

Translate this page into:
Simple and cost-effective approach for maxillary bilateral posterior intrusion: Nandlal Toshniwal Rural Dental College double intrusion arch
Address for correspondence: Dr. Mayuresh J. Baheti, Department of Orthodontics and Dentofacial Orthopedics, Rural Dental College, Pravara Institute of Medical Sciences, Loni - 413 736, Maharashtra, India. E-mail: mayuresh295@gmail.com
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Prosthodontic rehabilitation of edentulous space is often complicated with overeruption of antagonistic tooth and often requires preprosthodontic intervention. In this context, orthodontic intrusion of the overerupted antagonistic tooth to facilitate prosthodontic rehabilitation is a desirable strategy. Without orthodontic molar intrusion or segmental surgical impaction, restoring the posterior occlusion often entails the need for significant reduction of maxillary molar crown height, with the potential need for costly iatrogenic root canal therapy and restoration. Conventional orthodontic techniques do not intrude posterior teeth effectively, and almost all methods result in anterior extrusion rather than posterior intrusion. This case report describes the treatment of a patient with supra-erupted maxillary right and left first molars intruded with Nandlal Toshniwal Rural Dental College double intrusion arch. The results showed that the biological responses of the teeth and the surrounding bony structures to the intrusion appeared normal and acceptable.
Keywords
Adjunctive orthodontics
maxillary intrusion
Nandlal Toshniwal Rural Dental College intrusion arch
overerupted molars

INTRODUCTION
Supraerupted maxillary molars are a common clinical finding in dental practice. An early loss of any molar is bound to cause supra-eruption of opposing molar into that space. Overeruption of such molar can lead to occlusal interference, functional disturbances and cause great difficulty during prosthetic reconstruction, especially in adult patients.[1] To reconstruct the proper occlusion for the posterior dentition and to maintain periodontal health, an interdisciplinary and comprehensive dental treatment is necessary. In this context, the orthodontic intrusion of the overerupted antagonistic tooth to facilitate prosthodontic rehabilitation is a desirable strategy.
Conventional orthodontic techniques for intrusion require anchorage reinforcement by incorporating multiple teeth, which depend heavily on patient cooperation and usually result in extrusion of other teeth rather than a molar intrusion. However, the task is formidable with routine orthodontic mechanics and control of anchorage is difficult.
In recent years, temporary anchorage device have allowed orthodontists to overcome these drawbacks while avoiding anesthetic full-appliance therapy.[1-3] However, mini-implants and miniplates have certain disadvantages like higher cost, limited area for insertion, and the need for two separate insertion and removal surgeries,[1] insufficient space on the buccal side to insert a mini-implant safely between the roots, especially in the region of the upper molars.[4-5] To overcome these disadvantages, we designed a new intrusion appliance called Nandlal Toshniwal Rural Dental College (NTRDC) double intrusion appliance, where we intruded two molars of both sides simultaneously.
The present case report documents a case of an adult patient who requires prosthetic replacement of posterior teeth. As the roots of premolar and molar were so close, there was very less interdental bone to place the implant. Hence, it was an ideal case to use such appliance for the intrusion of posterior teeth where the other modern methods were difficult to apply.
