

Translate this page into:
The effect of the presence of brackets on the reliability of measurements made on three-dimensional digital models

*Corresponding author: Nurver Karsli, Department of Orthodontics, Faculty of Dentistry, Karadeniz Technical University, Trabzon, Turkey. dtnurverkarsli@hotmail.com
-
Received: ,
Accepted: ,
How to cite this article: Tuhan Kutlu E, Karsli N. The effect of the presence of brackets on the reliability of measurements made on three-dimensional digital models. APOS Trends Orthod. 2025;15:70-7. doi: 10.25259/APOS_204_2023
Abstract
Objectives:
Digital model scans are frequently used today at the beginning and intermediate stages of orthodontic treatment. The aim of this study is to evaluate the effect of orthodontic brackets on linear measurements made on three-dimensional digital models.
Material and Methods:
Dental models were obtained from 40 patients before orthodontic treatment and in the first treatment session. Dental plaster models were converted into digital models using the 3Shape R700 (3Shape, Copenhagen, Denmark) model scanner. Intraoral scans were created with the Shape Trios3 (3Shape, Copenhagen, Denmark) intraoral scanner. Digital models were transferred to the Orthoanalyzer program (3Shape, Copenhagen, Denmark), and linear measurements were made.
Results:
There was no significant difference in the measurements made in intraoral scans scanned with and without brackets. No significant difference was observed in the measurements made on model scans with and without brackets (P > 0.05).
Conclusion:
Digital scanner systems, which are increasingly used with developing technology, provide safe and effective results even in the presence of brackets.
Keywords
Digital dental model
Orthodontic brackets
Dental measurements

INTRODUCTION
Dental models, intraoral and extraoral photographs, and clinical and radiological examination methods are used for the diagnosis and treatment planning of malocclusion in orthodontics.[1,2] In the examination of malocclusion, orthodontic plaster models have been the gold standard from the past to the present.[3] Abrasions that occur as a result of measurements made on plaster models, the resulting decrease in measurement reliability, the risk of breakage, and the need for a physical space for storage can be counted as disadvantages.[4]
With developments in computer technology, digital models are now widely used for orthodontic diagnosis and treatment planning.[5] These models can be created using indirect or direct techniques. Indirect methods include laser scanning of plaster models obtained with alginate impressions, while direct methods include intraoral scanning of patients.[6,7] These digital scanning models have many advantages over plaster models, such as the absence of storage problems and the risk of model breakage.[8] In addition, digital models facilitate the exchange of ideas with patients and other physicians.[9,10]
Successful orthodontic treatment depends not only on the diagnosis but also on the correct evaluation of the treatment process. Clinicians often take digital or conventional models from patients to analyze occlusion and evaluate tooth movement during the ongoing stages of orthodontic treatment.[11]
With recent developments in intraoral scanners, digital intraoral scanning has been widely used at the beginning of treatment as an alternative to traditional impressions in dentistry, and its reliability has been reported in previous studies.[12-14] In contrast, digital scans in the ongoing stages of orthodontic treatment are performed in the presence of orthodontic brackets on the teeth. Few studies have investigated the effect of orthodontic brackets on digital scans.[11]
In the literature, studies on the effect of brackets on the reliability of linear measurements made on three-dimensional (3D) digital models are limited. In light of this information and these studies, we aim to evaluate the effect of orthodontic brackets on linear measurements made using 3D digital models. This study aims to provide a careful and conscious approach to the patient by observing whether the digital model recordings taken in the intermediate stages of orthodontic treatment make a difference compared to the initial recordings.
MATERIAL AND METHODS
This study was approved by the Ethics Committee of the Karadeniz Technical University Faculty of Dentistry (2022/4.07/09/2022). The individuals included in the study were selected from among the patients who applied to our clinic for orthodontic treatment, and informed consent was obtained. Before the study, the required number of patients was determined as 40 by taking alpha error = 0.05, beta error = 0.20, effect size 0.5, and power analysis in order for the results to reveal statistically significant data.[10]
The patients included in the study were those who did not have orthodontic treatment history, did not have any periodontal problems, had permanent dentition, and did not lack permanent teeth from the first molar to the opposite arch of the first molar. Patients with extensive restoration of their teeth, presence of hypodontia and supernumerary teeth, congenital anomalies, and syndromes were excluded from the study.
