

Translate this page into:
Relationship between malocclusion and state of the upper respiratory tract, position of the tongue and hyoid bone
 , Vira Kuroiedova1, Yuliya Sokolohorska-Nykina1, Yevhenii Vyzhenko1, Pavlo Korobov1
, Vira Kuroiedova1, Yuliya Sokolohorska-Nykina1, Yevhenii Vyzhenko1, Pavlo Korobov1

*Corresponding author: Oleksii Stasiuk, Department of Postgraduate Education of Orthodontists, Poltava State Medical University, Poltava, Ukraine. o.stasiuk@pdmu.edu.ua
-
Received: ,
Accepted: ,
How to cite this article: Stasiuk O, Kuroiedova V, Sokolohorska-Nykina Y, Vyzhenko Y, Korobov P. Relationship between malocclusion and state of the upper respiratory tract, position of the tongue and hyoid bone. APOS Trends Orthod. doi: 10.25259/APOS_241_2024
Abstract
Objectives
Malocclusions are among the main dental diseases and take second place after dental caries. The etiological factors for the occurrence of malocclusion include genetic factors, environmental and socioeconomic factors, as well as various bad childhood habits. Diseases of the upper respiratory tract deserve special attention, which can lead to oral breathing and the formation of malocclusion. Studying the relationship between craniofacial skeletal characteristics, position of the tongue and hyoid bone, and state of the upper respiratory tract, as a complex of interrelated factors, can become a new tool for diagnosing the etiopathogenesis of malocclusions and contribute to increasing the effectiveness of orthodontic treatment.
Material and Methods
We performed 67 cone beam computed tomography of the facial skeleton of orthodontic patients. The average age was 16.7 ± 5.1 years. Research of the respiratory tract was carried out at the level of standard anatomical landmarks on mid-sagittal sections at the level of the palatal plane, the base of the soft palate, and the base of the epiglottis. The position of the hyoid bone was studied by linear and angular parameters. The size and position of the tongue were measured on a mid-sagittal section along the residual space of Donders.
Results
It has been reliably established that in the II class, upper and middle airways are significantly narrower than in the III class. The Donders space is the largest in the I class - 5.91 ± 4.5 mm, the smallest in the III class - 2.99 ± 3.3 (P = 0.049), that is, the tongue occupies a higher position in the III class than in the I class. The vertical position of the hyoid bone, both in terms of distance from the palatal plane and relative to the C3Me plane, is significantly lower in the I class than in the III class. Therefore, retroposition of the mandible may narrow the pharyngeal airway by moving the hyoid bone backward, while forward displacement of the mandible may increase this space.
Conclusion
Thus, assessment of the upper respiratory tract in patients with malocclusion is important for determining the orthodontic treatment plan.
Keywords
Malocclusion
Upper respiratory tract
Hyoid bone
Position of the tongue
Cone beam computed tomography
Cephalometric analysis

This study is a fragment of the Scientific Research Work (SRW) “Features of rehabilitation of orthodontic patients of various ages” 2023–2028 № 0122U201229.
INTRODUCTION
In the world, malocclusions are among the main dental diseases and take second place after dental caries. According to research results, orthognathic occlusion at any age is only 5–7%.[1] The etiological factors for the occurrence of malocclusion include genetic factors[2], environmental and socio-economic factors[3,4], as well as various bad childhood habits.[5]
Many researchers point to the influence of general somatic pathology on the occurrence of dental diseases and the development of the maxillofacial system.[6,7] To increase the effectiveness and stability of orthodontic treatment, it is important to consider its etiological factor at the beginning.[8,9] Diseases of the upper respiratory tract deserve special attention, which can lead to mouth-type breathing and the formation of malocclusion.[10,11] According to Festa et al.[12] in children with otorhinolaryngological pathology and oral type of breathing, the presence of malocclusion is 81.4%. Such changes lead to a violation of the tongue position in the oral cavity, which complicates orthodontic treatment.
The ratio of the root of the tongue and the soft palate is an important parameter in determining functional impairment. Normally, the tip of the tongue rests against the front part of the hard palate with sagittal abnormalities of occlusion and mouth breathing, position of the tip of the tongue changes, and the back of the tongue is placed lower, so the space between it and the hard palate increases.
Some studies prove a close relationship between structures of the pharynx, the position of the tongue, and malocclusionss in patients with obstructive sleep apnea.[13]
The position of the hyoid bone relative to the skull base and lower jaw is also an indicator of the position and function of the tongue and can lead to changes in alveolar structures.[14,15]
The study of the relationship between craniofacial skeletal characteristics, position of the tongue, and hyoid bone and condition of the upper respiratory tract, as a complex of interrelated factors, can become a new tool for diagnosing the etiopathogenesis of malocclusion and contribute to increasing the effectiveness of orthodontic treatment.