CASE REPORT
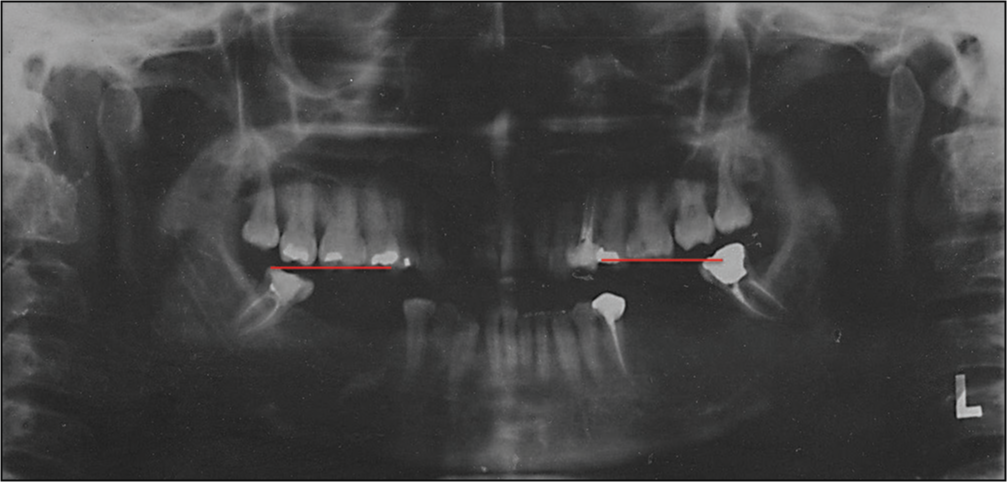
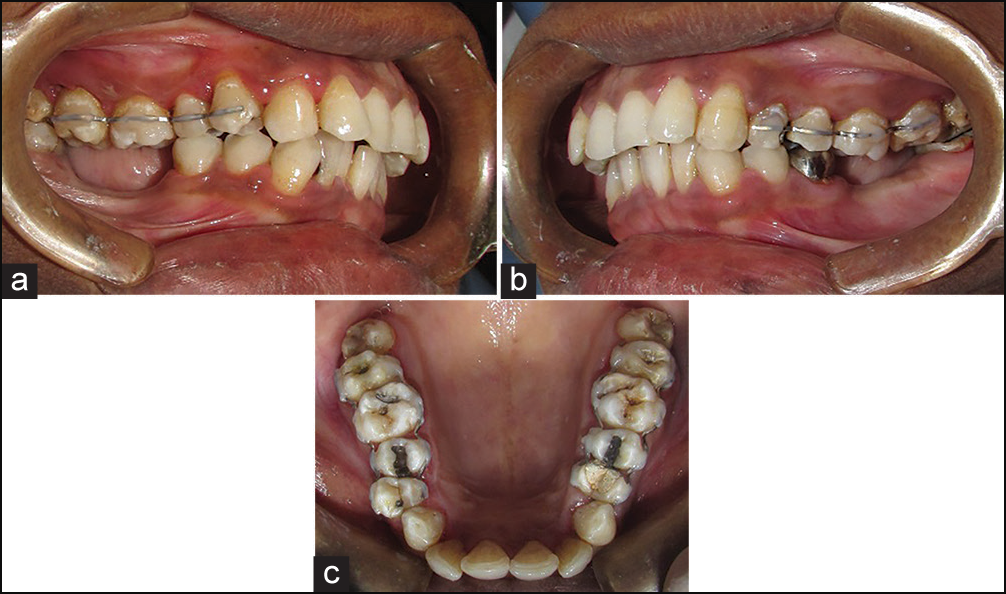
A 37-year-old woman was seeking restoration of her right and left posterior occlusion. She presented with a full complement of teeth except for the mandibular right and left first and second molars that were extracted 3 years ago because of decay. As a result, the maxillary right and left first and second molars were overerupted and there was insufficient occlusal clearance [Figures 1 and 2]. Judging by the marginal ridge discrepancy, the maxillary first molar had overerupted 3-3.5 mm occlusally, encroaching upon the antagonistic missing dental space. The objective of the treatment was to intrude the overerupted molar utilizing NTRDC intrusion arch and subsequently regain the appropriate dental space for prosthesis.