Roth system stainless steel upper and lower brackets and molar tubes (Mini Master Series, American Orthodontics, USA) with a 0.022” slot were used for orthodontic treatment of the patients. Dental impressions were taken with Zhermack Hydrocolor 5 (Zhermack SpA, Badia Polesine, Italy) alginate material from the patients without brackets before orthodontic treatment and at the beginning of orthodontic treatment with brackets. Dental models were obtained using Zhermack Elite Rock Type IV (Zhermack SpA, Badia Polesine, Italy) dental plaster without waiting for the measurements to be taken. Bracketless and bracketed dental plaster models were converted to digital models using the 3Shape R700 (3Shape, Copenhagen, Denmark) model scanner [Figure 1 and 2].
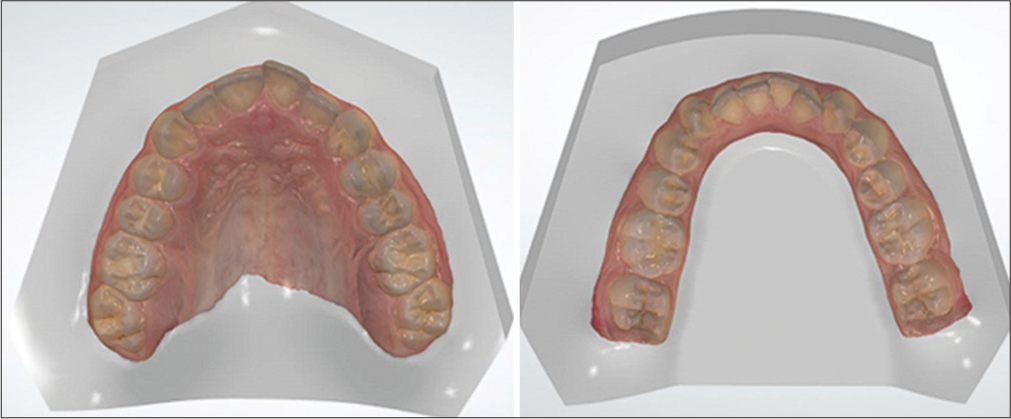
- Bracketless intraoral scan images.
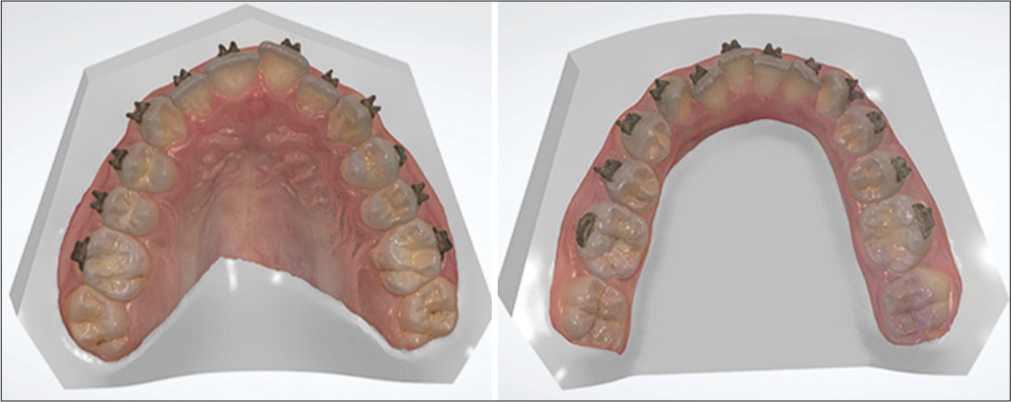
- Bracketed intraoral scan images.
Intraoral models of the patients were created with the 3Shape Trios3 (3Shape, Copenhagen, Denmark) intraoral scanner before orthodontic treatment started and when orthodontic treatment started [Figure 3 and 4]. Digital models were transferred to the Orthoanalyzer program (3Shape, Copenhagen, Denmark), and measurements were made through this program.