The purpose of our study was to investigate the condition of the upper respiratory tract and position of the tongue and hyoid bone in patients with malocclusions and to establish a relationship between themselves and sagittal, vertical, and transverse inconsistencies of the facial skeleton.
MATERIAL AND METHODS
This retrospective cross-sectional study was approved by the Biomedical Ethics Commission of Poltava State Medical University No. 228 dated June 20, 2024. Materials of the work comply with the Rules of Humane Treatment of Patients in accordance with the requirements of the Tokyo Declaration of the World Medical Association, international recommendations of the Helsinki Declaration on Human Rights, the Convention of the Council of Europe on Human Rights and Biomedicine, the Laws of Ukraine, and requirements of the Ethic Code of Ukrainian Doctor. All research participants gave written consent to the processing and use of data for educational and scientific purposes.
A total of 67 patients took part in the study, during 2020– 2024 and applied to the department of post-graduate education of orthodontists of Poltava State Medical University for orthodontic help. The average age of the subjects was 16.7 ± 5.1 years: Women 39 (17.6 ± 5.3 years) and men 28 (15.6 ± 4.7 years).
Inclusion criteria were men and women with occlusion pathology of class I, II, III.
Exclusion criteria were persons with maxillofacial trauma and congenital facial defects; (2) previously orthodontically treated; (3) patients with obvious facial asymmetry and deviation of the chin by more than 5 mm from the midline of the face.
To achieve the goal, we performed cone beam computed tomography (CBCT) of the facial skeleton of orthodontic patients using the Veraview X800 (J Morita) tube voltage 90 kV, tube current 10 mA, scanning time 20–30 s, slice thickness 1 mm. Images were archived in Digital Imaging and Communications in Medicine format and imported into EZ3D + software to render CBCT files.
All measurements were performed directly on the CBCT. To standardize the process, the 3D image was first centered: The Frankfurt plane was set parallel to the axial plane, and the sagittal plane was aligned with the midline. All studied parameters, which were performed in the sagittal window on the mid-sagittal section, are shown in [Table 1 and Figure 1].

- The studied parameters in the sagittal window. Skeletal indicators: SNA, SNB, ANB, NSBa, SNGoGn; Upper respiratory tract: (1) Nasopharynx (n1–n2), (2) Oropharynx (o1–o2), (3) Hypopharynx (h1–h2); Position of the hyoid bone: C3MeH, NSH, PnsH; Position of the tongue: Donder’s space. SNA: Sagittal position of the upper jaw, SNB: Sagittal position of the lower jaw, ANB: Sagittal jaw relationship, NSBa: Cranial base angle, SNGoGn: Angle between cranial plane and mandibular plane
| Parameter | Description | Value |
|---|---|---|
| Skeletal indicators | ||
| SNA | Angle between points S (Sella Turcica), N (Nasion) and A (Subspinale) | Characterizes sagittal position of the upper jaw relative to the base of the skull |
| SNB | Angle between points S, N, and B (Supramentale) | Characterizes sagittal position of the lower jaw relative to the base of the skull |
| ANB | Angle between points S, N, B | Characterizes sagittal relationship of the apical bases of the jaws among themselves |
| NSBa | Angle between points N, S, and Ba (Basion) | Angle of the base of the skull |
| SNGoGn | Angle between planes SN (cranial plane) and GoGn (mandibular plane between Gonion and Gnation points) | Characterizes the growth type of the facial skeleton |
| Study of state of the upper respiratory tract | ||
| Nasopharynx (mm) | Distance from the front edge of the upper airway at the level of the palatal plane to the nearest laryngeal wall (n1–n2) | Width of the upper part of the pharynx |
| Oropharynx (mm) | Distance between the front and back walls of the upper airway at the level of the soft palate (o1–o2) | Width of the middle part of the pharynx |
| Hypopharynx (mm) | Distance between the front and back walls of the upper airway at the level of the epiglottis (h1–h2) | Width of the lower pharynx |
| Study of the hyoid bone position | ||
| PnsH (mm) | Distance from point H (upper anterior point of hyoid bone) to point Pns (Spina nasalis posterior) | Characterizes vertical position of the hyoid bone |
| NSH | Angle between points N, S i H | Characterizes anteriorposterior position of thehyoid bone |
| C3MeH | Angle between points C3 (anterior upper point of the third cervical vertebra) Me (Menton) and H | Characterizes position of the hyoid bone relative to the C3Me plane |
| Study of the tongue position | ||
| Donders | Distance between the back of the tongue and the hard palate in the direction of the perpendicular lowered from the intercuspular fissure of the first permanent molar to the plane of the base of upper jaw Spp (the plane between the points Ans – Spina nasalis anterior and Pns) | Characterizes position of the tongue |
Cephalometric analysis of skeletal parameters
The study of skeletal cephalometric indicators was carried out on the sagittal section of CBCT with the help of “Angle” and “Ruler” tools.
