

Translate this page into:
Therapeutic effectiveness of AdvanSync2 at different stages of skeletal maturity in skeletal Class II malocclusion: A single-blind clinical trial


*Corresponding author: Kumar Amit, Department of Orthodontics and Dentofacial Orthopedics, Subharti Dental College, Swami Vivekananda Subharti University, Meerut, Uttar Pradesh, India. doctoramit2010@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Raghav P, Mathur S, Amit K, Mohan S. Therapeutic effectiveness of AdvanSync2 at different stages of skeletal maturity in skeletal Class II malocclusion: A single-blind clinical trial. APOS Trends Orthod 2020;10(2):111-9.
Abstract
Objectives:
AdvanSync2 (Ormco, Glendora, California, USA) is a molar-to-molar fixed Class II corrector, based on the philosophy of Herbst which allows the bonding of the both upper and lower arches simultaneously along with fixed functional therapy. The purpose of this study was to cephalometrically compare the skeletal and dentoalveolar effects of AdvanSync2 in the correction of Class II malocclusions in circumpubertal and post-pubertal patients.
Materials and Methods:
Forty-eight samples were selected and divided into two groups based on their CVMI staging, Group A, i.e., at CVMI Stages 2 and 3 (18 girls and six boys) and Group B, i.e., CVMI Stages 4, 5, and 6 (19 girls and five boys). Cephalograms taken at pre- and post-AdvanSync2 stages were compared and analyzed.
Results:
The results showed that there was a significant increase in mandibular length in both groups. Both the groups also showed sagittal maxillary restriction, maxillary molar distalization, and retroclination of maxillary incisors. On comparison between Group A and Group B, there was no statistically significant differences in terms of maxillary position, size of maxilla, as well as upper and lower incisor inclinations in Group A except for improvement of mandibular position (SNB; P ≤ 0.01) and greater amount of chin growth (B -Pg; P ≤ 0.01) with respect to Group B.
Conclusion:
AdvanSync2 can be used as an effective fixed functional appliance in post-pubertal group for sagittal mandibular correction in skeletal Class II patients.
Keywords
AdvanSync2
Class II corrector
Cephalometric
Circumpubertal
Post-pubertal

INTRODUCTION
Class II malocclusion is common among North Indians accounting for 14.5% of the total malocclusions.[1] An underlying skeletal imbalance either in the form of prognathic maxilla or retrognathic mandible or combination of both is probable in such cases. If patient has retrognathic mandible and seeks intervention in growing stage, functional appliances are the most preferred treatment modality for such malocclusions. These appliances correct the malocclusion and also achieve facial harmony by correcting the skeletal relationship through growth modification.[2]
Removable functional appliances such as activator, bionator, and twin block have been used by many but their results are often compromised due to patient compliance. Fixed functional appliances (FFA) offer better patient compliance and their use has gradually increased since the first such appliance was invented by Emil Herbst in 1909 named as the Herbst appliance. The appliance worked on the philosophy of using a simple telescopic mechanism to position the mandible forward. This mechanism requires well-aligned arches and full slot engagement of final working arch wire in the patients’ mouth before applying the FFA. The major drawback of this appliance system was its size and rigidity that restricted movement and often led to breakages.[3] Furthermore, there was a significant loss of time before such appliances could be used in patients, leading to loss of remaining growth potential in many cases.
In recent years, however, FFAs with molar-to-molar rigid fixation have been introduced, namely, crown Herbst, Mini- scope Herbst, and MARA. These appliances do not require the patients to be on rigid wire before placement of these appliances. Hence, molar-to-molar FFAs can utilize growth potential of the patient, if timed properly. Such appliances can be used in the patient from the very beginning of fixed appliance therapy, which means alignment of arches can be performed simultaneously with growth modification.
A recent introduction to the class of molar-to-molar FFAs is the AdvanSync2 (Ormco, Glendora, California, USA). This is unique in terms of the fact that although it is molar-to- molar FFA, its working principle is based on the philosophy of Herbst. There are only few studies published till date, which have evaluated the effects of AdvanSync2. Chitra et al.[4] suggested that AdvanSync2, when used in post-pubertal stage, shows significant improvement in the Class II skeletal pattern of patients.