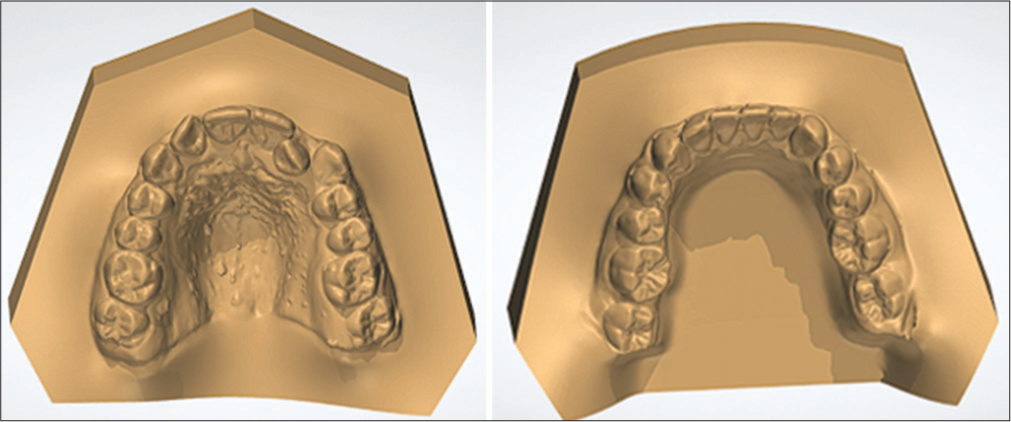
- Bracketless model scan images.
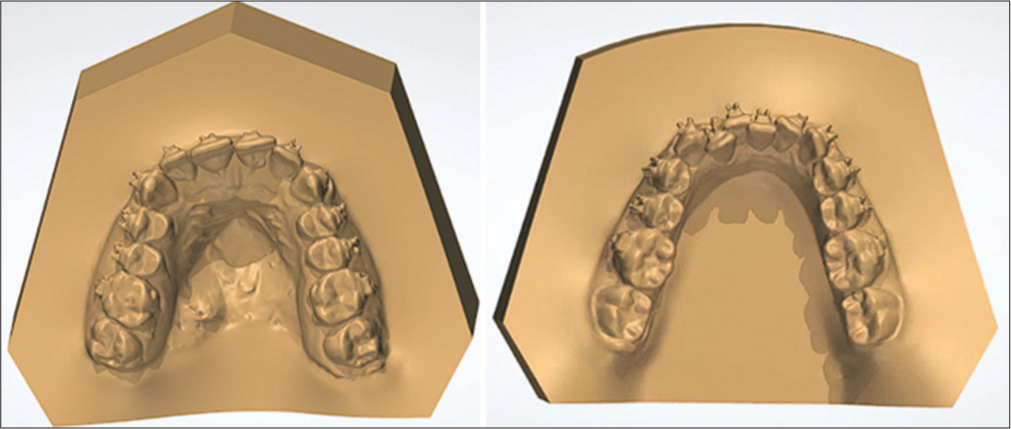
- Bracketed model scan images.
Care was taken to ensure that the plaster models were physically strong and clear and that there was no problem with the image and quality of the digital models. To evaluate the reliability of the measurements, all measurements were repeated by the same researcher with an interval of 30 days.
The measurements evaluated on the digital models are as follows:
Arch circumference: This is the sum of the individual mesiodistal dimensions of all teeth from the distal of the right first molar to the distal of the left first molar.
Arch length: This is the sum of the distance from the mesial contact points of the santal incisors to the distal of the canines and the distance from the distal of the canines to the mesial of the first molars.
Intermolar distance: This is the distance between the mesiobuccal tubercle crests of the right and left first molars.
Intercanine distance: This is the distance between the cusp crests of the right and left canine teeth.
Interpremolar distance: This is the distance between the mesiobuccal contact points of the right and left first and second premolars.
Statistical analysis
The Statistical Package for the Social Sciences 26 program was used for the statistical analysis. Descriptive statistical methods (mean, standard deviation, median, frequency, percentage, minimum, and maximum) were used to evaluate the study data. The conformity of the quantitative data to the normal distribution was tested with the Kolmogorov–Smirnov test, Shapiro–Wilk test, and graphical examinations. A dependent group t-test was used to compare normally distributed quantitative variables. The Wilcoxon signed-ranks test was used to compare quantitative variables that did not show a normal distribution. To evaluate intraobserver reliability, cephalometric radiographs were re-evaluated 30 days after the first assessment. Statistical significance was accepted as P < 0.05.