In the sagittal plane, all patients were divided into skeletal classes according to ANB angle.[16] Anteroposterior skeletal pattern: Class I – ANB angle between 0° and 4°, Class II – ANB >4°, Class III – ANB <0°.
Depending on the SNGoGn angle index, patients were divided by growth type[16] – vertical skeletal pattern: Normal – SNGoGn angle between 28° and 36°; hyperdivergent – SNGoGn>36°; hypodivergent – SNGoGn <28°.
Examination of the respiratory tract
Measurements were made at the level of standard anatomical landmarks on mid-sagittal sections at the level of the palatal plane, the base of the soft palate, and the base of the epiglottis. Thus, the respiratory tract is divided into three areas: (1) Nasopharynx (upper from the palatal plane), (2) oropharynx (between the palatal plane and the base of the soft palate at the most anterior point), and (3) hypopharynx (between the base of the soft palate and the base epiglottis).[17]
Width of the upper part of the pharynx (Nasopharynx section) was measured on mid-sagittal and axial sections at the level of the palatal plane to the nearest laryngeal wall.
Middle section (Oropharynx) – at the level of the soft palate (the base of the soft palate).
Width of the lower part of the pharynx (Hypopharynx) was measured at the level of the epiglottis (base of the epiglottis).
Study of the hyoid bone position
The position of the hyoid bone was studied by linear and angular parameters.[18]
According to the C3MeH angle index, all patients are divided into 2 groups: group 1, when the hyoid bone is located above the C3Me plane, and group 2 – the hyoid bone is located below the C3Me plane. The lower the location of the hyoid bone, the higher the risk of developing a narrowing of the airway.
Study of the tongue position
Size and position of the tongue were measured on a mid-sagittal section along the residual Donders space – the distance between the back of the tongue and the hard palate in the direction of a perpendicular lowered from the intercuspatory fissure of the first permanent molar to the plane of the base of the upper jaw.[19]
Transversal skeletal characteristic
Characteristics of the jaws in the transverse plane were studied on the coronal section of the 3D CBCT according to the method of the University of Pennsylvania[20] [Table 2 and Figure 2].
| Landmark/parameter | Definition |
|---|---|
| Maxillary landmark | The intersection point of the cut line withthe cortical plate on axial slice while the cut line passes through MxRMxL (the junction of the maxilla and zygomatic buttress) on coronal slice |
| Point of intersection of the cut line with the cortical plate on the axial section, while the cut line passes through MxRMxL (junction of the maxilla and the zygomatic support) on the coronal section. | |
| Mandibular landmark | The intersection point of the cut line withthe cortical plate on axial slice while the cut line passes through the furcation of mandibular first molars on coronal slice (MdRMdL) |
| Point of intersection of the cut line with the cortical plate on the axial section and the cut line passes through the furcation of the mandibular first molars on the coronal section | |
| Maxillary width (mm) | Linear distance between two maxillary landmarks. |
| Linear distance between two maxillary landmarks | |
| Mandibular width (mm) | Linear distance between two mandibular landmarks. |
| Linear distance between the two landmarks of the lower jaw. | |
| Transverse measurement in CBCT transverse analysis | The difference between maxillary width and mandibular width Normal≥5 mm |
CBCT: Cone beam computed tomography, MxR-MxL: Linear distance between two maxillary landmarks; MdR-MdL: Linear distance between two mandibular landmarks
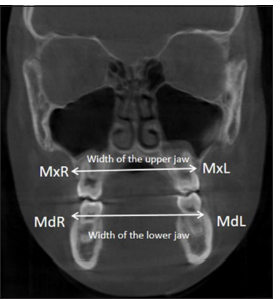
- Transversal skeletal pattern: MxRMxL – Linear distance between two maxillary landmarks; MdR-MdL – Linear distance between two mandibular landmarks.
According to the indicator of the ratio of the upper and lower jaws (the difference between maxillary width and mandibular width), all patients are divided into two groups: group 1– no discrepancy, if the size of the upper jaw was equal to or >5 mm in relation to the lower jaw and group 2 – when a narrowing of the upper jaw or a discrepancy in size of the jaws was determined, if its transverse size is <5 mm in relation to the transverse size of the lower jaw.
14 cephalometric measurements were performed on the CBCT of each patient; a total of 938 measurements were performed.
