

Translate this page into:
The effects of the twin arch bracket system in class 1 orthodontic patients for a control of orthodontic tooth movement: A randomized controlled clinical trial

*Corresponding author: Mahmoud M. Fathy Aboelmahasen, Department of Orthodontics, Faculty of Dental Medicine, Al-Azhar University, Cairo, Egypt. mahmoudfathy.209@azhar.edu.eg
-
Received: ,
Accepted: ,
How to cite this article: Farahat MB, Aboelmahasen MM, Elghetany R. The effects of the twin arch bracket system in class 1 orthodontic patients for a control of orthodontic tooth movement: A randomized controlled clinical trial. APOS Trends Orthod. doi: 10.25259/APOS_211_2024
Abstract
Objectives
Regarding the orthodontic appliance type or design, many factors play a role in the desired tooth movement (slot size, inter-bracket span, archwire size, material, etc.). The double slot bracket’s system is a pre-adjusted edgewise bracket featuring two horizontal slot sizes (0.022 and 0.018). The present study aimed to evaluate the efficacy of the twin arch bracket system during the leveling and alignment stage of orthodontic treatment.
Material and Methods
The present study was conducted on 20 patients who were recruited between 2022 and 2024. Patients were divided randomly into two equal groups: The experimental group (group I), which included 10 patients who were treated using the twin arch brackets system, while the Control group (group II) included 10 patients who were treated using the conventional pre-adjusted edgewise brackets system. Patients have been assessed for the first 5 months (T0-T10). The primary outcome is Little’s Index of irregularity and percentage of change, while the secondary outcomes are pain evaluation and assessment of oral hygiene status.
Results
By comparing a percentage of change in little’s irregularity index for both arches between the two groups, the experimental group recorded values that were significantly greater than that recorded in the control group at all-time intervals (T0-T9) but at T10. Both groups recorded (100 ± 0%), with no significant difference between groups (P = 1).
Conclusion
The twin arch bracket system can produce a greater effect for correction of crowding than the conventional pre-adjusted edgewise brackets system during the leveling and alignment stage, but it can induce a higher pain level and offends the oral hygiene status more than the conventional one.
Keywords
Twin arch bracket system
Double slot
Pain level
Little’s irregularity index
Oral hygiene index

INTRODUCTION
The orthodontic bracket plays an important role in fixed orthodontic treatment as they used to transmit the force from the fixed orthodontic appliance to the tooth structure.[1,2] Theoretically, the changes in the conventional pre-adjusted bracket design and the number of its components as wings, vertical slots, and horizontal slots, will affect the quality and quantity of the orthodontic tooth movement (OTM).[3,4] Theoretically, doubling the horizontal bracket slot will double the exerted orthodontic force applied to the tooth structure.[5]
Alignment and leveling of teeth generally constitute the most important preliminary clinical phase of any orthodontic treatment with fixed appliances.[6] During the leveling and alignment stage, tooth movement is directly affected by many factors, such as inter-bracket distances,[7] bracket width, archwire selection, and the friction generated between the bracket and the archwire.[8,9]
The force moment within the bracket slot generated by the interaction between the archwire and the bracket slot is critical for the force exerted from the archwire to be transferred to the malpositioned tooth.[10,11]
The geometric structure of the bracket plays an important role during OTM, especially the slot width, which determines the efficiency of the force moment and the inter-bracket span, which is one of the crucial factors affecting the effectiveness of tooth displacement.[8] It has been established that a sufficient inter-bracket span enables the flexible archwire to activate its springiness caused by deflection.[10] Wider brackets almost develop an adequate force moment, but the subsequent decrease in the space between the brackets will reduce the effective length of the archwire segments between the supports.[12]
Despite there are numerous bracket designs, one feature has remained unchanged: there is only one single horizontal slot on the facial surface of the bracket. In some design variations, such as the Tip-Edge Plus, In-Ovation, and “R” brackets, an additional horizontal slot is enclosed within the bracket base and is not open to the labial surface, therefore only allowing for the engagement of segmental auxiliary archwires.[11,13]
However, some inventors designed bracket systems that could fit two archwires simultaneously by incorporating two horizontal slots in the design of single brackets; they called it “the twin wire appliance.” In these designs, the bracket width is doubled without decreasing the inter-bracket span.[13]
In 2008, there was an experimental study for the efficiency of double-slot brackets in the correction of malposed teeth placed in a wax typodont. The study revealed that a twin-slot bracket doubles the rate of teeth alignment due to the force on the tooth bonded with the twin-slot bracket being doubled, and the rate of wax flow is likely to be proportional to load.[11]
The orthodontic work with two archwires simultaneously was present in previous orthodontic appliances.[11] The background of this idea was to achieve better control of the teeth movements.[14] In the literature, we found very little reference to that type of technique. In the 1930s, attempts were made to develop a new treatment method with this concept. Spencer Atkinson was the pioneer. He created a bracket with a vertical and a horizontal slot, positioned one on top of the other.[15]
Due to the promising results obtained from the previous experimental study and the lack of clinical study results, it will be beneficial to compare clinically little’s irregularity index, oral hygiene status, as well as pain assessment of the twin arch brackets versus conventional brackets during the initial leveling and alignment stage of treatment.
MATERIAL AND METHODS
Study design
This was a randomized, controlled clinical study.
Study setting and population
The present study was conducted on a sample of 20 orthodontic patients seeking orthodontic treatment from the orthodontic clinic, Department of Orthodontics, Faculty of Dental Medicine, Boys, Al-Azhar University, Cairo.
Sample size calculation
Based on a previous clinical study, a sample size calculation was undertaken Using the G power statistical power analysis program (version 3.1.9.7) for sample size determination. A total sample size of 20 (10 in each group) will be sufficient to detect an effect size ranging from 0.86 to 0.87, with an actual power (1-β error) of 0.8 (80%) and a significance level (α error) of 0.05 (5%) for the two-sided hypothesis test.[16,17]
Inclusion criteria
The patients who were included in the present study had the following criteria:
Female patients of age ranges from 13 to 18 years
Full set of permanent teeth (the third molars are not considered)
Angle class I malocclusion with normal facial proportions
Mild-to-moderate crowding (2–5 mm deficiency) in both arches that require treatment with fixed appliance using a non-extraction approach.
Ethical considerations
The present study was approved by the Research Ethics Committee of the Faculty of Dental Medicine, Boys, Cairo, Al-Azhar University, Cairo, Egypt, with code (653/253). Furthermore, the present study was registered on the clinical trials.gov by ID NCT05071599.
Furthermore, the objectives of the study were discussed with the patients, parents, and guardians, and an informed consent form and the orthodontic instructions sheet were signed before the start of orthodontic treatment.
Study groups
The selected patients were divided randomly into two equal groups according to the type of bracket system that was used for leveling and alignment as follows: The experimental group (group I) included 10 patients who were treated using a twin arch brackets system, while Control group (group II) included 10 patients who were treated using the conventional pre-adjusted edgewise brackets system.
Groups’ randomization
The patients involved in the study groups were randomly distributed through a simple online generated randomization plan using online software found at the website http://www.graphpad.com/quickcalcs/index.cfm. The allocation ratio is 1:1.
Orthodontic records
The following standardized orthodontic records were taken for each patient for both groups [Figures 1 and 2]:
Extra-oral and intra-oral photographs before and after orthodontic treatment
Intra-oral scans: before treatment (T0), and each week in the first 6 weeks after installation of the fixed orthodontic appliance (T1, T2, T3, T4, T5, and T6), then each month until the 5th month (T7, T8, T9, and T10) [Figure 3]
Digital lateral cephalometric radiograph before and after orthodontic treatment 4. Digital panoramic radiograph before and after orthodontic treatment.