The objective of our study was to cephalometrically compare the skeletal and dentoalveolar effects of AdvanSync2 in the correction of Class II malocclusions at circum-pubertal (CVMI 2,3) and post-pubertal (CVMI 4,5,6) growth stages.
Null hypothesis
There is no difference in the effectiveness of AdvanSync2 in both circumpubertal and post-pubertal group.
Study design
This was a prospective single arm clinical trial registered in ICMR with CTRI No. CTRI/2018/03/012423. The study was approved by the Institutional Ethics Review Board.
MATERIALS AND METHODS
The study participants were selected from patients reporting to the outpatient department of our hospital. Following inclusion criteria were considered:
Patients of North India origin with Class II div.1 malocclusion.
Skeletal Class II pattern (ANB >4° <7°) due to retrognathic mandible.
Average to horizontal growth pattern (SN- GoGn ≤32°)
Minimum lower anterior crowding
No missing permanent teeth (clinically or radiographically)
Non-extraction treatment approach.
Patients in mixed dentition stage or with severe dentofacial deformity or those with any systemic disease were excluded from the study. Patients with temporomandibular disorders and ANB ≥ 8° were also excluded.
Forty-eight subjects were selected and divided into two groups of 24 patients each (Groups A and B) based on their CVMI staging. Group A subjects were in CVMI Stages 2, and 3 (circumpubertal) which included 18 girls and six boys while Group B subjects in CVMI Stages 4, 5, and 6 (post-pubertal) included 19 girls and five boys [Table 1]. The sample size was determined using G power version 3.0.10 with power of 0.80. Simple random sampling was done. Case records were taken for each patient at pre- AdvanSync2 (T1) and post-AdvanSync2 (T2), which included cephalometric radiographs, extraoral, and intraoral photographs. Informed consent was obtained from each participant for the use of their case records for scientific research and publication.
| Groups | Females n (%) |
Males n (%) |
Total n (%) |
Age (years) (Mean±SD) |
|---|---|---|---|---|
| A | 18 (75) | 6 (25) | 24 (50) | 12.16±1.69 |
| B | 19 (79.2) | 5 (20.8) | 24 (50) | 16.16±2.28 |
| Total | 37 (77.1) | 11 (22.9) | 48 (100) | 14.16±1.98 |
SD: Standard deviation
Appliance
Fixed mechanotherapy was started and bonding was done between second premolars with 0.022” × 0.028” slot MBT bracket system at T1. AdvanSync2 was placed when 0.019” × 0.025” NiTi wire stage was reached and alignment and leveling stage was complete. Activation of AdvanSync2 was scheduled as per the protocol suggested by Dischinger. The appliance was activated in increments of 2 mm (2 mm shims/C spacers each side) every 3 months until overcorrected Class I molar relationship was achieved. After overcorrection of the sagittal discrepancy, the appliance was removed, and treatment was completed with conventional fixed mechanotherapy. The distal driving force exerted by AdvanSync appliance can cause retroclination of maxillary anterior. Hence, to counteract that high torque MBT brackets were used for maxillary anterior. To counter flaring of mandibular anterior, extra (‒10°) of negative torque was incorporated into the working stainless steel wire in the region of mandibular anterior.
The average length of the AdvanSync2 treatment was 10.5 months (±1.5 months).
Cephalometric analysis
Lateral cephalogram for each patient was taken in the natural head position with the teeth in centric occlusion, using VATECH PAX-400C Digital X-ray system.
Thereafter, the digital cephalograms were imported into a commercial software (Nemoceph NX 2006, Software Nemotec SL, Madrid, Spain) and the magnification of the radiographs was accounted for using known ruler measurements that were captured on the cephalograms. To standardize the radiographs, all magnifications were corrected to 0%. Radiographs were digitally traced by one investigator and were then analyzed using a customized digital analysis, which included 15 skeletal and seven dental measurements. The analysis included a combination of the variables described by Jacobson,[5] McNamara,[6] Ricketts,[7] Steiner,[8] Graber et al.,[9] Burstone et al.,[10] and Tweed.[11] The cephalometric parameters included maxillary skeletal [Figure 1], mandibular skeletal [Figures 1 and 2], maxillomandibular relationship [Figure 2], and dental [Figure 3] parameters.