Examiner reliability and statistical analysis
Statistical data processing was carried out in open statistical software for the desktop Jamovi version 2.3.28.0 free license.[21]
Tracing of cephalometric points and cephalometric measurements were carried out independently by 2 orthodontists (10 and 12 years of experience). Interexaminer verification of cephalometric measurements was carried out by comparing mean values using the t-test of independent samples. According to the results of the test, the level of significance for all measurements was P > 0.05, therefore, in the future, the averaged data between two researchers were used. A study of the sample for the normality of the data distribution was carried out using exploratory analysis according to the Shapiro–Wilk test. The relationship between the studied parameters was determined using the Spearman correlation coefficient. One-way analysis of variance (ANOVA) with Welch’s non-parametric correction was performed to compare indicators between skeletal bite characteristics. Pearson’s χ2 test was used to study the position of the hyoid bone with different skeletal characteristics. A result of P < 0.05 was considered statistically significant.
RESULTS
According to the results of cephalometric analysis, the distribution of patients into skeletal groups showed the following: According to the skeletal characteristics of occlusion in the sagittal plane: Class I - 27 patients, class II - 24, class III – 16; according to the type of growth: Hypodivergent - 36, normal - 26, and hyperdivergent – 5; and in the transverse plane: patients who did not have intermaxillary inconsistencies - 7, with existing inconsistencies - 60.
[Table 3] presents the correlations that had statistical significance.
| Parameter | Spirmen | Naso-pharynx | Orop-harynx | Hypo-pharynx | NSH | PnsH | C3MeH | Donders |
|---|---|---|---|---|---|---|---|---|
| Hypo pharynx | Po | 0.074 | 0.468*** | — | ||||
| P-value | 0.552 | <0.001 | — | |||||
| C3MeH | Po | 0.075 | 0.082 | -0.225 | 0.072 | 0.605*** | — | |
| P-value | 0.545 | 0.509 | 0.068 | 0.561 | <0.001 | — | ||
| Donders | Po | 0.042 | 0.127 | -0.034 | -0.009 | 0.288* | 0.292* | — |
| P-value | 0.734 | 0.306 | 0.782 | 0.945 | 0.018 | 0.017 | — | |
| SNB | Po | 0.139 | 0.241* | 0.156 | -0.287* | -0.128 | -0.208 | -0.092 |
| P-value | 0.263 | 0.049 | 0.209 | 0.018 | 0.302 | 0.092 | 0.461 | |
| SNGoGn | Po | -0.210 | 0.064 | 0.130 | 0.277* | 0.167 | -0.099 | 0.079 |
| P-value | 0.088 | 0.609 | 0.293 | 0.023 | 0.177 | 0.426 | 0.526 | |
| NSBa | Po | 0.119 | 0.127 | -0.073 | 0.242* | -0.082 | 0.321** | -0.051 |
| P-value | 0.339 | 0.308 | 0.555 | 0.048 | 0.510 | 0.008 | 0.681 | |
| Width of the upper jaw | Po | -0.269* | -0.141 | -0.041 | -0.273* | -0.049 | 0.003 | -0.083 |
| P-value | 0.028 | 0.255 | 0.744 | 0.026 | 0.694 | 0.980 | 0.505 |
According to the results of the correlation analysis, there is an inverse weak relationship between the width of the upper part of the pharynx (Nasopharynx) and the width of the upper jaw (Spirmen coefficient Po = −0.269, P = 0.028). Width of the middle part (Oropharynx) inverse weak correlates with the SNB angle (Po = −0.241, P = 0.049).
The NSH angle had an inverse weak correlation with the SNB angle (Po = −0.287, P = 0.018), NSBa angles (Po = −0.242, P = 0.048), SNGoGn angles (Po = −0.277, P = 0.023), and with width of the upper jaw (Po = −0.273, P = 0.026). The PnsH indicator has an inverse moderate relationship with the C3MeH angle (Po = −0.605, P < 0.001) and an inverse weak correlation with the position of the tongue (Donders) (Po = −0.288, P = 0.018).
The C3MeH angle has an inverse significant correlation with the NSBa angle (Po = −0.321, P = 0.008) and an inverse weak relationship with tongue position (Donders) (Po = −0.292, P = 0.017).
To compare indicators of state of the upper respiratory tract, position of the tongue, and hyoid bone with different skeletal characteristics in three planes, ANOVA analysis with Welch’s non-parametric correction was performed.
A comparison of parameters of the upper respiratory tract, position of the tongue, and the hyoid bone in different classes of malocclusions in the sagittal plane is shown in [Table 4].