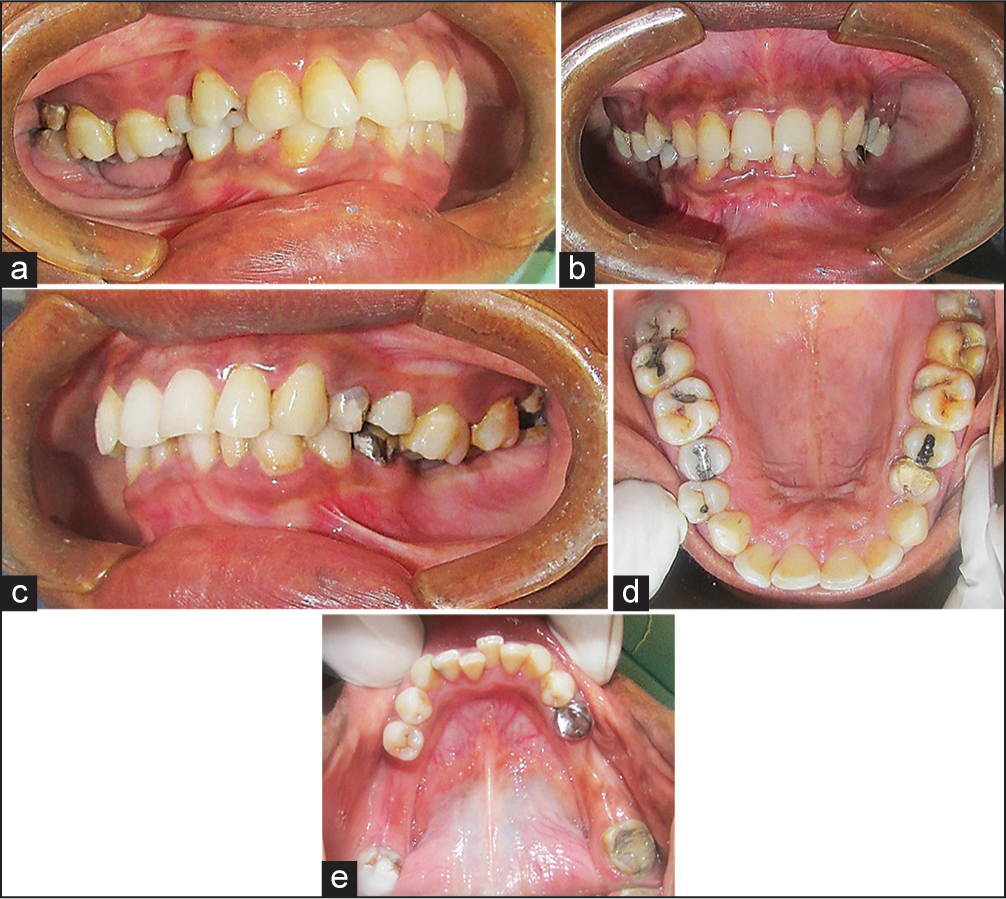
- Pretreatment intraoral photographs. (a) Right buccal view. (b) Frontal view. (c) Left buccal view. (d) Upper occlusal view. (e) Lower occlusal view
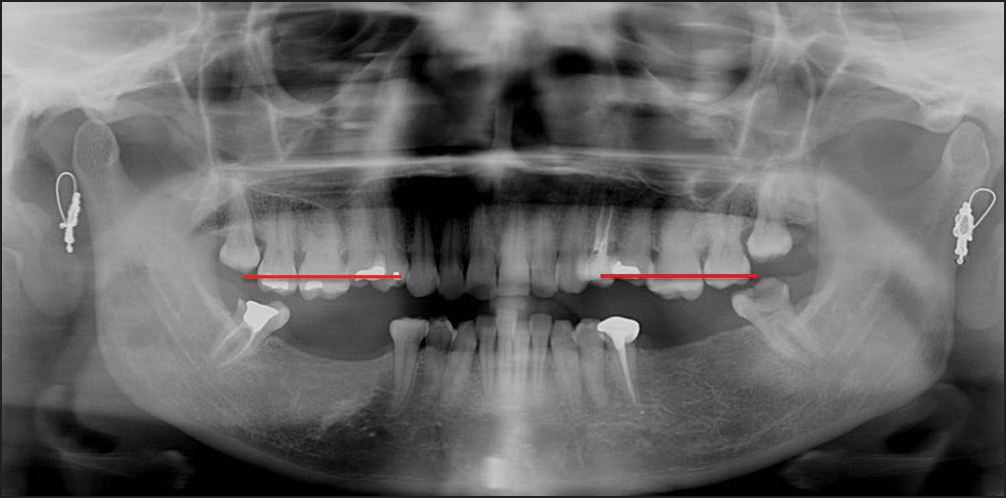
- Pretreatment panoramic radiograph
Treatment objectives
Intrude maxillary right and left first and second molars.
Treatment plan
Intrusion of upper right and left first and second molars with NTRDC double intrusion arch.
Prosthetic replacement of missing lower molars on both sides.
Appliance construction and treatment outcome
A pair of the framework was fabricated on working model with 21 × 25 inch stainless steel wire, which was adapted along the contours of canine, premolars, and third molar buccally and continuing it palatally. This was done to reinforce the anchorage. Helices were incorporated in the framework high in the vestibule in line with first molar and second molar for the engagement of elastics [Figure 3].