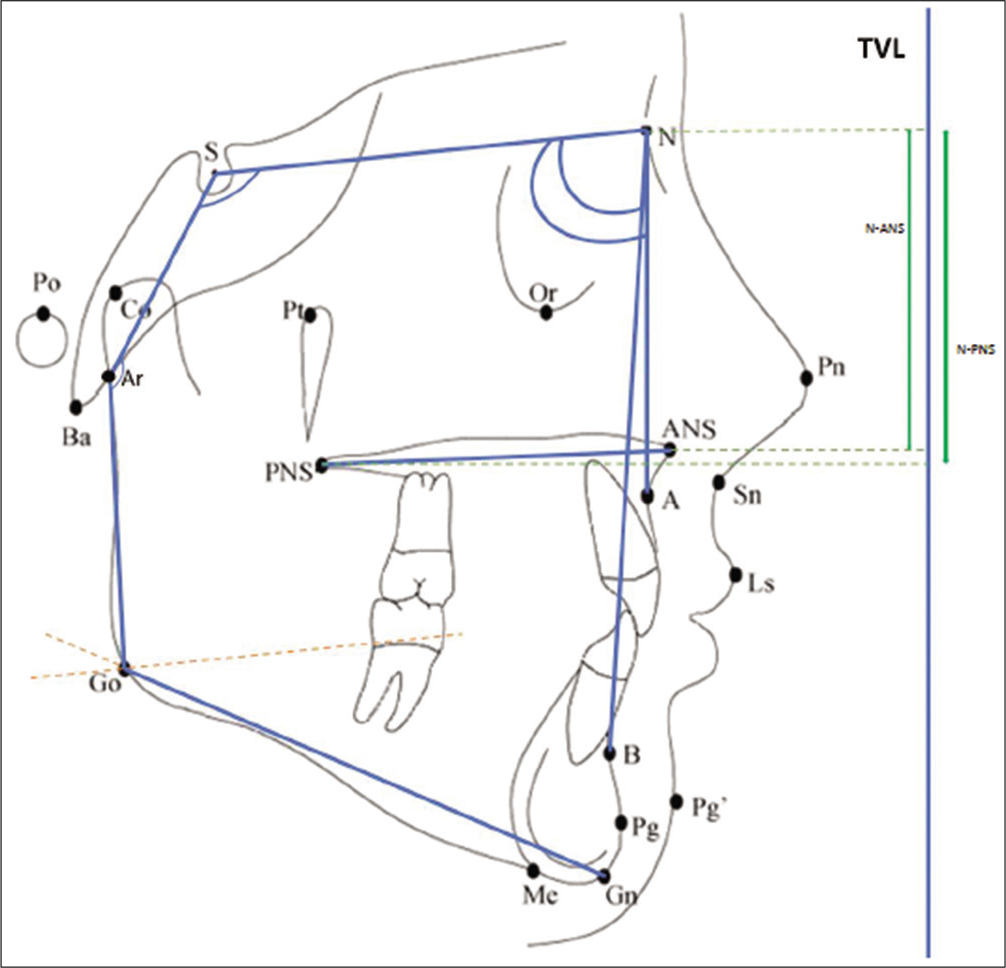
- Maxillary skeletal parameters- A) SNA, B) ANS-PNS, C) N-ANS and D) N-PNS. Mandibular skeletal parameters (i)- A) SNB, B) SN-GoGn, C) Saddle angle and D) Articular angle.