| Parameter | Skeletal class | Mean±SD | P-value |
|---|---|---|---|
| Nasopharynx | I class | 14.43±4.29 | P1=0.821 |
| II class | 13.738±3.95 | P2=0.160 | |
| III class | 16.469±2.83 | P3=0.039* | |
| Oropharynx | I class | 10.256±2.90 | P1=0.745 |
| II class | 9.617±3.27 | P2=0.113 | |
| III class | 12.219±3.06 | P3=0.039* | |
| Hypopharynx | I class | 11.889±3.93 | P1=0.993 |
| II class | 11.779±3.27 | P2=0.069 | |
| III class | 15.744±5.83 | P3=0.055 | |
| PnsH | I class | 57.296±6.59 | P1=0.393 |
| II class | 54.938±6.21 | P2=0.02* | |
| III class | 52.263±4.99 | P3=0.301 | |
| NSH | I class | 89.233±5.74 | P1=0.098 |
| II class | 92.313±4.67 | P2=0.968 | |
| III class | 88.819±5.22 | P3=0.095 | |
| C3MeH | I class | 174.234±19.7 | P1=0.53 |
| II class | 168.349±17.77 | P2<0.001*** | |
| III class | 154.701±8.22 | P3=0.193 | |
| Donders | I class | 5.907±4.49 | P1=0.107 |
| II class | 3.692±3.08 | P2=0.049* | |
| III class | 2.987±3.29 | P3=0.777 |
It has been reliably established that in II class respiratory tracts of the upper and middle sections are significantly narrower than in III class: Nasopharynx 13.74 ± 3.95 mm and 16.47 ± 2.83 mm, respectively, Oropharynx in II class – 9.62 ± 3.3 mm and in III class – 12.22 ± 3.06 at (P = 0.039). In the lower part of the upper respiratory tract (Hypopharynx), the situation is similar (II class - 11.78 ± 3.3 mm, III class - 15.74 ± 5.8 mm), but there is no statistically significant difference.
The Donders space is the largest in the I class - 5.91 ± 4.5 mm, the smallest in the III class - 2.99 ± 3.3 (P = 0.049), that is, the tongue occupies a higher position in the III class than in the I class.
The vertical position of the hyoid bone both in terms of the distance from the palatal plane and relative to the C3Me plane is significantly lower in the first class than in the third class (in the first case P < 0.02, in the second P < 0.001).
A comparison of parameters of the upper respiratory tract, position of the tongue, and hyoid bone in different types of skeletons in the vertical plane is shown in [Table 5].
| Parameter | Vertical skeletal pattern | Mean±SD | P-value |
|---|---|---|---|
| Nasopharynx | Hypodivergent | 15.42±3.90 | P1=0.29 |
| Norm | 13.87±4.02 | P2=0.546 | |
| Hyperdivergent | 13.46±3.66 | P3=0.973 | |
| Oropharynx | Hypodivergent | 10,14±3.16 | P1=0.724 |
| Norm | 10,80±3.45 | P2=0.454 | |
| Hyperdivergent | 11,42±1.92 | P3=0.842 | |
| Hypopharynx | Hypodivergent | 11,82±3.63 | P1=0.268 |
| Norm | 13.77±5.49 | P2=0.389 | |
| Hyperdivergent | 14.38±3.73 | P3=0.949 | |
| PnsH | Hypodivergent | 54.59±6.98 | P1=0.952 |
| Norm | 55.05±5.16 | P2=0.079 | |
| Hyperdivergent | 61.08±4.84 | P3<0.01** | |
| NSH | Hypodivergent | 88,5±4.34 | P1=0.033* |
| Norm | 92.00±5.67 | P2=0.36 | |
| Hyperdivergent | 93.70±7.43 | P3=0.871 | |
| C3MeH | Hypodivergent | 171±18.74 | P1<0.08 |
| Norm | 161±18.26 | P2=0.988 | |
| Hyperdivergent | 171±5.75 | P3=0.087 | |
| Donders space | Hypodivergent | 3.93±3.29 | P1=0.606 |
| Norm | 4.89±4.28 | P2=0.859 | |
| Hyperdivergent | 5.44±6.18 | P3=0.98 |
According to the results of the analysis, it was reliably established that the position of the hyoid bone is lower in the hyperdivergent type than in the normal type of skeleton (P < 0.01). Regarding the anterior-posterior position, a significant difference was established between patients with hypodivergent and normal types of skeletal growth (P = 0.033).
A comparison of parameters of the upper respiratory tract, position of the tongue and the hyoid bone with different types of skeleton in the transverse plane is shown in [Table 6].
| Parameter | Transverse skeletal pattern | Mean±SD | P-value |
|---|---|---|---|
| Nasopharynx | No discrepancy | 13.26±4.50 | P=0.360 |
| Discrepancy | 14.83±3.95 | ||
| Oropharynx | No discrepancy | 8.41±4.40 | P=0.217 |
| Discrepancy | 10.74±2.98 | ||
| Hypopharynx | No discrepancy | 9.76±2.40 | P=0.004** |
| Discrepancy | 13.12±4.60 | ||
| PnsH | No discrepancy | 56.79±6.17 | P=0.508 |
| Discrepancy | 55.07±6.38 | ||
| NSH | No discrepancy | 89.44±5.87 | P=0.714 |
| Discrepancy | 90.33±5.39 | ||
| C3eH | No discrepancy | 167.37±16.85 | P=0.978 |
| Discrepancy | 167.17±18.77 | ||
| Donders | No discrepancy | 4.59±3.76 | P=0.904 |
| Discrepancy | 4.40±3.96 |
It was established that the width of the respiratory tract in the area of the hypopharynx is significantly greater in patients with a discrepancy in the transverse dimensions of the jaws than in the group with a normal ratio (P = 0.004).