RESULTS
This study was conducted with a total of 40 cases. The intraclass correlation coefficients for the linear measurements of the digital models were >0.962, confirming the reliability of the measurement. [Table 1] shows the mean values of the measurements made on the bracketed and non-bracketed models with intraoral scanning. No statistically significant difference was found between the upper and lower arch circumferences, upper and lower arch lengths, upper and lower intercanine measurements, upper and lower interpremolar measurements, upper and lower intermolar measurements of the cases with and without braces, and intraoral scanning with brackets (P > 0.05).
| Group | Mean | SD | Median (Min–Max) | P |
|---|---|---|---|---|
| Upper arch circumference | ||||
| Bracketless | 86.99 | 4.29 | 87.7 (79.2–96.2) | a0.373 |
| Bracketed | 87.3 | 3.99 | 86.7 (79.3–95.1) | |
| Lower arch circumference | ||||
| Bracketless | 80.66 | 3.91 | 81.6 (71.8–87.9) | a0.564 |
| Bracketed | 80.42 | 4.47 | 80.7 (70.7–89.6) | |
| Upper arch length | ||||
| Bracketless | 93.34 | 4.99 | 93.8 (83.1–103.4) | a0.823 |
| Bracketed | 93.4 | 5.17 | 93.6 (82.5–105.5) | |
| Lower arch length | ||||
| Bracketless | 84.48 | 4.99 | 84.9 (74.3–96.8) | a0.544 |
| Bracketed | 84.29 | 4.52 | 84.2 (75–94.8) | |
| Upper intercanine | ||||
| Bracketless | 34.12 | 2.72 | 34.7 (25.2–38.3) | a0.614 |
| Bracketed | 34.27 | 2.35 | 34.5 (29.3–37.4) | |
| Lower intercanine | ||||
| Bracketless | 26.79 | 2.43 | 26.4 (22.5–34.6) | a0.845 |
| Bracketed | 26.85 | 2.9 | 26.6 (22.7–37.1) | |
| Upper interpremolar | ||||
| Bracketless | 42.48 | 2.74 | 42.6 (36.2–48.2) | a0.243 |
| Bracketed | 42.78 | 2.78 | 42.5 (36.2–48.4) | |
| Lower interpremolar | ||||
| Bracketless | 36.32 | 3.08 | 36.6 (29.9–42.3) | a0.641 |
| Bracketed | 36.13 | 3.68 | 35.8 (26.4–46.5) | |
| Upper intermolar | ||||
| Bracketless | 51.5 | 3.45 | 51.7 (44.6–60.5) | a0.045 |
| Bracketed | 51.73 | 3.36 | 51.9 (44.6–60.8) | |
| Lower intermolar | ||||
| Bracketless | 45.13 | 3.45 | 45.3 (37.2–53.6) | a0.230 |
| Bracketed | 44.64 | 3.98 | 44.5 (37.5–55) |
aPaired samples test. SD: Standard deviation
[Table 2] shows the mean values of the measurements on the bracketed and non-bracketed models for which the model was scanned. No statistically significant difference was found between the upper and lower arch circumferences, upper and lower arch lengths, upper and lower intercanine measurements, upper and lower interpremolar measurements, and upper and lower intermolar measurements of the cases with and without bracket scanning (P > 0.05).