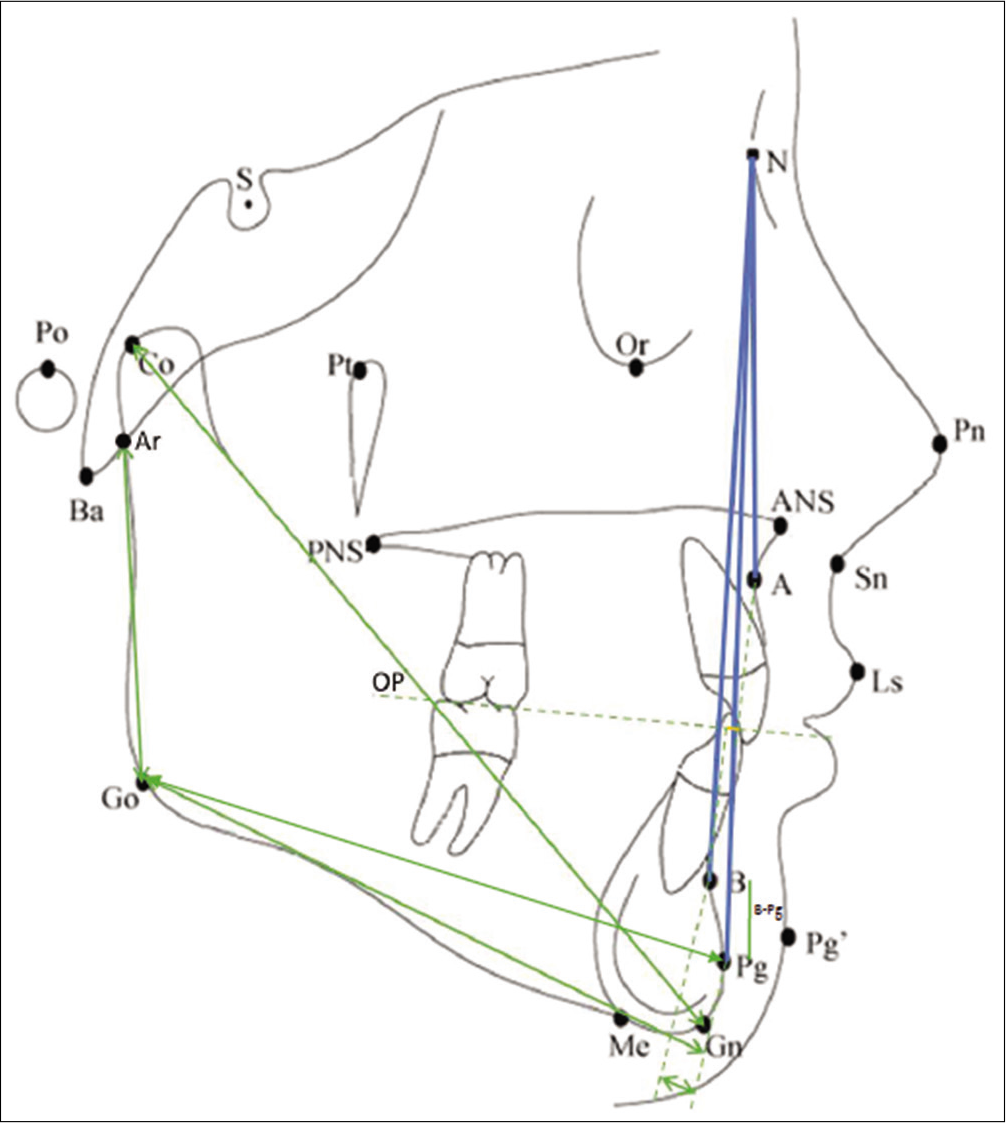
- Mandibular skeletal parameters (ii)- A) Co-Gn, B) Ar-Go, C) Go-Pg and D) B-Pg. Maxillo-mandibular parameters- A) ANB, B) N-A-Pg and C) Wits appraisal.