We also performed Pearson’s χ2 test to analyze the position of the hyoid bone relative to the C3Me plane with different skeletal characteristics. The distribution of patients was as follows: group 1 - when the hyoid bone is located above the C3Me plane (n = 54) and group 2 – the hyoid bone is located below the plane (n = 13).
According to the results of Pearson’s χ2 test, a statistically significant difference was established in the skeletal sagittal pattern patient group (P = 0.026): Normal – higher position of the hyoid bone in I class was 18 patients (66.7%), in II class 20 (83.3%) ) and for the III class in 100% [Table 7].
| Skeletal class | |||||
|---|---|---|---|---|---|
| Position of the hyoid bone | n(%) | I class | II class | III class | Total |
| Above the C3Me line | n | 18 | 20 | 16 | 54 |
| % | 66.7 | 83.3 | 100.0 | 80.6 | |
| Below the C3Me line | n | 9 | 4 | 0 | 13 |
| % | 33.3 | 16.7 | 0.0 | 19.4 | |
| Total | n | 27 | 24 | 16 | 67 |
| % | 100.0 | 100.0 | 100.0 | 100.0 | |
χ2 Pirson’s=0.026
DISCUSSION
When planning treatment, it is important to have knowledge about the morphological components of various anomalies of occlusion. The growth and development of the maxillofacial area and the functions of the oral cavity are closely interconnected. Factors of an “unintentional” nature, which constantly act on the maxillofacial and alveolar areas, can cause a general deformation of bone structures, which leads to jaw deformation and malocclusion.
The airways of the pharynx, tongue, and hyoid bone are interconnected. The hyoid bone is connected to the pharynx, mandible, and skull by muscles and ligaments, and its position relative to them determines the position and function of the tongue. Its position also plays an important role in maintaining the respiratory tract, regardless of the class of malocclusion.[18]
Studies in this area show numerous associations between skeletal pathology in the sagittal plane and airway size, which is consistent with the results of our study. The volume and cross-sectional area of the airways in patients with skeletal class II are significantly narrower than in individuals with class I and class III,[22-25] and the largest airway sizes are observed with skeletal malocclusion, class III, which also confirms the results of other studies.[26] We established a statistically significant difference in the size of the respiratory tract between patients of the II class and III class in the naso and oropharyngeal areas (P < 0.05).
Regarding the position of the tongue and hyoid bone, there are a number of studies that patients with skeletal malocclusion of II class, in particular, and III,[24] have a lower position of the tongue and hyoid bone than patients with skeletal I class, but the position of the tongue and hyoid bone was not significantly affected by different types of vertical facial development.[27]
There are conflicting data regarding the position of the hyoid bone. Iwasaki et al.[28] prove that the position of the hyoid bone was lower in skeletal II class patients than in I class patients. Chauhan et al.[25] prove that there was no statistically significant difference in the vertical position of the hyoid bone in malocclusion groups of I class, class II, and III class. According to the results of our research, the lowest position of the tongue and hyoid bone was established in the I class and, conversely, the highest position in the III class, and a statistically significant difference was established between I and II classes.
In this aspect, the study of Kocakara et al. is of interest,[29] who studied not only width but also vertical length of the airways and position of the hyoid bone in different skeletal classes of occlusion and different types of growth and established that width of the pharyngeal airways and position of the hyoid bone are the same in individuals with different classes of malocclusion in the sagittal direction, while the vertical length of the respiratory tract is significantly shorter in patients with III class and hypodivergent type of growth. Such data further explain the relationship between the state of the respiratory tract, the position of the tongue, and the hyoid bone. The higher the position of the tongue and hyoid bone, the shorter the airway, which is typical for class III. Our study also confirmed that in 100% of cases in class III, the hyoid bone has a high position relative to the C3Me plane.
Regarding the connection of the studied parameters with the vertical type of growth, according to the results of our study, the upper respiratory tract in the nasopharyngeal area is the widest in hypodivergent growth type and the narrowest in hyperdivergent growth, and the opposite pattern is observed in the hypopharyngeal area. The largest tongue space was found in patients with hyperdivergent growth, although in both cases without statistical significance. Such data coincide with the results of Ucar and Uysal,[30] who found that with the I skeletal class, the nasopharyngeal space of the respiratory tract (P < 0.01) and the upper oropharyngeal space (P < 0.05) was larger, and the palatal space of the tongue (P < 0.05) was smaller in subjects with hypodivergent type than in patients with a hyperdivergent craniofacial pattern. We established a statistical difference in the NSH angle, which characterizes the position of the hyoid bone in the anterior-posterior direction, between patients with hypodivergent and normal growth.
