

Translate this page into:
The clinical diversity of segmental orthodontics in pre-prosthetic cases

*Corresponding author: Roxana Rugina, Department of Orthodontics, Clinica Rugina, Str. Gheorghe Doja 23, Timisoara, Romania. rox.rugina@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Rugina R, Lazar D. The clinical diversity of segmental orthodontics in pre-prosthetic cases. APOS Trends Orthod 2020;10(3):191-4.
Abstract
The prosthodontic rehabilitation of edentulous spaces is a very common demand of patients. However, in the majority of cases, this is not as simple as it sounds. Because in time, the consequences of tooth extraction affect the neighboring teeth, leading to tooth migrations, tooth rotations, tilting, and the sagittal and vertical reduction of the edentulous spaces that have to be restored. Using segmental orthodontics on a limited number of teeth associated with skeletal anchorage, we can significantly improve the clinical situation, correcting these consequences of tooth migration following extraction, allowing the prosthodontist to have a better starting point in the process of rehabilitation. The treatment time is shorter than compared to a comprehensive orthodontic treatment, and thus, the patient acceptance may be increased. Once the spaces are correctly calibrated, and the tooth migrations have been corrected, the prosthodontist can restore the missing teeth as minimally invasive as possible.
Keywords
Skeletal anchorage
Mini-implants
Direct and indirect anchorage
Pre-prosthetic orthodontics
Segmental orthodontics

INTRODUCTION
Restoring edentulous spaces can pose quite a challenge for the prosthodontist due to all the tooth movements of the neighboring teeth that occur in time, such as tilting, extrusion, rotation, and/ or reduction of the edentulous space. The orthodontic correction of these migrations facilitates the prosthodontic rehabilitation, reducing, if not eliminating, the need for healthy tissue sacrifice; it improves the axial loading of the teeth and facilitates the maintaining of a healthy periodontal environment. Segmental orthodontics offers an alternative treatment in correcting these tooth migrations using a limited number of teeth and skeletal anchorage.[1] This approach uses direct and indirect anchorage from mini-implants, therefore eliminating the need to involve a large number of anchor teeth and, at the same time, controlling the secondary effects on the active units.[2-4]
Because the orthodontic movements in these cases are made to improve the prosthodontic situation, clear treatment objectives have to be set by the interdisciplinary team orthodontist- prosthodontist.
This way, the orthodontist can calibrate these spaces and reposition the migrated teeth improving, thereby the pre-prosthetic clinical situation and allowing the prosthodontist to be less invasive with the healthy dental tissue of the patient.
Segmental orthodontics can be used in several ways, its clinical applications being very diverse, according to the clinical situation and the biological limits. However, the biomechanical principles remain the same, to obtain the desired dental tooth movements, an anchor unit, an active unit, and the activation protocol are needed to create the appliance design.
As specified before, clear objectives have to be established by the interdisciplinary team prosthodontist-orthodontist, such as the intrusion or uprighting of a molar, a derotation of a rotated tooth, or space calibration to restore an edentulous space.
In this report, two cases are used to exemplify the clinical diversity of segmental orthodontics.
Technique
The appliance design consists of three parts: The anchor unit, the active unit, and the activation protocol. The anchor unit consists usually of two neighboring teeth and one or two mini-implants, connected by a 19 × 25 stainless steel wire. The wire is bent around the mini-implant, it extends from the mini-implant to the anchor teeth, and it is attached on both ends with flowable composite. The entire construction is built to be passive so that it does not exert any tension on the anchor teeth nor any pressure on the gingival tissue.
The active unit consists of a limited number of teeth that need to be moved according to the treatment objectives set by the interdisciplinary team.
The activation protocol consists of the wire sequence and the accessories, such as elastic chains or coil springs, needed for the specific dental movement.