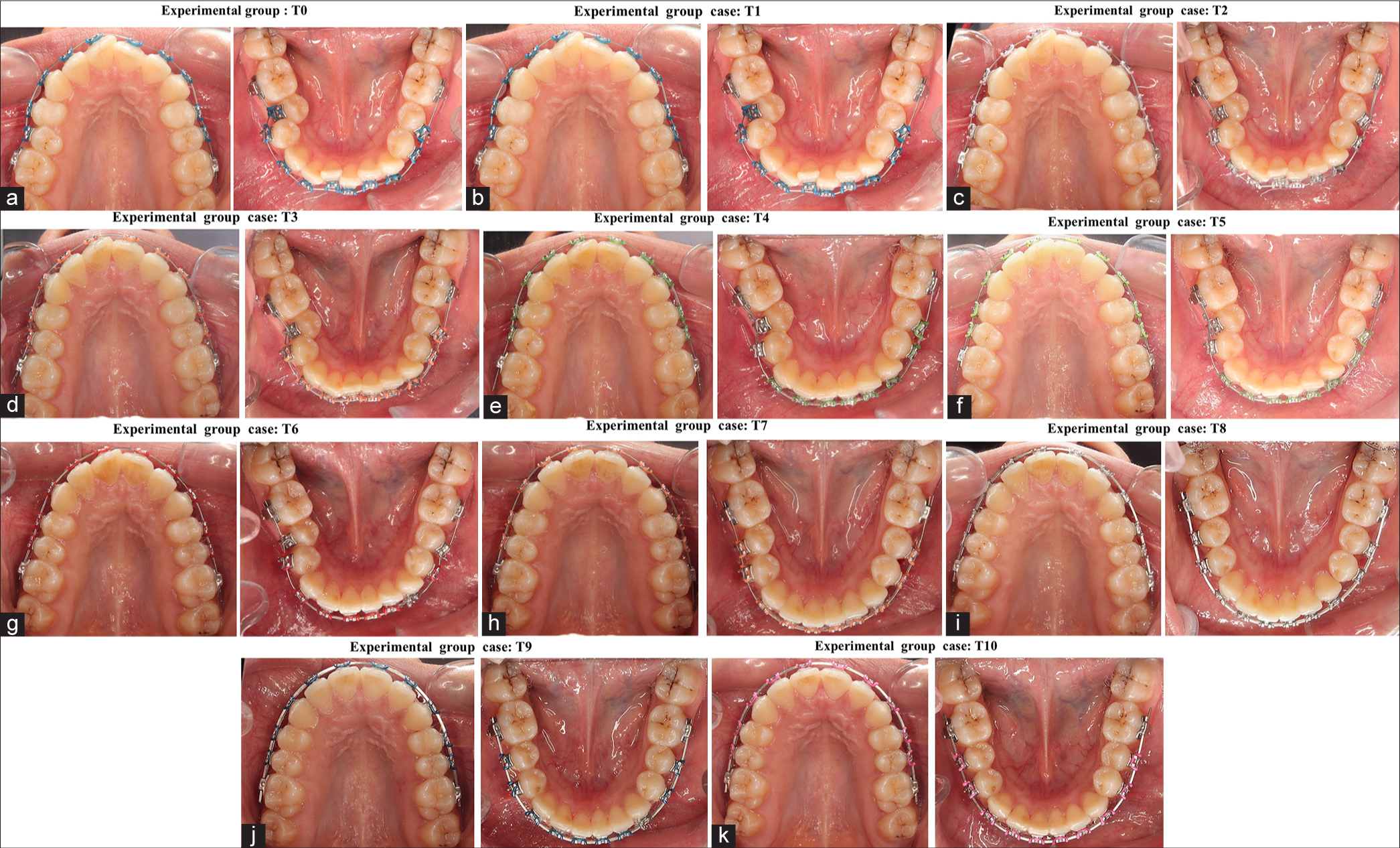
- (a-k) Progressive intra-oral photographs for an experimental group patient at each measurement point.
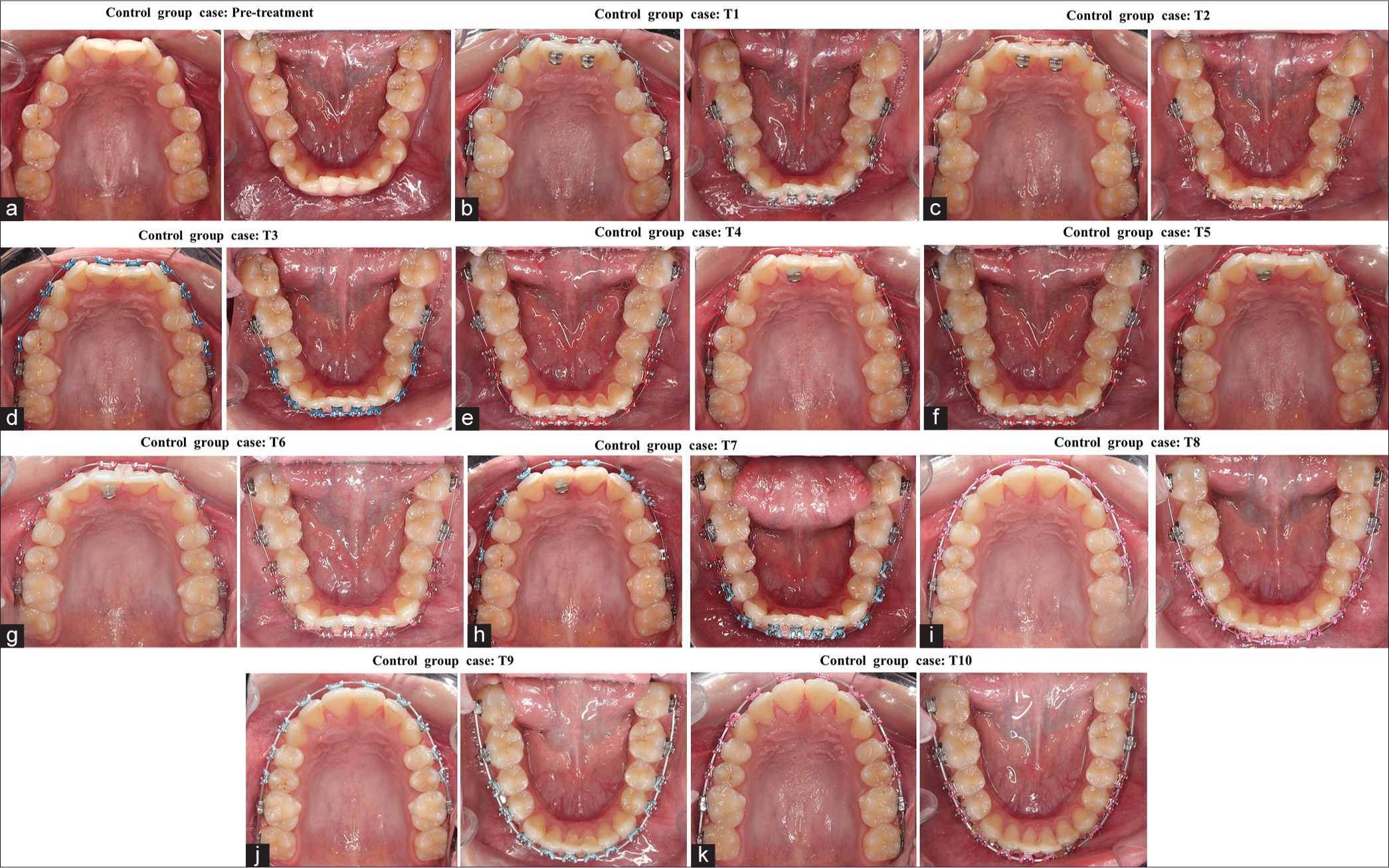
- (a-k) Progressive intra-oral photographs for a control group patient at each measurement point.