When analyzing the relationship between the respiratory tract indicators between the groups, which characterize the ratio of the jaws in the transverse plane, a significant decrease in the size of the hypopharyngeal area was established in patients of the group with a normal ratio (P = 0.004). This is explained by the fact that the transverse discrepancy is associated with a narrowing of the upper jaw or with an increase in the width of the lower jaw. Such data may require clarification due to additional studies of the relationship between the dimensions of the lower jaw and condition of the upper respiratory tract.
Some discrepancies between indicators and their correlations in our study with the data of other scientists may be related to different methods of conducting the CBCT study. In particular, some studies have been performed in supine patients, arguing that the epiglottis, soft palate, and esophageal opening move caudally when the patient’s position changes from supine to upright and move backward when the position changes from upright to supine.[18,31]
Another limitation of this study concerns the methodology of airway measurements. There are works that used methods of volumetric visualization and 3D measurement, including the use of additional software.[17,32] In particular, Da Costa et al.[33] found a significant correlation between linear measurements of pharyngeal subareas and hyoid position on lateral cephalograms and multi planar reconstruction (MPR) 3D CBCT reconstructions, and no correlations were observed between volumetric measurements of pharyngeal subareas and hyoid position.
We would also like to note that most of the studies we analyzed were related to the study of the connections of the respiratory tract, tongue, position of the hyoid bone, and malocclusion in the sagittal and vertical planes. The advantages of our study include the fact that the analysis of features of the state of respiratory tract and lingual-hyoid complex was carried out taking into account the development of the craniofacial area in three planes.
The prospect of further research is the study of the relationship between the dimensions of the lower jaw and the state of the upper respiratory tract.
CONCLUSION
According to the results of our study, the condition of the upper respiratory tract is more related to skeletal characteristics. The largest dimensions in all three departments are found in III class and the smallest in the skeletal II class.
The position of the tongue is closely related to the position of the hyoid bone, while its highest (normal) position is established in 100% of cases also in III class and is most characteristic of the hypodivergent type of growth.
Therefore, retroposition of the mandible may narrow the pharyngeal airway by moving the hyoid bone backward, while forward displacement of the mandible may increase this space. Thus, assessment of the upper respiratory tract in patients with malocclusion is important for determining the orthodontic treatment plan.
The prospect of further research is a prospective clinical study of the dynamics of changes in the upper respiratory tract during the treatment of skeletal class II caused by retrognathia of the lower jaw.
Ethical approval
The research/study was approved by the Institutional Review Board at the Biomedical Ethics Commission of Poltava State Medical University, number 228, dated July 20, 2024.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The author(s) confirms that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- The evaluation of heads of temporomandibular joint (TMJ) position in patients with malocclusion. New Armen Med J. 2020;14:48-53.
- [Google Scholar]
- Systematic review on the genetic factors associated with skeletal Class II malocclusion. Indian J Dent Res. 2021;32:399-406.
- [CrossRef] [PubMed] [Google Scholar]
- A short-term approach for promoting oral health of internally displaced children with PTSD: The key is improving mental health-results from a quasi-randomized trial. BMC Oral Health. 2021;21:58.
- [CrossRef] [PubMed] [Google Scholar]
- The influence of chronic stress on periodontal tissues in orthodontic patients in conditions of martial law. Med Perspektivi. 2024;29:127-34.
- [CrossRef] [Google Scholar]
- Bad oral habits: A review of the literature. J Biol Regul Homeost Agents. 2021;35:403-6.
- [CrossRef] [PubMed] [Google Scholar]
- Interdisciplinary approach to diagnostics of malocclusions (review) Wiad Lek. 2019;72:918-22.
- [CrossRef] [PubMed] [Google Scholar]
- Features of physical and sexual development and the state of bone tissue in adolescent girls. Ukrain J Perinatol Pediatr. 2023;96:91-9.
- [CrossRef] [Google Scholar]
- Unilateral maxillary central incisor root resorption after orthodontic treatment for Angle Class II, division 1 malocclusion with significant maxillary midline deviation: A possible correlation with root proximity to the incisive canal. Korean J Orthod. 2020;50:216-26.
- [CrossRef] [PubMed] [Google Scholar]
- Skeletal and airway stability after mandibular setback in patients with mandibular prognathism: A systematic review. Saudi Dent J. 2021;33:169-76.
- [CrossRef] [PubMed] [Google Scholar]
- Skeletal class II malocclusion caused by mouth breathing in a pediatric patient undergoing treatment by interceptive guidance of occlusion. J Int Med Res. 2021;49:3000605211021037.