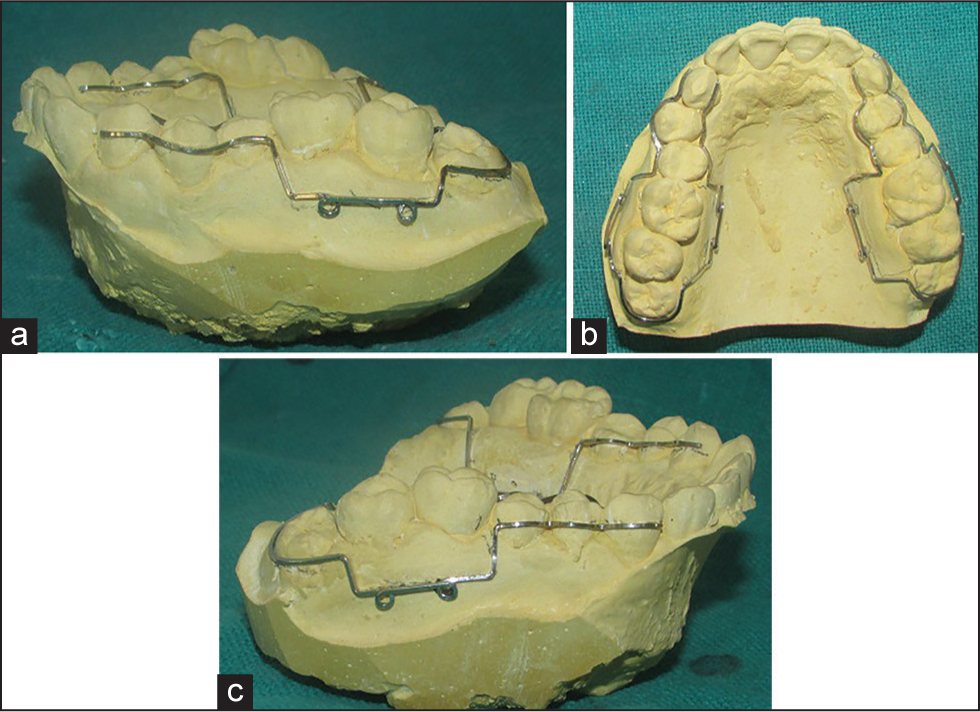 Figure 3
Figure 3- Wire framework. (a) Right side, (b) Palatal side, (c) Left side
The prestretched elastic was engaged into the helices for applying light force [Figure 4].
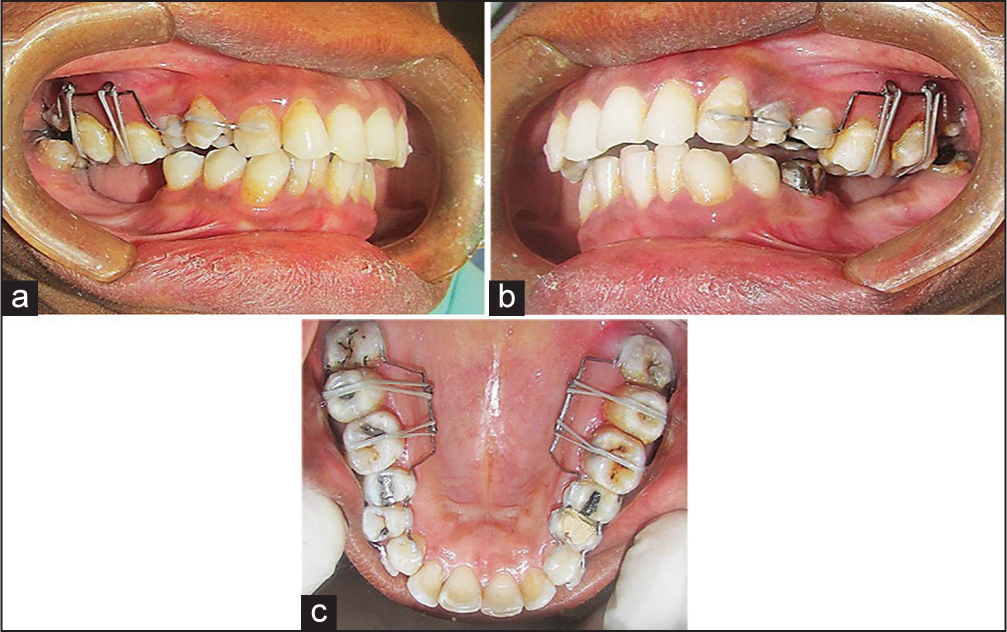 Figure 4
Figure 4- Nandlal Toshniwal Rural Dental College double intrusion arch with elastic in place (a) Right buccal view, (b) Left buccal view, (c) Upper occlusal view
Expected intrusion of molar was achieved in the time frame of 2 and 1/2 months [Figures 5 and 6].