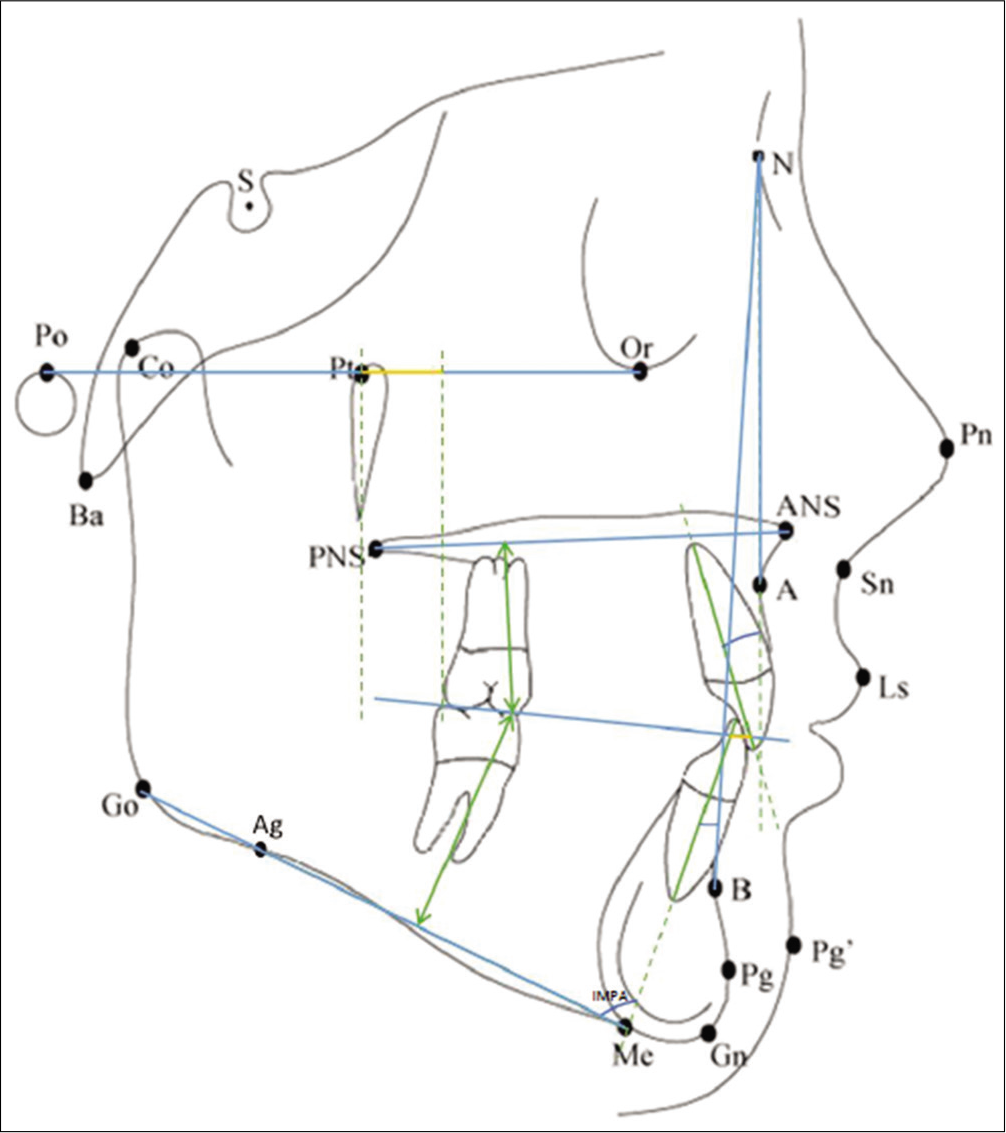
- Dentoalveolar parameters (1)- A) U1-NA, B) L1-NB, C) IMPA and D) Overjet. Dentoalveolar parameters (2)- A) U6-NF, B) U6-Ptv and C) IMPA.
Methodological error
To determine accuracy of the method, 24 cephalograms were randomly selected after 14 days and were retraced and their values were remeasured by the same investigator. Intraclass correlation coefficient was done to check reliability. All the measurements showed high reliability (between 0.95 and 0.98) and were all within 0.5 mm/0.6° of the original.