- [CrossRef] [PubMed] [Google Scholar]
- Associations between skeletal discrepancies, breathing pattern, and upper airway obstruction in Class III malocclusions. Int J Pediatr Otorhinolaryngol. 2023;166:111471.
- [CrossRef] [PubMed] [Google Scholar]
- Association between upper airway obstruction and malocclusion in mouth-breathing children. Acta Otorhinolaryngol Ital. 2021;41:436-42.
- [CrossRef] [PubMed] [Google Scholar]
- Craniofacial and upper airway morphology in adult obstructive sleep apnea patients: A systematic review and meta-analysis of cephalometric studies. Sleep Med Rev. 2017;31:79-90.
- [CrossRef] [PubMed] [Google Scholar]
- Research on the correlation between the size of condyle and occlusion plane in skeletal Class II malocclusions. Clin Exp Dent Res. 2022;8:1547-54.
- [CrossRef] [PubMed] [Google Scholar]
- Three-dimensional evaluation of soft tissues in hyperdivergent skeletal class II females in Guangdong. BMC Med Imaging. 2022;22:56.
- [CrossRef] [PubMed] [Google Scholar]
- The use of cephalometrics as an aid to planning and assessing orthodontic treatment. Am J Orthod. 1960;29:8.
- [CrossRef] [Google Scholar]
- Airway and cephalometric changes in adult orthodontic patients after premolar extractions. Angle Orthod. 2020;90:39-46.
- [CrossRef] [PubMed] [Google Scholar]
- Position of the hyoid bone and its correlation with airway dimensions in different classes of skeletal malocclusion using cone-beam computed tomography. Imaging Sci Dent. 2020;50:105-15.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of changes in intraoral dynamic space (donders space) with myofunctional therapy in skeletal class II division 1 malocclusion: An in vivo study. J Contemp Dent Pract. 2023;24:582-6.
- [CrossRef] [PubMed] [Google Scholar]
- Responsiveness of three measurements in cone-beam computed tomography transverse analyses during both tooth-supported and mini-screw-assisted rapid maxillary expansion. Angle Orthod. 2023;94:39-50.
- [CrossRef] [PubMed] [Google Scholar]
- The jamovi project (Version 2.3) [Computer Software] 2022. Available from: https://www.jamovi.org [Last accessed on 2024 Sep 04]
- [Google Scholar]
- Three-dimensional evaluation of upper airway in patients with different anteroposterior skeletal patterns. Orthod Craniofac Res. 2014;17:38-48.
- [CrossRef] [PubMed] [Google Scholar]
- The airway volume related to the maxillo-mandibular position using 3D analysis. Biomed Res Int. 2021;2021:6670191.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of pharyngeal airway dimension, tongue and hyoid bone position based on ANB angle. Natl J Maxillofac Surg. 2015;6:42-51.
- [CrossRef] [PubMed] [Google Scholar]
- Radiographic evaluation of the hyoid bone position and pharyngeal airway depth in anteroposterior dysplasia. Int J Clin Pediatr Dent. 2019;12:101-6.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of class II and class III skeletal malocclusion on pharyngeal airway dimensions: A systematic literature review and meta-analysis. Heliyon. 2024;10:e27284.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of the position and morphology of tongue and hyoid bone in skeletal Class II malocclusion based on cone beam computed tomography. BMC Oral Health. 2021;21:475.
- [CrossRef] [PubMed] [Google Scholar]
- Relationships among tongue volume, hyoid position, airway volume and maxillofacial form in paediatric patients with Class-I, Class-II and Class-III malocclusions. Orthod Craniofac Res. 2019;22:9-15.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of pharyngeal airway dimensions and hyoid bone position according to craniofacial growth pattern. Cranio. 2022;40:313-23.
- [CrossRef] [PubMed] [Google Scholar]
- Orofacial airway dimensions in subjects with Class I malocclusion and different growth patterns. Angle Orthod. 2011;81:460-8.
- [CrossRef] [PubMed] [Google Scholar]
- The oropharyngeal airway in young adults with skeletal class II and class III deformities: A 3-D morphometric analysis. PLoS One. 2016;11:e0148086.
- [CrossRef] [PubMed] [Google Scholar]
- A 2-year follow-up of changes after bimaxillary surgery in patients with mandibular prognathism: 3-dimensional analysis of pharyngeal airway volume and hyoid bone position. J Oral Maxillofac Surg. 2016;73:340.e1-9.
- [CrossRef] [PubMed] [Google Scholar]
- Correlation between the position of hyoid bone and subregions of the pharyngeal airway space in lateral cephalometry and cone beam computed tomography. Angle Orthod. 2017;87:688-95.
- [CrossRef] [PubMed] [Google Scholar]