Clinical case 1
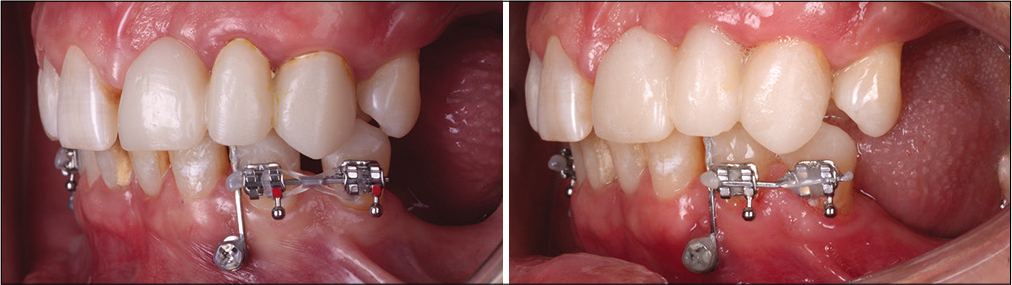
This patient, 52 years old, presented herself to the prosthodontist with the wish to restore her edentulous spaces. Implants were planned to restore the missing spaces in all the four quadrants. However, because the extractions were made several years ago, the neighboring teeth migrated and invaded the edentulous spaces making the rehabilitation process very difficult [Figure 1]. The patient did not wish to have brackets bonded on all the teeth, and she refused a comprehensive orthodontic treatment. An alternative treatment approach with segmental orthodontics and skeletal anchorage was proposed to her by the interdisciplinary team. To improve the clinical situation for the prosthodontic rehabilitation, a segmental appliance was planned in the first quadrant, with indirect anchorage on a mini-implant to stabilize the upper right first molar and a direct anchorage from a second mini- implant so that a force couple could be used with an elastic chain to derotate the upper right second premolar. After the derotation, a bracket was placed on the premolar and with the use of a 19 × 25 NiTi wire followed by a 19 × 25 SS wire, the long axis of the tooth was corrected to be properly placed in the bone. For the insertion of the implant at the position of the upper right first premolar, the mini-implant in the edentulous space had to be removed, and another mini-implant was inserted distal to the molar just to maintain the orthodontic outcome until the prosthodontic rehabilitation [Figure 2].

- Clinical case 1: Initial situation.
- Clinical case 1: Treatment sequence in the first quadrant.
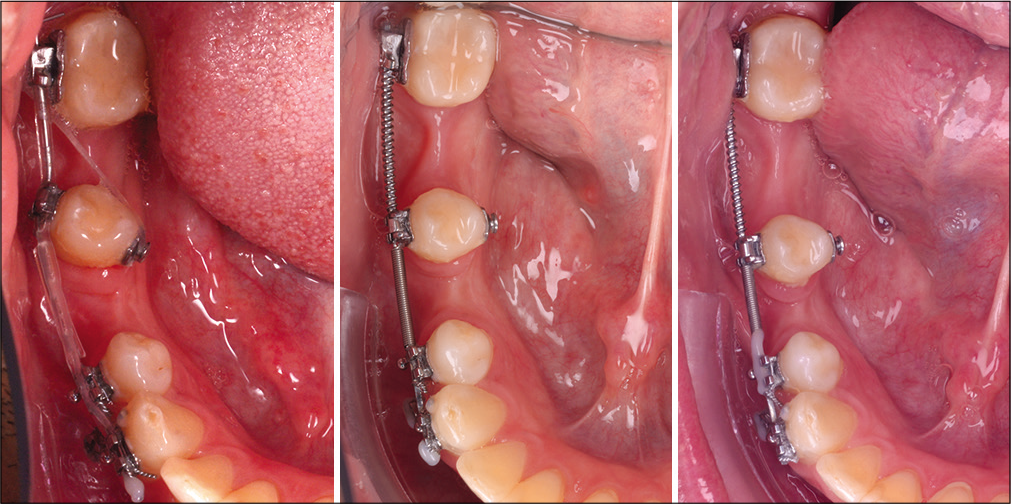
In the third quadrant, the overerupted second premolar had to be intruded. Therefore, brackets were bonded on both premolars, the first premolar was stabilized with indirect anchorage from a mini-implant inserted between the two premolars. The second premolar was intruded with the use of a 19 × 25 SS wire with a progressive intrusion step [Figure 3].

- Clinical case 1: Treatment sequence in the third quadrant.