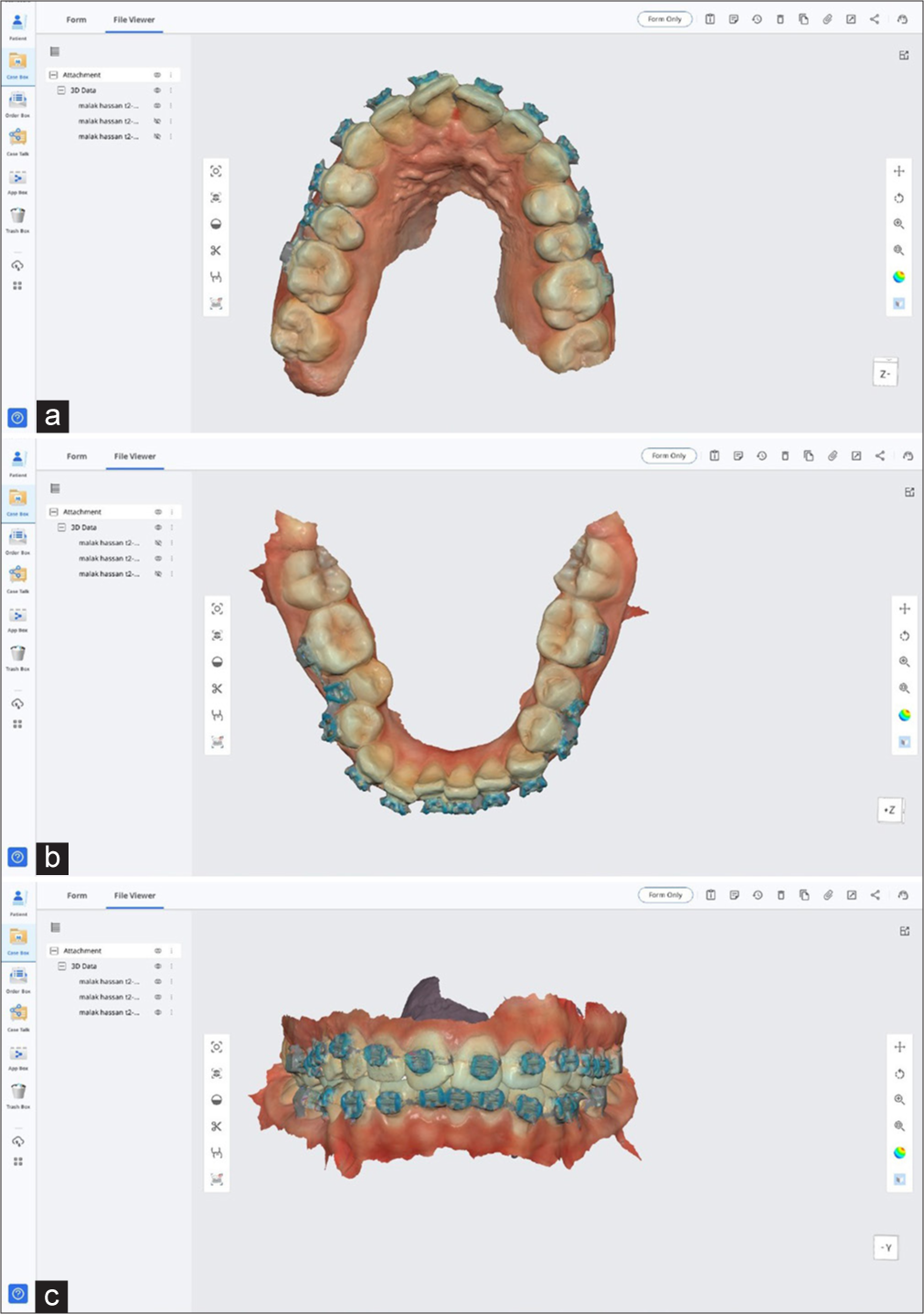
- (a-c) Digital dental model for upper and lower teeth fabricated on IOS software.
Interventional steps
Roth buccal tubes (Roth Buccal Tubes: DTC Buccal Tubes – USA) for the first permanent molars were incorporated with a pre-adjusted bracket system (Ormco mini 2000 twin TM Roth brackets 0.022-inch slot- USA) for a control group of patients, while the double slot brackets kit (Twin arch brackets system: Double Slot Brackets – Sortech Company – Brazil) come included with specific buccal tubes for first and second permanent molars for an experimental group.
The bracket kit for both groups was bonded using the same bonding materials and technique according to a standardized protocol. The adhesive used to adhere brackets to tooth surfaces is a light-cured resin-based composite (Grengloo bracket adhesive system: Ormco Corporation-USA)
The leveling and alignment stage for patients in both groups was performed using the same type and diameter of aligning wires using two wires for an experimental group and a single wire for a control group; the archwire sequences were 0.012-inch (NiTi), followed by 0.014-inch NiTi, 0.016-inch NiTi, 0.016 × 0.022-inch NiTi, 0.017 × 0.025-inch NiTi, and finally, 0.017 × 0.025-in stainless steel on both arches [Figures 4 and 5].
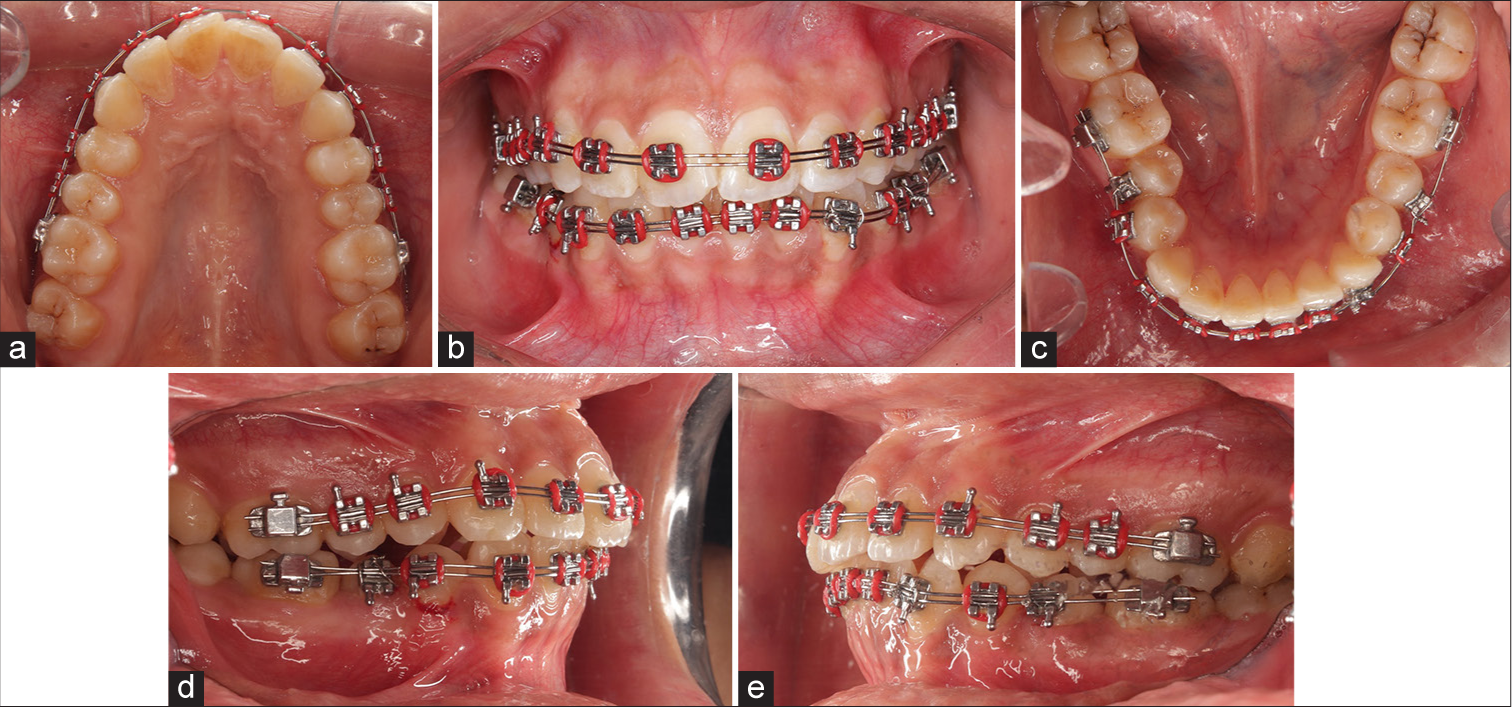
- (a-e) Progressive intra-oral photographs for an experimental group patient.
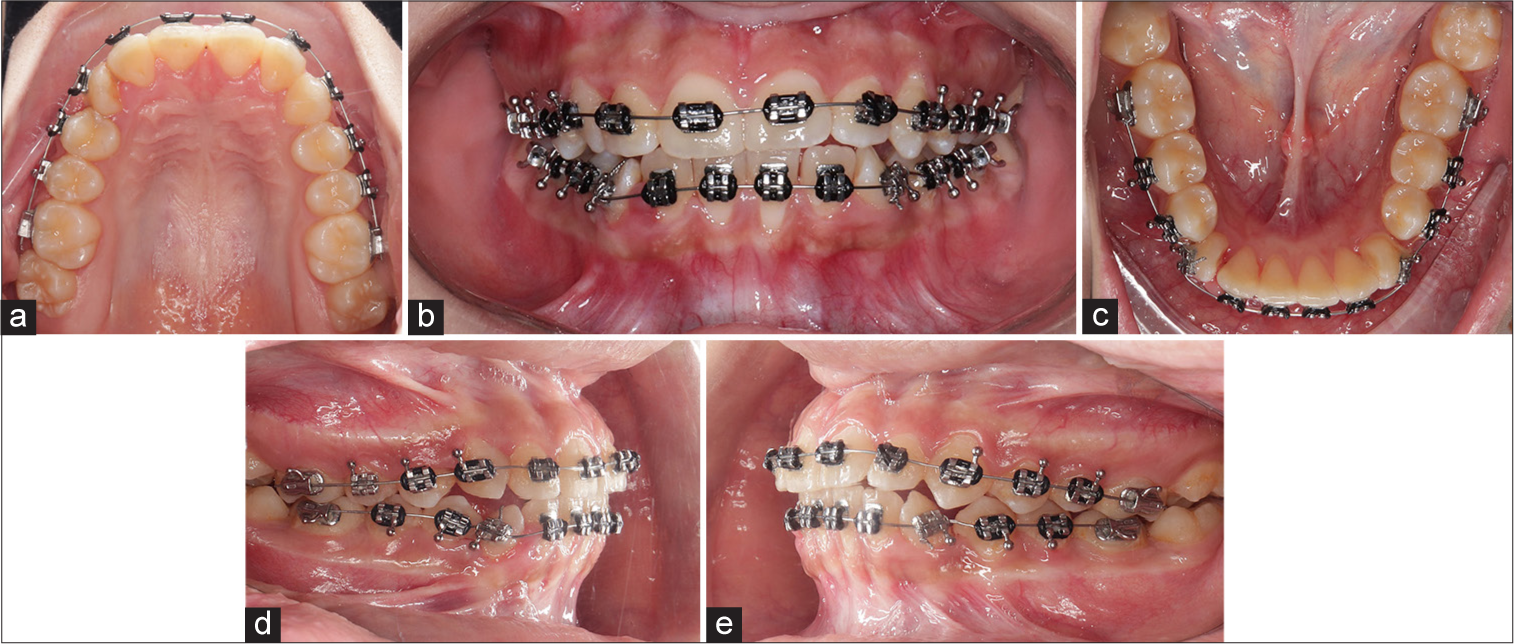
- (a-e) Progressive intra-oral photographs for a control group patient.