| Group | Mean | SD | Median (Min–Max) | P |
|---|---|---|---|---|
| Upper arch circumference | ||||
| Bracketless | 85.59 | 4.28 | 86.3 (76.3–92.3) | a0.329 |
| Bracketed | 85.26 | 3.98 | 84.9 (76.9–93.2) | |
| Lower arch circumference | ||||
| Bracketless | 79.88 | 3.77 | 80.5 (72.8–87.8) | a0.608 |
| Bracketed | 80.04 | 3.91 | 80.1 (70.4–89.3) | |
| Upper arch length | ||||
| Bracketless | 92.94 | 5.73 | 93.1 (80–106) | a0.834 |
| Bracketed | 92.83 | 5.4 | 93.5 (82.9–106) | |
| Lower arch length | ||||
| Bracketless | 84.13 | 4.44 | 84.2 (75.7–95.5) | a0.081 |
| Bracketed | 84.47 | 4.76 | 84 (75.4–97.3) | |
| Upper intercanine | ||||
| Bracketless | 34.08 | 2.3 | 34.4 (29.1–37.8) | a0.979 |
| Bracketed | 34.09 | 2.31 | 34.4 (28.8–37.1) | |
| Lower intercanine | ||||
| Bracketless | 26.67 | 2.02 | 26.6 (22.8–30.3) | b0.260 |
| Bracketed | 27.26 | 3.74 | 26.9 (22.9–46.8) | |
| Upper interpremolar | ||||
| Bracketless | 42.52 | 2.78 | 42.6 (35.9–47.4) | a0.180 |
| Bracketed | 42.82 | 3.24 | 42.9 (36.5–54.3) | |
| Lower interpremolar | ||||
| Bracketless | 36.4 | 2.81 | 36.3 (29.5–42.1) | a0.301 |
| Bracketed | 36.08 | 2.86 | 36.1 (28.6–41.4) | |
| Upper intermolar | ||||
| Bracketless | 51.58 | 3.56 | 51.2 (44.8–61.1) | a0.503 |
| Bracketed | 51.26 | 3.63 | 51.5 (40.7–60.1) | |
| Lower intermolar | ||||
| Bracketless | 45.18 | 3.41 | 45.7 (37.7–53.3) | a0.489 |
| Bracketed | 45.09 | 3.38 | 45.8 (36.9–54.2) |
aPaired samples test, bWilcoxon signed-ranks test. SD: Standard deviation
[Table 3] shows the mean values of the measurements made on the intraoral and model scans of the bracketless models. Upper arch circumference values of the patients who underwent intraoral scanning without brackets were found to be significantly higher than those on whom non-bracket model scanning was performed (P = 0.001; P < 0.01). The lower arch circumference values of the patients who underwent intraoral scanning without brackets were found to be significantly higher than those who underwent model scanning without brackets (P = 0.022; P < 0.05). No statistically significant difference was found between the upper and lower intercanine measurements, upper and lower interpremolar measurements, and upper and lower intermolar measurements of the cases who underwent bracketless intraoral and non-bracket model scanning (P > 0.05).
| Group | Mean | SD | Median (Min–Max) | P |
|---|---|---|---|---|
| Upper arch circumference | ||||
| Intraoral scanning | 86.99 | 4.29 | 87.7 (79.2–96.2) | a0.001** |
| Model scanning | 85.59 | 4.28 | 86.3 (76.3–92.3) | |
| Lower arch circumference | ||||
| Intraoral scanning | 80.66 | 3.91 | 81.6 (71.8–87.9) | a0.022* |
| Model scanning | 79.88 | 3.77 | 80.5 (72.8–87.8) | |
| Upper arch length | ||||
| Intraoral scanning | 93.34 | 4.99 | 93.8 (83.1–103.4) | a0.362 |
| Model scanning | 92.94 | 5.73 | 93.1 (80–106) | |
| Lower arch length | ||||
| Intraoral scanning | 84.48 | 4.99 | 84.9 (74.3–96.8) | a0.128 |
| Model scanning | 84.13 | 4.44 | 84.2 (75.7–95.5) | |
| Upper intercanine | ||||
| Intraoral scanning | 34.12 | 2.72 | 34.7 (25.2–38.3) | a0.885 |
| Model scanning | 34.08 | 2.3 | 34.4 (29.1–37.8) | |
| Lower intercanine | ||||
| Intraoral scanning | 26.79 | 2.43 | 26.4 (22.5–34.6) | a0.613 |
| Model scanning | 26.67 | 2.02 | 26.6 (22.8–30.3) | |
| Upper interpremolar | ||||
| Intraoral scanning | 42.48 | 2.74 | 42.6 (36.2–48.2) | a0.882 |
| Model scanning | 42.52 | 2.78 | 42.6 (35.9–47.4) | |
| Lower interpremolar | ||||
| Intraoral scanning | 36.32 | 3.08 | 36.6 (29.9–42.3) | a0.692 |
| Model scanning | 36.4 | 2.81 | 36.3 (29.5–42.1) | |
| Upper intermolar | ||||
| Intraoral scanning | 51.5 | 3.45 | 51.7 (44.6–60.5) | a0.834 |
| Model scanning | 51.58 | 3.56 | 51.2 (44.8–61.1) | |
| Lower intermolar | ||||
| Intraoral scanning | 45.13 | 3.45 | 45.3 (37.2–53.6) | a0.836 |
| Model scanning | 45.18 | 3.41 | 45.7 (37.7–53.3) |
aPaired samples test, Bold value signifies *P<0.05, Bold value signifies **P<0.01. SD: Standard deviation
[Table 4] shows the mean values of the measurements made on the intraoral and model scans of the bracketed models. Upper arch circumference values of the patients who underwent intraoral scans with bracket were found to be significantly higher than those who underwent bracket model scans (P = 0.001; P < 0.01). The lower intercanine values of the patients who underwent bracketed intraoral scanning were found to be significantly higher than those who underwent bracketed model scanning (P = 0.013; P < 0.05). No statistically significant differences were found between the upper arch circumference, upper intercanine measurement, upper and lower interpremolar measurements, and upper and lower intermolar measurements of cases with bracketed intraoral and bracketed model scanning (P > 0.05).