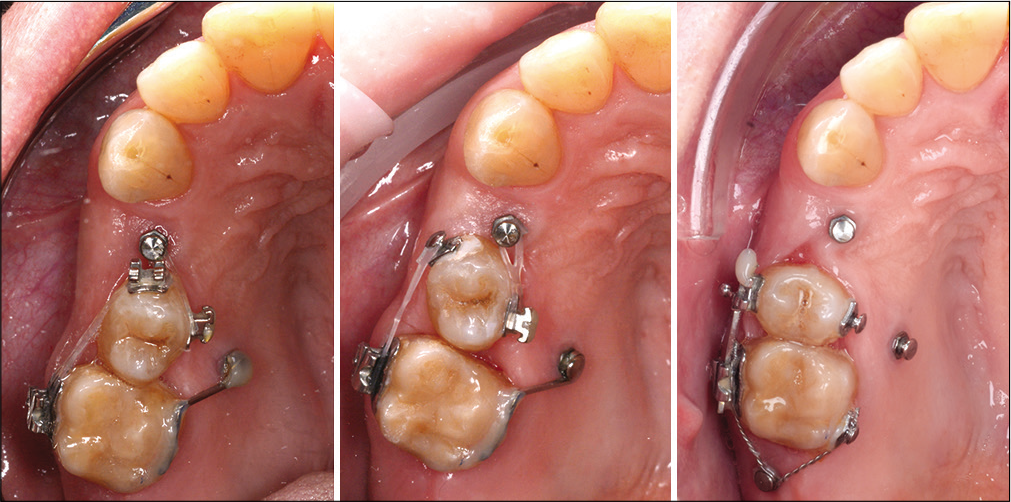
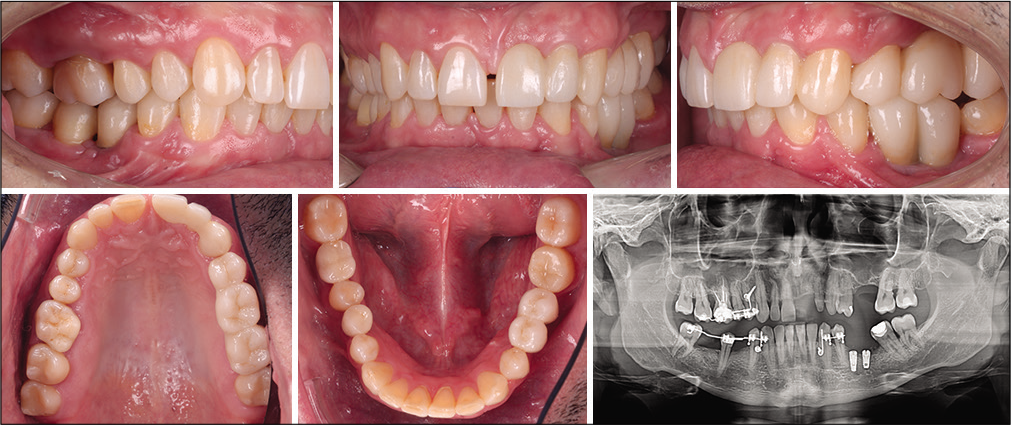
In the fourth quadrant, the edentulous space needed to be reopened, and the second molar distalized, uprighted, and intruded. The two premolars were anchored to a mini-implant inserted between the roots. The uprighting of the molar was accomplished with the help of an active open coil and sequential wires, 0.18 NiTi, 19 × 25 NiTi, and 19 × 25 SS. The open coil was first placed on 19 × 25 NiTi, slightly active to distally derotate the molar, and it was on 19 × 25 SS that the open coil was actively used for the distalization of the molar. An intrusion step was added on the stainless steel wire to intrude the molar while uprighting it so that it would not create an occlusal interference [Figure 4]. Once sufficient space was obtained for an implant, the activation process was stopped, and the appliance remained passive until the prosthodontic rehabilitation could be finalized. The total active treatment time was 10 months. The mini- implants used for this case (Osstem Orthodontic Screw) measured 1.6 mm in diameter and 8 mm in length, except for the distal mini-implant in the first quadrant which measured 1.6 mm in diameter and 10 mm in length [Figure 5].

- Clinical case 1: Treatment sequence in the fourth quadrant.