Orthodontic outcomes
There are two main outcomes for the current study; the primary outcome is Little’s Index of irregularity (LII) and percentage of change, while secondary outcomes are pain evaluation and assessment of oral hygiene status.
Measurements and observations
LII and percentage of change
The upper and lower arch were directly digitally scanned using Medit i500 IOS before treatment (T0) and every first 6 weeks (T1-T2-T3-T4-T5-T6), then every 1 month, until the 5th month of treatment (T7-T8-T9-T10), digital models were fabricated before, during, and after treatment using the scanner’s software.[18,19]
Using a computer software- 3 Shape Ortho System, LII was measured for upper and lower anterior teeth on digital models using a digital caliper tool before treatment (T0); during the treatment (T1-T10), LII was measured in the following way: the points were put precisely from anatomic contact point of one tooth to anatomic contact point of the adjacent tooth, to obtain five horizontal linear measurements in millimeter for each arch, those horizontal linear measurements were made horizontally parallel to the occlusal plane as much as possible to represent only a horizontal displacement of anatomic contact points for anterior teeth[20-22] [Figure 6].
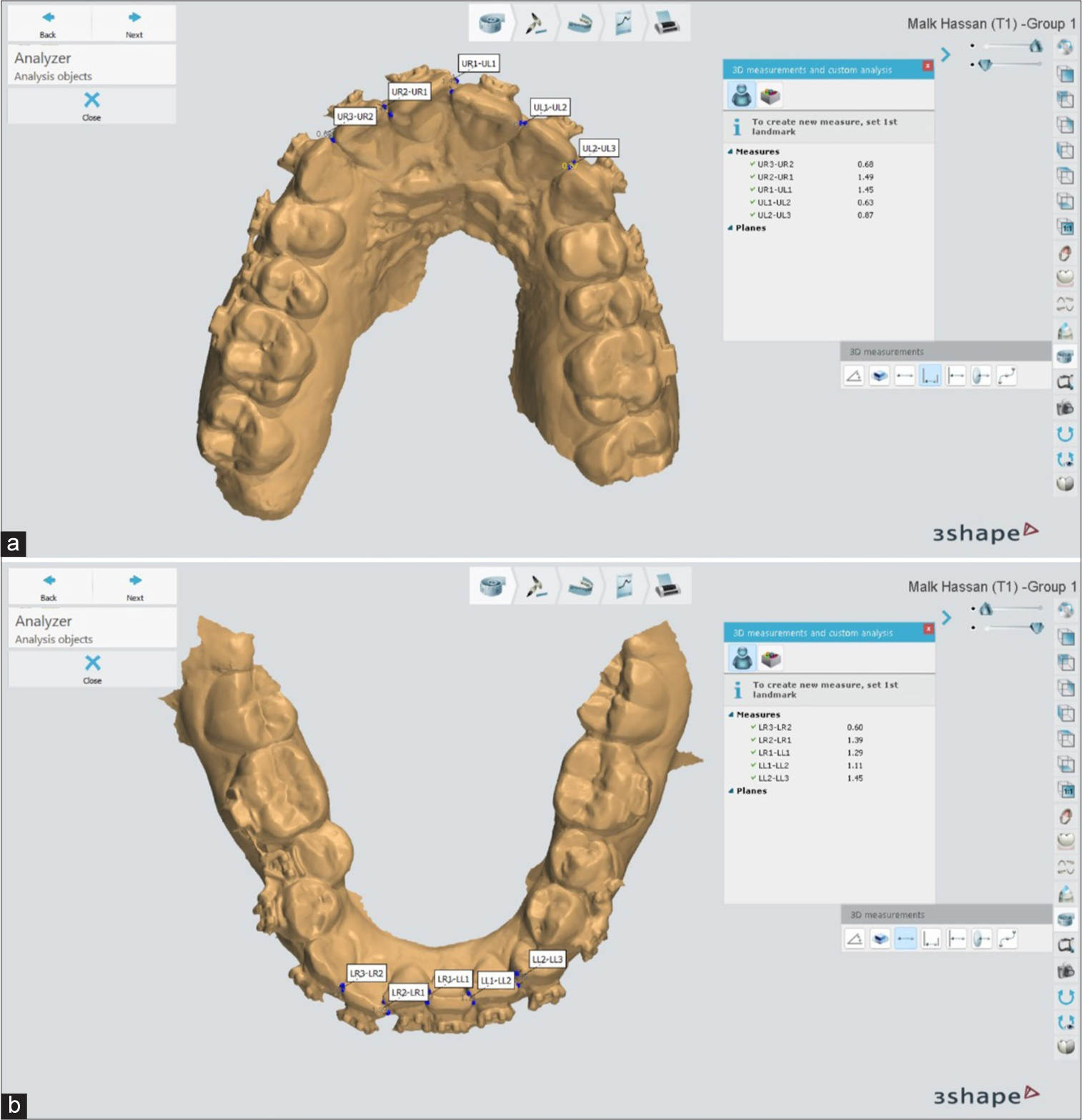
- (a and b) Digital calliper tool has been used to measure Little’s index of irregularity on a digital model using 3Shape Ortho System software.
Ten linear measurements, five for each arch, were performed to estimate LII, which reflected the degree of anterior teeth malalignment improvement from T0 to T10. Then, these ten measurements were recorded. Leveling and alignment improvement percentage (LAIP) was calculated by subtracting the amount of change in the LII value at a specific time point (T1, T2, T7, etc.) from the LII value just before initial wire placement (T0), then the value obtained will be divided on the value of LII at T0 and multiplying by 100, these calculations are represented in the following equation:
LAIP = T(0)-T(X)=Y/T(0) × 100
LAIP: Leveling and alignment improvement percentage (%)
T(0): LII value just before initial wire placement
T(X): LII value at a specific time point (T1, T2, T7, etc.)
Y: Value obtained from subtracting T(0) from (TX).
Pain assessment
Delayed pain evaluation
The pain reported in the first 7 days after insertion of the initial archwire, the initial archwire will be (0.012- or 0.014-inch NiTi) according to the severity of malocclusion present.[23]
Following the initial archwire placement was given a written questionnaire and instructed on how to complete and answer it. The given questionnaire contained the following questions[24,25] [Figure 7]:
Question 1: Have you got pain in (day 1–day 7), yes, or no?
Question 2: Have you consumed any analgesics or painkillers?
Question 3: How much severity of pain was according to the visual analog scale (VAS) index?
![Written questionnaire for assessment of delayed pain according to [Visual analog scale (VAS) Index by Linacre].](/content/9/2025/0/1/img/APOS-211-2024-g007.png)
- Written questionnaire for assessment of delayed pain according to [Visual analog scale (VAS) Index by Linacre].
Immediate pain evaluation
The pain was evaluated and recorded during the tying and untying of the O-tie ligature under chairside conditions according to the VAS index by Linacre; the operator will ask and notice the patient’s reaction to accurately estimate the degree of pain; immediate pain will be evaluated once a month during the first 5 months of the treatment.[23-25]
Evaluation of oral hygiene status
The oral hygiene status has been evaluated for both patient groups of the present study; all patients have been given digital, verbal, and written instructions and instructed to perform oral hygiene instructions according to a standardized protocol. Furthermore, we instructed the patient to use an interdental brush in addition to a conventional toothbrush and chlorhexidine oral rinse if there was a need.[26]
According to the Simplified Oral Hygiene Index (OHI-S) described by Greene and Vermillion, we estimated the oral hygiene status during treatment for each group in the following manner:[27,28] Six surfaces were selected (2 anterior and 4 posterior) as the following: The two anterior surfaces were the labial surface of the upper right and lower left central incisors, while the four posterior surfaces were the buccal surface of the right and left maxillary first permanent molar and the lingual surface right and left mandibular first permanent molars.