| Group | Mean | SD | Median (Min–Max) | p |
|---|---|---|---|---|
| Upper arch circumference | ||||
| Intraoral scanning | 87.3 | 3.99 | 86.7 (79.3–95.1) | a0.001** |
| Model scanning | 85.26 | 3.98 | 84.9 (76.9–93.2) | |
| Lower arch circumference | ||||
| Intraoral scanning | 80.42 | 4.47 | 80.7 (70.7–89.6) | a0.427 |
| Model scanning | 80.04 | 3.91 | 80.1 (70.4–89.3) | |
| Upper arch length | ||||
| Intraoral scanning | 93.4 | 5.17 | 93.6 (82.5–105.5) | a0.205 |
| Model scanning | 92.83 | 5.4 | 93.5 (82.9–106) | |
| Lower arch length | ||||
| Intraoral scanning | 84.29 | 4.52 | 84.2 (75–94.8) | a0.474 |
| Model scanning | 84.47 | 4.76 | 84 (75.4–97.3) | |
| Upper intercanine | ||||
| Intraoral scanning | 34.27 | 2.35 | 34.5 (29.3–37.4) | a0.528 |
| Model scanning | 34.09 | 2.31 | 34.4 (28.8–37.1) | |
| Lower intercanine | ||||
| Intraoral scanning | 26.85 | 2.9 | 26.6 (22.7–37.1) | b0.013* |
| Model scanning | 27.26 | 3.74 | 26.9 (22.9–46.8) | |
| Upper interpremolar | ||||
| Intraoral scanning | 42.78 | 2.78 | 42.5 (36.2–48.4) | a0.861 |
| Model scanning | 42.82 | 3.24 | 42.9 (36.5–54.3) | |
| Lower interpremolar | ||||
| Intraoral scanning | 36.13 | 3.68 | 35.8 (26.4–46.5) | a0.928 |
| Model scanning | 36.08 | 2.86 | 36.1 (28.6–41.4) | |
| Upper intermolar | ||||
| Intraoral scanning | 51.73 | 3.36 | 51.9 (44.6–60.8) | a0.271 |
| Model scanning | 51.26 | 3.63 | 51.5 (40.7–60.1) | |
| Lower intermolar | ||||
| Intraoral scanning | 44.64 | 3.98 | 44.5 (37.5–55) | a0.246 |
| Model scanning | 45.09 | 3.38 | 45.8 (36.9–54.2) |
aPaired samples test, bWilcoxon signed-ranks test, Bold value signifies *P<0.05, Bold value signifies **P<0.01. SD: Standard deviation
DISCUSSION
Orthodontic records are necessary for orthodontic diagnosis and treatment plans, and these records play an important role in patient documentation and in monitoring growth and development during orthodontic treatment.[15,16] Traditionally, dental plaster models, intraoral and extraoral photographs, radiographic images, and various analyses have been used for this purpose.