Posttreatment intraoral photographs. (a) Right buccal view. (b) Frontal view. (c) Left buccal view. (d) Upper occlusal view. (e) Lower occlusal view
Posttreatment panoramic radiograph
For retention purpose, at least till the prosthesis was delivered, a 19 × 25 inch stainless steel wire was adapted and bonded on the buccal surface of premolars and molars [Figure 7].
Retainers in place (a) Right buccal view, (b) Frontal view, (c) Left buccal view
DISCUSSION
The case exemplified an effective mechanism using a NTRDC double intrusion arch to intrude overerupted tooth in patients who seek restorative care. With the advent of double intrusion arch, the need for possible crown reduction as preprosthodontic modality can be eliminated. Furthermore, the current strategy largely avoided the placement of full strap up fixed orthodontic appliances. The set up did drastically reduce the financial burden on the patient as well. The orthodontic clinician may adopt this conservative and cost-effective strategy in their routine practice. Molar intrusion is a challenging task, and it is more so in adult patients with restorative concerns. Loss of the mandibular first molar often results in overeruption of the opposing teeth; resulting in occlusal interference, functional disturbances, compromised periodontal health, and increased complexity of restoring the edentulous space.[2] Use of miniscrew implant in preprosthodontic management has drawn great interest in recent years among researchers and clinicians. However in this case, we could not use mini-implants because of less space between roots of premolars, and we don’t want patient to suffer an additional trauma of implant placement, so we designed the NTRDC double intrusion arch for this patient.
The intrusion of supererupted maxillary molars has been described by numerous authors, employing various treatment modalities with a wide range of movement rates and treatment times. Methods of correcting this problem generally involve either grinding the elongated tooth in preparation for a full-crown restoration or intruding the molar with an intermaxillary device,[6] sectional mechanics,[7] a removable appliance, a transpalatal bar,[8]anchorage from mini-plates[2] or mini-screws,[3]or magnets.[9] The present case was described as unique as there was very less interdental bone between premolars and molars limiting the use of modern methods like mini-implants for the molar intrusion. So, we designed NTRDC double intrusion arch. The elastics were used as it exerts the optimal amount of force required for intrusion (this kind of tooth movement requires light force).
In this report, we have demonstrated a simplified version of replacing mini-screws with NTRDC double intrusion arch to intrude the maxillary first and second molars simultaneously on both sides. Most importantly, the molar responded well to the intrusive forces throughout treatment, no root resorption was detected during follow-up, and the vitality of the teeth was sustained after 6 months follow-up. The orthodontic clinician may adopt this conservative and cost-effective strategy in their routine practice. The coordination of different specialties allowed us to gain optimal results in a shorter treatment time.
CONCLUSION
The present article serves as a viable alternative to carryout molar intrusion in such patient where today’s modern methods cannot be used, thus emphasizing the role of these appliances in orthodontics. The favorable result obtained shows that the intrusion procedure is an acceptable treatment option for extruded molars that can be preferred instead of prosthodontics reduction or the extraction of the extruded tooth.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Intrusion of supra-erupted molars using miniscrews: Clinical success and root resorption. Am J Orthod Dentofacial Orthop. 2011;139:S170-5.
- [Google Scholar]
- Intrusion of the overerupted upper left first and second molars by mini-implants with partial-fixed orthodontic appliances: A case report. Angle Orthod. 2004;74:550-7.
- [Google Scholar]
- Intrusion of overerupted maxillary molars with miniscrew anchorage. J Clin Orthod. 2006;40:378-83.
- [Google Scholar]
- Anatomical guidelines for miniscrew insertion: Vestibular interradicular sites. J Clin Orthod. 2011;45:165-73.
- [Google Scholar]
- Evaluation of interdental space of the maxillary posterior area for orthodontic mini-implants with cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2009;135:635-41.
- [Google Scholar]
- The uprighting of tilted molar teeth and the intrusion of over-erupted posterior teeth. Aust Orthod J. 1986;9:329-34.
- [Google Scholar]