The oral hygiene status was evaluated using a conventional mouth mirror and dental probe, and all six selected surfaces were inspected for each patient and recorded in the specific chart. Partially erupted teeth, teeth with full crown restoration, or with restoration on the labial or lingual surface were excluded, according to OHI-S by Greene and Vermillion.
Debris scoring according to OHI-S by Greene and Vermillion:
0 – no debris or stain present, 1 – soft debris covering not more than one the selected third of the tooth surface, 2 – soft debris covering more than one-third of the selected tooth surface, and 3 – soft debris covering more than two-thirds of the selected tooth surface.
Calculus scoring according to OHI-S by Greene and Vermillion:
0 – No calculus present, 1 – supragingival calculus covering not more than one-third of the selected tooth surface, 2 – supragingival calculus covering more than one-third but not more than two-thirds of the selected tooth surface, and 3 – Supragingival calculus covering more than two-thirds of the selected tooth surface or a continuous heavy band of subgingival calculus around the cervical portion of the tooth.
Hygiene index calculation
The debris and calculus scores are summed and calculated to obtain the OHI according to the scoring system recommended by Greene and Vermillion for both patient groups.
Data management and statistical analysis
The data were collected, tabulated, and statistically analyzed using the Statistical Package for the Social Sciences (SPSS program, version 18, Inc., Chicago, IL, USA).
RESULTS
All 20 patients who met inclusion criteria have a complete analysis for LII, percentage of crowding correction, pain assessment, and evaluation of oral hygiene status at all-time intervals (T0 to T10) without any dropping out [Participant Flow Diagram 1]. Each participant has a follow-up every 3 weeks at the orthodontic clinic.
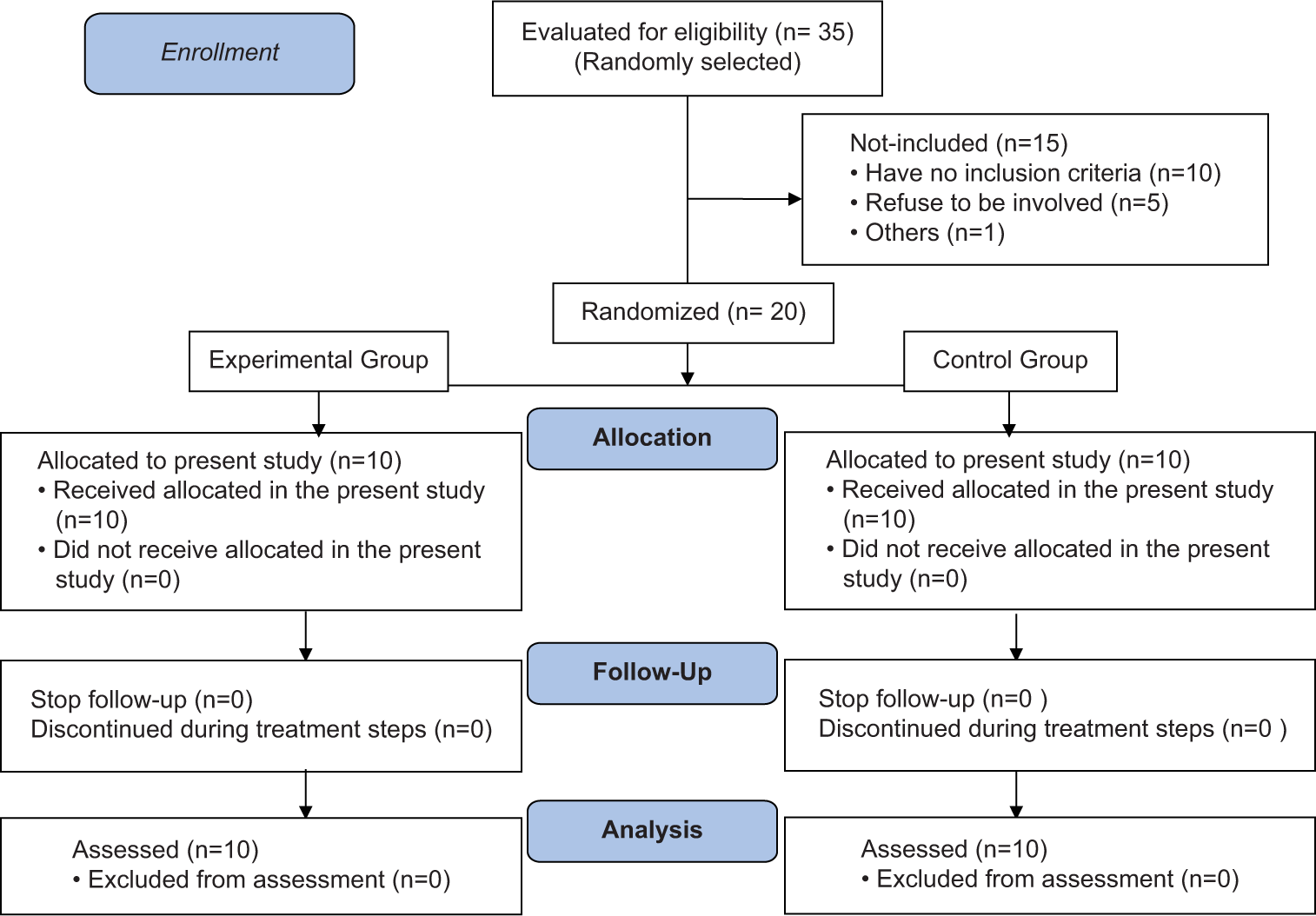
- Participants flow diagram.
Data were explored for normality using the Kolmogorov– Smirnov test of normality. All measurements were non-parametric, so therefore, Mann–Whitney tests were used for inter-group comparison, while the Freidman test and Wilcoxon signed-rank test were used for intragroup comparisons.
LII and percentage of change
By comparison of values of Little’s index for upper and lower arches within the same group, both groups reported that there was a gradual statistically significant decrease, which was noted throughout the study. The difference between different time points was statistically significant (P = 0.000). The post hoc test revealed no significant difference between T9 and T10 [Table 1].
| Groups | Group I | Group II | ||||
|---|---|---|---|---|---|---|
| Mean | Standard deviation | Median | Mean | Standard deviation | Median | |
| T0 | 9.44a | 2.58 | 9.88 | 9.52a | 3.41 | 10.49 |
| T1 | 7.02b | 1.73 | 6.88 | 8.31b | 3.69 | 9.43 |
| T2 | 5.77c | 1.64 | 5.69 | 7.03c | 3.59 | 7.45 |
| T3 | 4.47d | 1.44 | 4.34 | 6.14d | 3.05 | 6.56 |
| T4 | 3.65e | 1.15 | 3.71 | 4.83e | 2.95 | 4.35 |
| T5 | 3.13f | 0.98 | 3.17 | 3.69f | 2.48 | 3.36 |
| T6 | 2.67g | 0.87 | 2.78 | 3.01g | 2.26 | 2.58 |
| T7 | 1.86h | 0.74 | 1.67 | 2.04h | 1.74 | 1.67 |
| T8 | 1.15i | 0.71 | 1.01 | 1.66i | 1.41 | 1.12 |
| T9 | 0.46j | 0.75 | 0.00 | 0.68j | 1.01 | 0.00 |
| T10 | 0.00j | 0.00 | 0.00 | 0.00j | 0.00 | 0.00 |
| P-value within the same group | 0.000* | 0.000* | ||||
Significance level P≤0.05, *Significant, post hoc test, within the same column, values sharing the same superscript letter are not significantly different. (T) for time interval (T0 - T10). (a-j) superscript letters used for statistical significant difference between values, th values have the same superscript letter are not statistically different while whose have different superscript letters, they are statistically different.