The development of low radiation dose cone-beam computed tomography and digital dental scanners has increased the clinical use of more specific data, making important contributions to orthodontic diagnosis and treatment planning.[17]
Dental models, whether plaster or digital, are not only taken at the beginning of orthodontic treatment but is also necessary in the intermediate stages of the treatment. These models are often used in the intermediate stages in the evaluation of the progress of orthodontic treatment and in orthognathic surgical treatment planning.[11] When the literature was examined, no study was found that evaluated the accuracy of linear measurements made on digital models taken in the presence of brackets in the mouth in vivo.
Patients with periodontal problems were not included in the study, as it was thought that advanced periodontal destruction may affect the teeth in the time elapsed between the acquisition of a non-bracket model and a model with a bracket, and it was thought that it would adversely affect the reliability of the measurements. For the standardization of the measurements to be made, attention was paid to the absence of missing teeth in the patients and the completion of the permanent dentition. Individuals with congenital anomalies and syndromes were excluded in order not to encounter cooperation problems during the measurement process.
Saleh et al.,[18] concluded that the 3Shape R700 model scanner is a reliable device for converting the surface details of dental plaster models to a 3D digital format. Renne et al.,[19] published a 3D in vitro analysis study on the evaluation of the accuracy of seven different digital scanners. Scanners differed in the speed, accuracy, and precision of total arch scans, with 3Shape TRIOS 3 (3Shape, Copenhagen, Denmark) stating that it provided the best combination of speed, accuracy, and precision. In our study, the 3Shape R700 (3Shape, Copenhagen, Denmark) device was used as the model scanner, and the 3Shape TRIOS3 (3Shape, Copenhagen, Denmark) device was used for intraoral scanning.
In one study, intraoral scans were taken from patients using both iTero (Align Technology) and Trios (3Shape, Copenhagen, Denmark) intraoral scanners before and after the attachment of orthodontic brackets, and the effect of orthodontic brackets on intraoral scanning was evaluated.[20] The deviations between the surfaces were determined by superpositioning the bracketed and non-bracketed images. The results of this study show that the accuracy of bracketed intraoral scans is clinically acceptable in orthodontics. The upper and lower arch circumferences, upper and lower arch lengths, upper and lower intercanine measurements, upper and lower interpremolar measurements, and upper and lower intermolar measurements of the cases scanned with the bracketless and bracketed 3Shape TRIOS3 (3Shape, Copenhagen, Denmark) intraoral scanner support the results of this study (P > 0.05).
Wiranto et al.,[10] found significant differences between model scans and plaster models for width measurements of some teeth in their study, but these differences were considered clinically insignificant because they were smaller than 0.2 mm. They found an insignificant difference between intraoral scanning models and plaster models in all measurements. They reported that the threshold value considered clinically significant in the mesiodistal sum of 12 teeth from the first molar to the opposite arch first molar was 1.5 mm. In our study, similar to this study, the upper arch and lower arch circumference values of the patients who underwent intraoral scanning without brackets were found to be significantly higher than those on whom non-bracket model scanning was performed (P = 0.022; P < 0.05), (P = 0.001; P < 0.01). However, since the difference between the model scans and the intraoral scans was <1.5 mm, it was found to be clinically acceptable.
In one study, intraoral scans of one patient were scanned with an iTero (Align Technologies, San Jose, CA) intraoral scanner, and plaster model scans were scanned with both iTero (Align Technologies, San Jose, CA) and D250 (3Shape, Copenhagen, Denmark) model scanners. Three groups were formed.[21] All scans were repeated 10 times and overlapped, and the areas with the highest inconsistency in the models were determined. Deviations in the iTero oral and model scan images were observed mostly on the labial surfaces of the maxillary teeth, and the deviations in the mandible were found to be significantly lower than in the maxilla. In our study, the upper arch circumference values of the patients who underwent intraoral scanning with brackets were found to be significantly higher than those who underwent bracket model scanning (P = 0.001; P < 0.01). The difference between the upper arch circumference measurements in bracketed intraoral scanning and model scanning was 2.04 mm. Since this difference was >1.5 mm, it was the only clinically significant finding.
In our study, statistically significant differences were found in the upper and lower arch circumference measurements in the comparisons between non-bracket model scans and intraoral scans. Upper arch circumference was measured with an average of 1.4 mm, and lower arch circumference was measured with an average of 0.7 mm in intraoral scanning. Statistically significant differences were found between upper arch circumference and lower intercanine measurements in comparisons between bracketed model scanning and intraoral scans. Lower intercanine measurements were overestimated on the mean 0.4 mm model scan. This difference is clinically insignificant. These differences between model scans and intraoral scans are thought to be due to alginate contraction.