Statistical analysis
Data were analyzed using SPSS (SPSS version 16 for Windows, Chicago, III). Descriptive statistics were conducted initially, and means and standard deviations were calculated. Data were uniform for individual groups, i.e., Groups A and B separately, parametric test (paired t-test) was performed. When comparing Groups A and B, non-parametric tests were conducted. In the statistical analysis of cephalometric measurements, the Wilcoxon signed-rank test was used to evaluate the changes from pre-treatment to post-treatment. To compare the changes in the two groups, Mann–Whitney U-test was used. Statistical significance was determined at the 0.05 level. According to the power analysis with this level and 80% power the minimum sample size needed for each group was 24.
RESULTS
Post-treatment cephalometric changes after AdvanSync2 application in Group A patients (circumpubertal) are shown in [Table 2]. The cephalometric parameters depict that the combination of AdvanSync2 with preadjusted edgewise appliances, produced statistically significant changes in mandibular position (SNB; 1.76 ± 1.01°), mandibular length (Go-Pg; 3.01 ± 2.4 mm, Co-Gn; 3.98 ± 2.65 mm, Ar-Go;1.65 ± 1.79 mm and B-Pg; 0.6 ± 0.91 mm), and intermaxillary skeletal relationship (ANB; ‒2.33 ± 1.31°, Wits appraisal; ‒2.78 ± 1.69 mm, and A-N-Pg; ‒2.2 ± 1.17°).
| Cephalometric parameters | Before treatment (T1) (mean±SD) | After treatment (T2) (mean±SD) | Mean difference (T2-T1) (mean±SD) | P-value |
|---|---|---|---|---|
| Maxillary skeletal | ||||
| SNA (angle) | 79.14±1.59 | 78.62±1.55 | ‒0.52±1.29 | 0.139 |
| N-ANS (mm) | 47.68±2.87 | 47.93±3.37 | 0.25±2.19 | 0.552 |
| N-PNS (mm) | 50.17±2.39 | 49.57±4.34 | ‒0.6±2.82 | 0.421 |
| Ans-pns (mm) | 52.06±4.97 | 52.96±3.23 | 0.89±2.26 | 0.172 |
| Mandibular skeletal | ||||
| SNB (angle) | 73.16±2.11 | 74.92±2.12 | 1.76±1.01 | 0.001 * |
| SN-Go-Gn (angle) | 28.91±5.37 | 28.98±5.47 | 0.05±2.17 | 0.972 |
| Saddle angle | 124.98±6.81 | 124.64±7.27 | ‒0.34±2.91 | 0.532 |
| Articular angle | 144.25±7.46 | 143.72±6.18 | ‒0.53±4.18 | 0.532 |