On another hand, by a comparison of values of Little’s index for both arches between the two groups, it was noted that there was no significant difference between groups at different time intervals [Table 2].
| Time | Groups | Mean | Standard deviation | Median | Difference | P-value | |||
|---|---|---|---|---|---|---|---|---|---|
| Mean | Standard deviation | C.I. lower | C.I. upper | ||||||
| T0 | Group I | 9.44 | 2.58 | 9.88 | −0.08 | 1.35 | −2.92 | 2.75 | 0.940 ns |
| Group II | 9.52 | 3.41 | 10.49 | ||||||
| T1 | Group I | 7.02 | 1.73 | 6.88 | −1.29 | 1.29 | −4.08 | 1.49 | 0.226 ns |
| Group II | 8.31 | 3.69 | 9.43 | ||||||
| T2 | Group I | 5.77 | 1.64 | 5.69 | −1.26 | 1.25 | −−3.88 | 1.37 | 0.364 ns |
| Group II | 7.03 | 3.59 | 7.45 | ||||||
| T3 | Group I | 4.47 | 1.44 | 4.34 | −1.67 | 1.07 | −3.98 | 0.64 | 0.199 ns |
| Group II | 6.14 | 3.05 | 6.56 | ||||||
| T4 | Group I | 3.65 | 1.15 | 3.71 | −1.19 | 1.00 | −3.37 | 1.00 | 0.450 ns |
| Group II | 4.83 | 2.95 | 4.35 | ||||||
| T5 | Group I | 3.13 | 0.98 | 3.17 | −0.56 | 0.84 | −2.40 | 1.28 | 0.821 ns |
| Group II | 3.69 | 2.48 | 3.36 | ||||||
| T6 | Group I | 2.67 | 0.87 | 2.78 | −0.34 | 0.77 | −2.02 | 1.33 | 0.940 ns |
| Group II | 3.01 | 2.26 | 2.58 | ||||||
| T7 | Group I | 1.86 | 0.74 | 1.67 | −0.18 | 0.60 | −1.45 | 1.09 | 0.683 ns |
| Group II | 2.04 | 1.74 | 1.67 | ||||||
| T8 | Group I | 1.15 | 0.71 | 1.01 | −0.51 | 0.51 | −1.59 | 0.57 | 0.534 ns |
| Group II | 1.66 | 1.41 | 1.12 | ||||||
| T9 | Group I | 0.46 | 0.75 | 0.00 | −0.22 | 0.41 | −1.10 | 0.66 | 0.711 ns |
| Group II | 0.68 | 1.01 | 0.00 | ||||||
| T10 | Group I | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 1 ns |
| Group II | 0.00 | 0.00 | 0.00 | ||||||
C.I.: 95% confidence interval, P≤0.05, ns: Non-significant
As for the comparison of a percentage of change in Little’s irregularity index for both arches between the two groups, the experimental group recorded values that were significantly greater than that recorded in the control group at all-time intervals (T0-T9), but at T10, both groups recorded (100 ± 0%), with no significant difference between groups (P = 1) [Table 3].
| Time | Groups | Mean | Standard deviation | Median | Difference | P-value | |||
|---|---|---|---|---|---|---|---|---|---|
| Mean | Standard deviation | C.I. lower | C.I. upper | ||||||
| T1 | Group I | 24.96 | 6.11 | 25.92 | 11.04 | 3.38 | 3.94 | 18.14 | 0.003* |
| Group II | 13.93 | 8.77 | 11.88 | ||||||
| T2 | Group I | 38.67 | 6.59 | 38.40 | 12.42 | 3.77 | 4.51 | 20.33 | 0.007* |
| Group II | 26.25 | 9.92 | 26.50 | ||||||
| T3 | Group I | 52.77 | 8.62 | 54.38 | 18.38 | 4.17 | 9.61 | 27.15 | 0.000* |
| Group II | 34.39 | 10.00 | 37.75 | ||||||
| T4 | Group I | 59.74 | 11.58 | 61.25 | 14.33 | 5.24 | 3.32 | 25.33 | 0.019* |
| Group II | 45.41 | 11.84 | 46.20 | ||||||
| T5 | Group I | 64.90 | 10.58 | 65.45 | 9.93 | 5.61 | −1.86 | 21.71 | 0.199 ns |
| Group II | 54.97 | 14.23 | 59.30 | ||||||
| T6 | Group I | 70.55 | 9.43 | 69.15 | 7.73 | 5.51 | −3.84 | 19.31 | 0.326 ns |
| Group II | 62.82 | 14.65 | 68.45 | ||||||
| T7 | Group I | 79.61 | 7.72 | 79.90 | 1.59 | 5.07 | −9.06 | 12.25 | 0.880 ns |
| Group II | 78.02 | 14.06 | 81.30 | ||||||
| T8 | Group I | 87.44 | 8.52 | 89.90 | 0.82 | 5.09 | −9.87 | 11.51 | 0.820 ns |
| Group II | 86.62 | 13.65 | 87.50 | ||||||
| T9 | Group I | 94.96 | 8.41 | 100.00 | 1.37 | 4.37 | −7.95 | 10.68 | 0.736 ns |
| Group II | 93.59 | 9.62 | 100.00 | ||||||
| T10 | Group I | 100.00 | 0.000 | 100.00 | 0.000 | 0.000 | 0.000 | 0.000 | 1 ns |
| Group II | 100.00 | 0.000 | 100.00 | ||||||
C.I.: 95% confidence interval, P≤0.05, *significant, ns: Non-significant
Pain assessment
Delayed pain evaluation
As for the comparison of VAS index values related to pain level between the two groups at first 7 days after initial orthodontic wire installation, a significantly higher value was recorded in the experimental group; in comparison to the control group, the difference between groups was statistically significant [Table 4].
| Time | Groups | Mean | Standard deviation | Median | Difference | P-value | |||
|---|---|---|---|---|---|---|---|---|---|
| Mean | Standard deviation | C.I. lower | C.I. upper | ||||||
| Day 1 | Group (I) | 4.00 | 0.00 | 4.00 | 0.80 | 0.13 | 0.50 | 1.10 | 0.000* |
| Group (II) | 3.20 | 0.42 | 3.00 | ||||||
| Day 2 | Group (I) | 3.40 | 0.52 | 3.00 | 1.30 | 0.19 | 0.89 | 1.71 | 0.000* |
| Group (II) | 2.10 | 0.32 | 2.00 | ||||||
| Day 3 | Group (I) | 2.70 | 0.48 | 3.00 | 0.90 | 0.20 | 0.47 | 1.33 | 0.001* |
| Group (II) | 1.80 | 0.42 | 2.00 | ||||||
| Day 4 | Group (I) | 2.30 | 0.48 | 2.00 | 1.30 | 0.15 | 0.95 | 1.65 | 0.000* |
| Group (II) | 1.00 | 0.00 | 1.00 | ||||||
| Day 5 | Group (I) | 1.80 | 0.63 | 2.00 | 0.90 | 0.22 | 0.43 | 1.37 | 0.002* |
| Group (II) | 0.90 | 0.32 | 1.00 | ||||||
| Day 6 | Group (I) | 1.10 | 0.74 | 1.00 | 1.10 | 0.23 | 0.57 | 1.63 | 0.001* |
| Group (II) | 0.00 | 0.00 | 0.00 | ||||||
| Day 7 | Group (I) | 0.70 | 0.48 | 1.00 | 0.70 | 0.15 | 0.35 | 1.05 | 0.001* |
| Group (II) | 0.00 | 0.00 | 0.00 | ||||||
C.I.: Confidence interval, Significance level P≤0.05, *Significant, ns: Non-significant
Immediate pain
By comparison of pain levels during tying between the two groups, it was reported that during the 1st and 5th months, a significantly higher value was recorded in the experimental group in comparison to the control group. The difference between groups was statistically significant. While during the 2nd, 3rd, and 4th months, there was no statistically significant difference between the groups [Figure 8]. Regarding a comparison of pain levels during untying between the two groups, it was reported that during the first 3 months, a significantly higher value was recorded in the experimental group in comparison to the control group. The difference between groups was statistically significant. While during the 4th and 5th months, there was no statistically significant difference between groups [Figure 8].
- Box plot illustrating median value of pain level during tying and untying (immediate pain) according to visual analog scale.