CONCLUSION
There was no significant difference in the measurements made in intraoral scans scanned with and without brackets.
No significant difference was observed in the measurements made on the model scans with and without brackets.
In the measurements made on the intraoral scan images scanned with brackets and the model images scanned with brackets, a significant difference was found in the upper arch circumference and lower intercanine distances.
In the measurements made on the intraoral scan images scanned without brackets and the model images scanned without brackets, a significant difference was found in the measurements of the upper and lower arch circumferences.
Ethical approval
This study was approved by the Ethics Committee of the Karadeniz Technical University Faculty of Dentistry. (2022/4.07/09/2022).
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Consistency of orthodontic treatment decisions relative to diagnostic records. Am J Orthod Dentofacial Orthop. 1991;100:212-9.
- [CrossRef] [PubMed] [Google Scholar]
- Errors and discrepancies in measurement of tooth size. J Dent Res. 1960;39:405-14.
- [CrossRef] [PubMed] [Google Scholar]
- An evaluation of the use of digital study models in orthodontic diagnosis and treatment planning. Angle Orthod. 2005;75:300-4.
- [Google Scholar]
- Reproducibility of an intraoral scanner: A comparison between in-vivo and ex-vivo scans. Am J Orthod Dentofacial Orthop. 2018;154:305-10.
- [CrossRef] [PubMed] [Google Scholar]
- Application of intra-oral dental scanners in the digital workflow of implantology. PLoS One. 2012;7:e43312.
- [CrossRef] [PubMed] [Google Scholar]
- Full arch scans: Conventional versus digital impressions--an in-vitro study. Int J Comput Dent. 2011;14:11-21.
- [Google Scholar]
- Will digital impressions eliminate the current problems with conventional impressions? J Am Dent Assoc. 2008;139:761-3.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of measurements made on digital and plaster models. Am J Orthod Dentofacial Orthop. 2003;124:101-5.
- [CrossRef] [PubMed] [Google Scholar]
- Validity, reliability, and reproducibility of linear measurements on digital models obtained from intraoral and cone-beam computed tomography scans of alginate impressions. Am J Orthod Dentofacial Orthop. 2013;143:140-7.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of the presence of orthodontic brackets on intraoral scans. Angle Orthod. 2021;91:98-104.
- [CrossRef] [PubMed] [Google Scholar]
- Digital versus conventional impressions for fixed prosthodontics: A systematic review and meta-analysis. J Prosthet Dent. 2016;116:184-90.e12.
- [CrossRef] [PubMed] [Google Scholar]
- Validity and reliability of intraoral scanners compared to conventional gypsum models measurements: A systematic review. Eur J Orthod. 2016;38:429-34.
- [CrossRef] [PubMed] [Google Scholar]
- Accuracy, reliability, and efficiency of intraoral scanners for full-arch impressions: A systematic review of the clinical evidence. Eur J Orthod. 2016;38:422-8.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of digital intraoral scanners and alginate impressions: Time and patient satisfaction. Am J Orthod Dentofacial Orthop. 2018;153:534-41.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment comfort, time perception, and preference for conventional and digital impression techniques: A comparative study in young patients. Am J Orthod Dentofacial Orthop. 2016;150:261-7.
- [CrossRef] [PubMed] [Google Scholar]
- Diagnostic accuracy of impression-free digital models. Am J Orthod Dentofacial Orthop. 2013;144:916-22.
- [CrossRef] [PubMed] [Google Scholar]
- Accuracy and reproducibility of linear measurements of resin, plaster, digital and printed study-models. J Orthod. 2015;42:301-6.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of the accuracy of 7 digital scanners: An in vitro analysis based on 3-dimensional comparisons. J Prosthet Dent. 2017;118:36-42.
- [CrossRef] [PubMed] [Google Scholar]
- Precision of intraoral digital dental impressions with iTero and extraoral digitization with the iTero and a model scanner. Am J Orthod Dentofacial Orthop. 2013;144:471-8.
- [CrossRef] [PubMed] [Google Scholar]