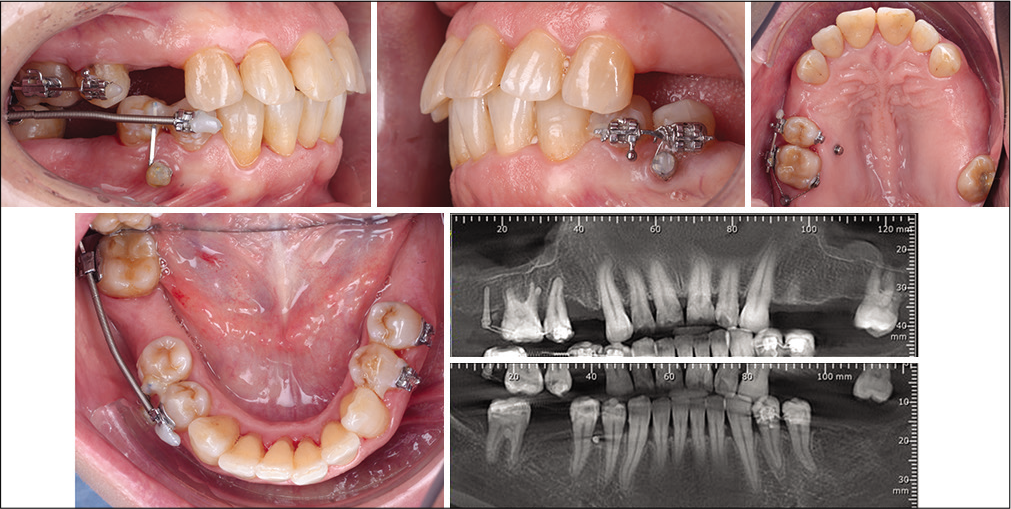
- Clinical case 1: Final situation.
Clinical case 2
The second patient, 40 years old, came in for periodontal treatment and the rehabilitation of the edentulous spaces. The clinical situation was complex due to the tooth migrations that had occurred after the extraction of the missing teeth: A space had opened up between the lower left first premolar and the canine, the lower right second premolar had distally drifted into the edentulous space and was distally rotated, the third molar was mesially rotated, and the upper right first molar was overerupted and in crossbite with the rotated lower premolar [Figure 6]. However, the patient did not want to have braces on all the teeth so an alternative treatment plan with segmental orthodontics and mini-implants was proposed, and the patient accepted.
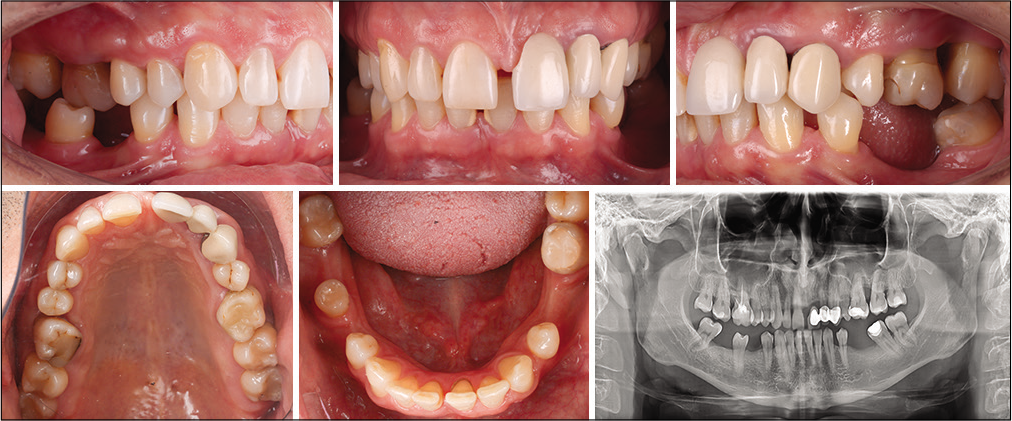
- Clinical case 2: Initial situation.
For the corrections in the first quadrant, the premolars were anchored to a mini-implant inserted between the first premolar and the canine. Once the first molar was in the correct position, the second molar was also bonded to intrude it and to correct the positive buccal crown torque. The corrections were accomplished with the wire sequence 0.16 NiTi, 17 × 25 NiTi, 19 × 25 NiTi, and 19 × 25 SS. On the stainless steel wire, an offset was bent to improve the position of the upper first molar. To intrude the second molar and to correct the buccal crown torque, an intrusion step and a third-order bend were added on the wire [Figure 7].