Evaluation of oral hygiene status
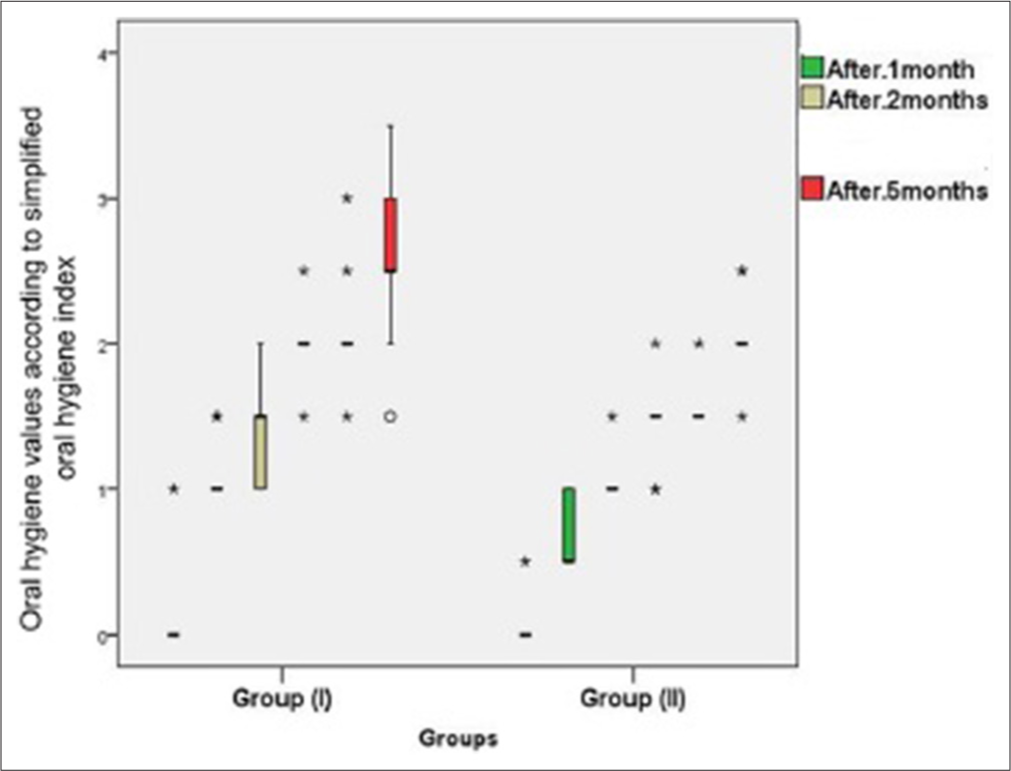
A comparison of OHI values between the two groups revealed that there was a significantly higher value, which was recorded in the experimental group, in comparison to control group II. The difference between groups was statistically significant in the first 5 months of installation of fixed orthodontic appliances [Figure 9].
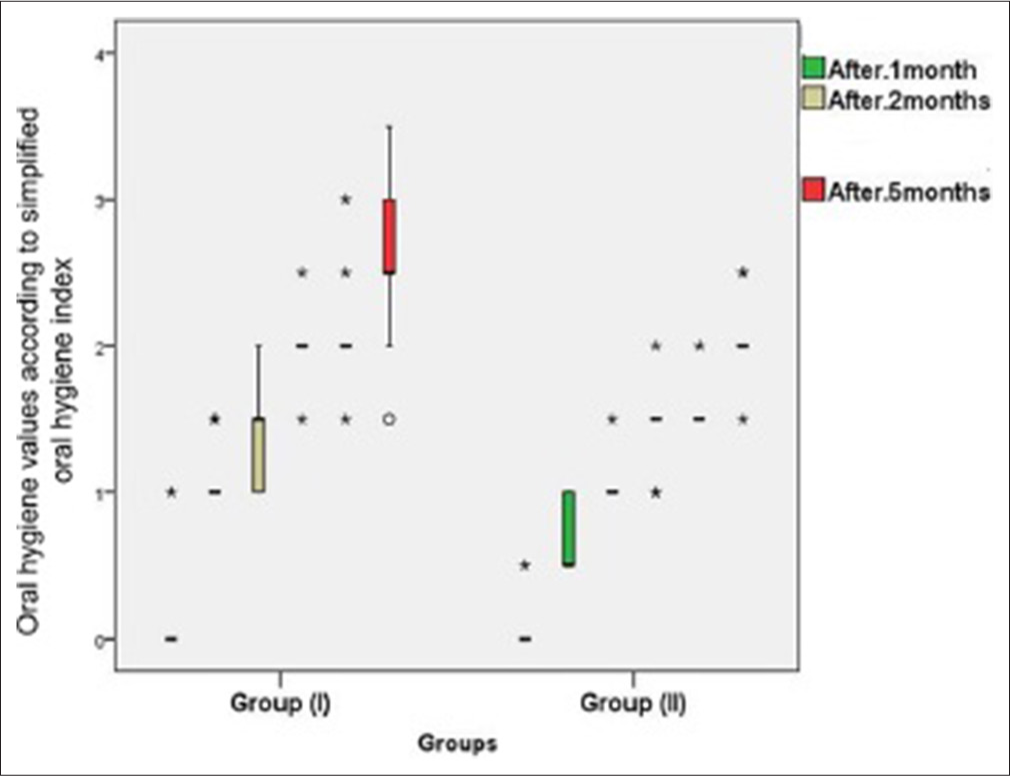
- Box plot illustrating median oral hygiene status (simplified oral hygiene index) in both groups.
DISCUSSION
Alignment and leveling is considered the first stage of orthodontic treatment in nearly all malocclusion problems, specifically in the non-extraction treatment. Alignment refers to the process of bringing malposed teeth into the arch, while leveling refers to correcting the vertical relationship between adjacent teeth.[29] However, regarding the appliance type or design, many factors play a role in the desired tooth movement (slot size, interbracket span, archwire size, material, etc.).[14] The double slot brackets system is a pre-adjusted edgewise bracket featuring two horizontal slot sizes (0.022 and 0.018).[11]
The present study was conducted on 20 female patients aged (13 to 16 years) with a mean age (of 15.3 ± 1.2) (young adult patients). This depends on the that the age of patients is certainly one of subject subject-related factors that affect the rate of OTM. The biological reactions related to tooth movement, such as bone resorption and bone deposition (i.e., bone turnover), are faster in younger patients.[30] In addition, adult age is usually concomitant with periodontal problems (i.e., gingivitis and periodontitis), which, in return, affect the rate of OTM and length of treatment duration. Moreover, apical root resorption and enamel demineralization are complications that show a strong association with adult orthodontic treatment.[31]
Another patient-related factor regarding OTM is patient sex; previous studies show no significance of patient gender on the rate of OTM; nevertheless, estrogen, one of the female sex hormones, plays an important role in bone metabolism (i.e., bone turnover), estrogen levels fluctuate during menstrual cycle phases, so in one way or another hormonal changes in female could interfere with OTM, animals studies show increased estrogen levels decrease alveolar bone remodeling process by inhibiting osteoclastic differentiation and enhancing osteoblast apoptosis; for this reason, high estrogen levels may decrease the rate of OTM.[32,33]
Assessment of pain related to fixed orthodontic therapy may differentiate between boys and girls; commonly, it is believed that boys can tolerate more pain than girls; regarding orthodontic pain, two studies found that females reported more discomfort/pain than males during fixed appliance treatment.[24] Concerning orthodontic pain relation with age, most data reveal higher pain levels in adult patients than in adolescents and preadolescents.[34]
Furthermore, hygiene status during fixed orthodontic therapy varied between males and females; most reports showed that girls brush their teeth more often and have less dental biofilm accumulation during fixed orthodontic treatment, with a lower bracket failure rate than boys.[34]
Conventionally Little’s irregularity index assessment was performed by hand-held caliper and dental stone model, with holding the caliper parallel to the occlusal plane to measure horizontal linear distance between anatomic contact points of adjacent anterior teeth.[21] Recently, with technological advancements in the dental field, the digital models obtained directly from (3D) intra-oral scanners and digital photocopied images for study models have replaced the traditional method, which is certainly done on a specific computer’s software.[35]
The present study depended on intra-oral scanners instead of the traditional impression technique, as measuring LII digitally on a computer’s software has been advocated by two investigators. The previous studies reported that the digital LII measurement method in the upper arch is more reliable than the conventional LII method, and they considered that the digital method of LII assessment is a valid substitute for the traditional method.[36]
Theoretically, doubling an aligning wire (12 or 14 NiTi archwire) will result in doubling a force act on the malpositioned teeth; in response, the rate of tooth movement may increase up to a certain level. Usually, a light continuous force at a certain level that does not cause a total blockage of blood vessels on the pressure side will result in a physiologic continuous tooth movement.[37] A previous typodont study used a twin arch brackets system; doubling the aligning archwires doubles the rate of tooth movement during the alignment phase.[11]
By a comparison of a percentage of change in Little’s irregularity index for both arches between the two groups, the experimental group recorded values that were significantly greater than that recorded in the control group at most time intervals (T0-T9); this can be attributed to the fact that doubling an aligning orthodontic archwire resulted in doubling the orthodontic force that acts on the malposed teeth; also, the orthodontic force can be applied on wider tooth surface area more than that in case of conventional pre-adjusted straight wire bracket system, these results come in agreement with previous studies.[11,38] However, at T10, both groups recorded (100 ± 0%), with no significant difference between groups (P = 1) due to both groups finishing leveling and alignment stage at this time.
