incision for secondary repair of cleft lip nose. Plast Reconstr Surg. 1977;60:256-61.
- [CrossRef] [PubMed] [Google Scholar]
- Cleft palate repair by double opposing Z-plasty. Plast Reconstr Surg. 1986;78:724-38.
- [CrossRef] [PubMed] [Google Scholar]
- A modified nasoalveolar molding technique for correction of unilateral cleft nose deformity. J Craniomaxillofac Surg. 2015;43:2100-5.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of lip repair on maxillary growth and facial soft tissue development in patients with a complete unilateral cleft of lip, alveolus and palate. J Craniomaxillofac Surg. 2006;34:355-61.
- [CrossRef] [PubMed] [Google Scholar]
- Use of a feeding obturator for infants with severe cleft lip and palate. Spec Care Dentist. 1982;2:116-20.
- [CrossRef] [PubMed] [Google Scholar]
- Full digital workflow of nasoalveolar molding treatment in infants with cleft lip and palate. J Craniofac Surg. 2020;31:367-71.
- [CrossRef] [PubMed] [Google Scholar]
- A novel method for fabricating nasoalveolar molding appliances for infants with cleft lip and palate using 3-dimensional workflow and clear aligners. Am J Orthod Dentofacial Orthop. 2020;158:452-8.
- [CrossRef] [PubMed] [Google Scholar]
- Nonsurgical correction of congenital auricular deformities in the early neonate: A preliminary report. Plast Reconstr Surg. 1984;73:38-51.
- [CrossRef] [PubMed] [Google Scholar]
- Preoperative non-surgical over-correction of cleft lip nasal deformity. Br J Plast Surg. 1991;44:5-11.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of early onset nasoalveolar molding with patients who presented for molding up to 1 year of age. J Oral Maxillofac Surg. 2016;74:811-27.
- [CrossRef] [PubMed] [Google Scholar]
- The progressive changes of nasal symmetry and growth after nasoalveolar molding: A three-year follow-up study. Plast Reconstr Surg. 2004;114:858-64.
- [CrossRef] [PubMed] [Google Scholar]
- Stability of nasal symmetry following primary cleft lip and nasal repair: Five years of follow-up. Int J Oral Maxillofac Surg. 2023;52:451-9.
- [CrossRef] [PubMed] [Google Scholar]
- The burden of care in nasoalveolar molding treatment in cleft patients. Indian J Plast Surg. 2022;55:87-91.
- [CrossRef] [PubMed] [Google Scholar]
- Symmetry of the nose after pre-surgical nasoalveolar molding in infants with unilateral cleft lip and palate: A preliminary study. Cleft Palate Craniofac J. 2005;42:658-63.
- [CrossRef] [PubMed] [Google Scholar]