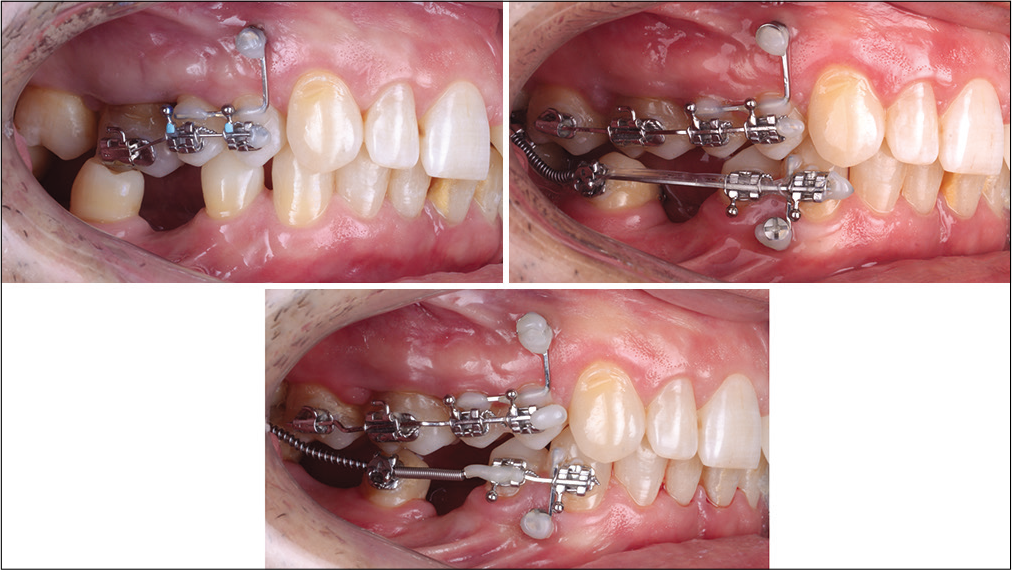
- Clinical case 2: Treatment sequence in the first quadrant.
In the third quadrant, the first premolar was mesialized to close the space between the premolar and the canine. The canine was anchored to a mini-implant inserted between the canine and the premolar [Figure 8].
- Clinical case 2: Treatment sequence in the third quadrant.
In the fourth quadrant, the treatment objective was to derotate the second premolar and to calibrate the two spaces for implants mesial and distal to the second premolar. The canine and the premolars were used together with the mini-implant inserted between their roots as the anchor unit. The rotations were corrected, the axial tooth inclinations were improved, and the spaces were accordingly calibrated [Figure 9].
- Clinical case 2: Treatment sequence in the fourth quadrant.
All the treatment objectives were obtained using the segmental approach with the same biomechanical principles. All the mini-implants (Dual Top Anchor System, Jeil Medical Corporation) used in this case measured 1.6 mm in diameter and 8 mm in length. The active treatment time for the first and the fourth quadrant was 10 months, while the corrections in the third quadrant took 3 months. Once the spaces were correctly calibrated that the implants were inserted, and the appliance remained passive until the prosthodontic rehabilitation could be finished [Figure 10].
- Clinical case 2: Final situation.
CONCLUSION
These clinical cases demonstrate the effectiveness and the clinical diversity of segmental orthodontics with skeletal anchorage in cases needing pre-prosthetic orthodontics, specifically those related to the rehabilitation of edentulous spaces, in which the migration of the neighboring teeth occurred. With the use of mini-implants and direct and indirect anchorage, these corrections can be accomplished with segmental orthodontics involving only a few teeth. This way, the desired tooth movements can be obtained without requiring a large number of anchor teeth and without undesirable secondary effect on the active units. The clinical pre-prosthetic situations can be improved by correctly calibrating the edentulous spaces and by properly placing the adjacent teeth into the bone, therefore improving their axial load during occlusal forces and creating a better periodontal environment. The patient acceptance toward orthodontic correction using this approach may be increased due to the limited number of bonded teeth involved.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Segmental orthodontics for space calibration in preprosthodontic treatment. J Clin Orthod. 2019;53:227-33.
- [Google Scholar]
- Mini-Implants in Orthodontic: Innovative Anchorage Concepts United States: Quintessence Publishing; 2008.
- [Google Scholar]
- Uprighting second molars with micro-implant anchorage. J Clin Orthod. 2004;38:100-3.
- [Google Scholar]
- Uprighting mesially impacted second molars with miniscrew anchorage. J Clin Orthod. 2007;41:94-7.
- [Google Scholar]