Based on the fact that doubling the orthodontic archwire will double pain sensation, especially during the first stage of tissue reaction biological response for orthodontic force, the present study reported that by a comparison of pain levels during tying between the two groups, it was recorded that during 1st and 5th month, a significantly higher value was recorded in the experimental group, in comparison to the control group. The difference between groups was statistically significant. While during the 2nd, 3rd, and 4th months, there was no statistically significant difference between the both groups.[24,25]
As tying and untying steps will induce pain for an affected tooth, especially that controlled by double wire, the present study revealed that by a comparison of pain levels during tying between the two groups, it was reported that during 1st and 5th month, a significantly higher value was recorded in the experimental group, in comparison to the control group. During untying, it was reported that during the first 3 months, a significantly higher value was recorded in the experimental group in comparison to the control one.[24,39]
Fixed appliance components (bracket, o-tie, archwire, etc.) impair self-cleaning action by the tongue and cheeks, so the plaque index scores high in orthodontic patients; in other words, components of the fixed orthodontic appliance endanger patients to dental caries and periodontal diseases, etc. Investigators agreed that orthodontic patients should follow a strict hygiene protocol, and instructions should be strongly stressed before beginning orthodontic treatment.
Consequently, increasing the number of orthodontic appliance components as doubling the horizontal bracket slot, doubling the orthodontic arch wire, increase the size of the bracket system, all these factors will affect the oral hygiene status, so the present study revealed that by comparison of OHI values between the two groups revealed that there was a significantly higher value which was recorded in the experimental group, in comparison to control group II. The difference between groups was statistically significant in the first 5 months of installation of fixed orthodontic appliances.[27-29]
CONCLUSION
The twin arch bracket system produces greater effect for releasing of anterior teeth crowding more than that performed by the conventional pre-adjusted bracket system during leveling and alignment stage
The twin arch bracket system induces greater immediate pain level than the conventional one, also during tying and untying
The twin arch bracket system impairs the oral hygiene status more than the conventional one.
Ethical approval
This study was approved by the Ethical committee of the faculty of dental medicine, Cairo, Boys, Al-Azhar University with ethical code 653/253. The present study was also submitted to ClinicalTrials.gov with the code ID: NCT05071599, dated 13/6/2021.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Association between maxillary and mandibular apical base lengths and severity of dental crowding or spacing in Class II malocclusion subjects: An in-vitro study. J Clin Exp Dent. 2019;11:e49-54.
- [CrossRef] [PubMed] [Google Scholar]
- Assessing the morphological characteristics of teeth and dental arches as potential predictors of dental crowding. Med Pharm Rep. 2023;96:211-20.
- [CrossRef] [PubMed] [Google Scholar]
- Is there a relationship between dental crowding and the size of the maxillary or mandibular apical base? Angle Orthod. 2020;90:216-23.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of dental crowding occurring in mixed dentition in maxillary and mandibular arches based on tooth size-arch length relationships and certain cephalometric parameters. Int J Clin Pediatr Dent. 2023;16:357-62.
- [CrossRef] [PubMed] [Google Scholar]
- Severity of mandibular arch crowding in different sagittal malocclusions. J Adv Pharm Technol Res. 2022;13:S45-9.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical evaluation of dental alignment and leveling with three different types of orthodontic wires. Dental Press J Orthod. 2013;18:31-7.
- [CrossRef] [PubMed] [Google Scholar]
- The first stage of comprehensive treatment: alignment and leveling In: Proffit WR, Fields HW, Sarver DM, eds. Contemporary orthodontics (4th ed). St Louis: Mosby; 2007. p. :551-76.
- [Google Scholar]
- A comparative assessment of torque generated by lingual and conventional brackets. Eur J Orthod. 2012;35:82-6.
- [CrossRef] [PubMed] [Google Scholar]
- Maxillary dental arch changes following the leveling and alignment stage with lingual and labial orthodontic appliances: A preliminary report of a randomized controlled trial. J Contemp Dent Pract. 2014;15:561-6.
- [CrossRef] [PubMed] [Google Scholar]
- Stiffness and frictional resistance of a superelastic nickel-titanium orthodontic wire with low-stress hysteresis. Am J Orthod Dentofacial Orthop. 2007;131:578.e12-8.
- [CrossRef] [PubMed] [Google Scholar]
- The effects of a newly designed twin-slot bracket on severely malpositioned teeth-a typodont experimental study. Eur J Orthod. 2008;30:401-6.
- [CrossRef] [PubMed] [Google Scholar]
- A clinical trial of Damon 2 vs conventional twin brackets during initial alignment. Angle Orthod. 2006;76:480-5.
- [Google Scholar]
- Current products and practice: Tip-Edge Plus. J Orthod. 2007;34:59-68.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontic appliance design. Am J Orthod Dentofacial Orthop. 2007;131:76-82.
- [CrossRef] [PubMed] [Google Scholar]
- Twin-arch technique. Revival of the “edgewise-technique”? J Asian Pac Orthod Soc. 2011;2:1-8.
- [CrossRef] [Google Scholar]
- Porcelain brackets during initial alignment: Are self-ligating cosmetic brackets more efficient? Aust Orthod J. 2010;26:21-6.
- [CrossRef] [Google Scholar]
- How to calculate sample size for different study designs in medical research. Indian J Psychol Med. 2013;35:121-6.
- [CrossRef] [PubMed] [Google Scholar]
- Medit i500-Intraoral scanners and dental software. Available from: https://www.medit.com/medit-i500-intraoral-scanner [Last accessed on 2024 Jun 28]
- [Google Scholar]
- Accuracy of digital and conventional full-arch impressions in patients: An update. J Clin Med. 2020;9:688.
- [CrossRef] [PubMed] [Google Scholar]
- 3Shape ortho system-software improvement and changes. 3Shape. Available from: https://www.3shape.com/en/software-updates/ortho-system [Last accessed on 2024 Jun 28]
- [Google Scholar]
- The irregularity index: A quantitative score of mandibular anterior alignment. Am J Orthod. 1975;68:554-63.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of low-level laser therapy on the time needed for leveling and alignment of mandibular anterior crowding. Angle Orthod. 2022;92:478-86.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontic pain: From causes to management--a review. Eur J Orthod. 2007;29:170-9.
- [CrossRef] [PubMed] [Google Scholar]
- The use of questionnaires in pain assessment during orthodontic treatments: A narrative review. Medicina (Kaunas). 2023;59:1681.
- [CrossRef] [PubMed] [Google Scholar]
- American dental association-mouth healthy. Available from: https://www.mouthhealthy.org/en/az-topics/b/brushing-your-teeth [Last accessed on 2024 Aug 18]
- [Google Scholar]
- The simplified oral hygiene index. J Am Dent Assoc. 1964;68:7-13.
- [CrossRef] [PubMed] [Google Scholar]
- Oral hygiene status among orthodontic patients. J Contemp Dent Pract. 2010;11:25-32.
- [CrossRef] [Google Scholar]
- Leveling and aligning: Challenges and solutions. Semin Orthod. 2001;7:16-25.
- [CrossRef] [Google Scholar]
- Age effects on orthodontic treatment: Adolescents contrasted with adults. Am J Orthod Dentofacial Orthop. 1991;100:523-30.
- [CrossRef] [PubMed] [Google Scholar]
- Effectiveness and duration of orthodontic treatment in adults and adolescents. Am J Orthod Dentofacial Orthop. 1998;114:383-6.
- [CrossRef] [PubMed] [Google Scholar]
- Bone remodeling in post-menopausal osteoporosis. J Dent Res. 2006;85:584-95.
- [CrossRef] [Google Scholar]
- Estrogen effects on orthodontic tooth movement and orthodontically-induced root resorption. Arch Oral Biol. 2020;118:104840.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of orthodontic treatment with fixed appliances on oral health status: A comprehensive study. J Dent Sci. 2011;6:235-8.
- [CrossRef] [Google Scholar]
- Digital models for the analysis of Little's Irregularity Index in subjects with a different degree of crowding: A reproducibility study. Appl Sci (Basel). 2020;10:7108.
- [CrossRef] [Google Scholar]
- The reliability of Little's Irregularity Index for the upper dental arch using three dimensional (3D) digital models. J Dent. 2014;42:1320-6.
- [CrossRef] [PubMed] [Google Scholar]
- Current concepts in the biology of orthodontic tooth movement. Am J Orthod Dentofacial Orthop. 2006;129:458-68.
- [CrossRef] [PubMed] [Google Scholar]
- A review on orthodontic brackets and their application in clinical orthodontics. Cureus. 2023;15:e46615.
- [CrossRef] [Google Scholar]
- Effects of pain associated with orthodontic tooth movement on tactile sensation of periodontal ligaments. Clin Oral Investig. 2023;28:36.
- [CrossRef] [PubMed] [Google Scholar]