| Go-pg (mm) | 65.12±5.98 | 68.13±4.45 | 3.01±2.45 | 0.001 * |
| Ar-go (mm) | 38.78±4.06 | 40.43±4.76 | 1.65±1.79 | 0.004 * |
| B-pg (mm) | 5.66±1.45 | 6.26±1.51 | 0.6±0.91 | 0.02 * |
| Co-Gn (mm) | 98.18±5.95 | 102.17±4.46 | 3.98±2.65 | 0.001 * |
| Maxillomandibular relationship | ||||
| ANB (angle) | 5.98±1.34 | 3.65±1.41 | ‒2.33±1.31 | 0.001 * |
| A-N-Pg angle | 4.15±1.24 | 1.95±1.67 | ‒2.2±1.17 | 0.001 * |
| Wits appraisal (mm) | 5.61±1.87 | 2.83±1.23 | ‒2.78±1.69 | 0.001 * |
| Dentoalveolar | ||||
| IMPA (angle) | 100.82±8.04 | 103.03±7.88 | 2.21±3.51 | 0.014 * |
| UI-NA (angle) | 30.77±7.41 | 29.16±5.87 | ‒1.61±6.21 | 0.28 |
| LI-NB (angle) | 24.74±4.68 | 27.88±4.27 | 3.14±2.24 | 0.001 * |
| U6-NF (mm) | 19.03±2.07 | 20.37±1.58 | 1.34±1.46 | 0.004 * |
| L6-MF (mm) | 25.95±2.75 | 26.11±3.56 | 0.15±2.31 | 0.754 |
| Overjet (mm) | 8.93±1.93 | 5.92±1.82 | ‒3.01±.76 | 0.001 * |
| U6-ptv (mm) | 11.42±2.54 | 12.11±2.329 | 0.68±2.36 | 0.494 |
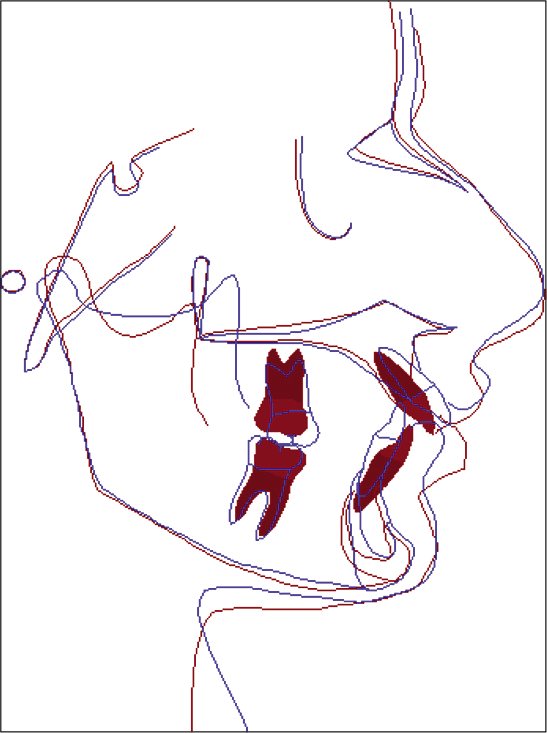
In the dentoalveolar effect, a statistically significant mandibular incisor proclination (IMPA; 2.21 ± 3.51° and L1-NB; 3.14 ± 2.24°) and extrusion of the upper molar (U6-NF; 1.34 ± 1.46 mm) was observed. Other skeletal parameters such as SNA, ANS-PNS, and dental parameters like U1-NA, L6-MF measurements did not show statistically significant changes. [Figure 4] illustrates a typical overall superimposition of a patient treated with the AdvanSync2 in Group A.
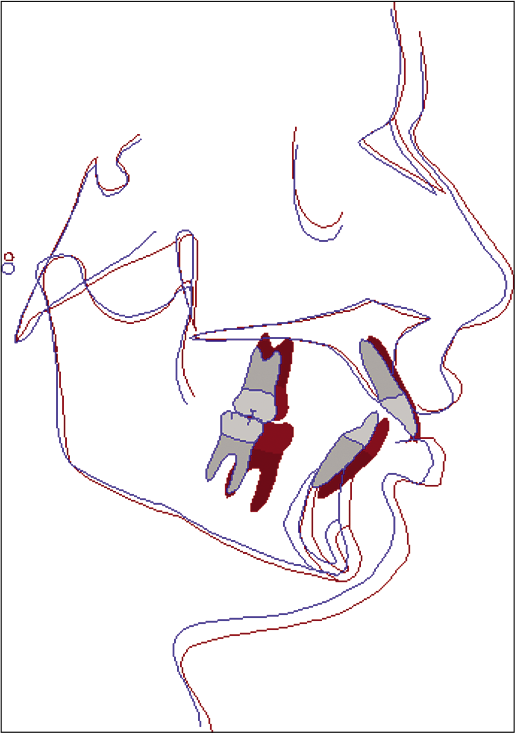
- Typical overall superimposition (along SN at S) of a Group A patient: Blue (pre-treatment) and red (post-treatment).
Post-treatment cephalometric changes after AdvanSync2 application in Group B patients (post-pubertal) are shown in [Table 3]. The skeletal changes showed statistically significant results with respect to maxillary skeletal growth restriction (SNA; ‒0.94 ± 0.97°), improvement in mandibular position (SNB; 0.78 ± 0.72°), mandibular length (Go-Pg; 1.97 ± 2.49 mm, and Ar-Go; 2.02 ± 2.17 mm), and intermaxillary skeletal relationship (ANB; ‒1.72 ± 1.14°, wits appraisal; ‒2.44 ± 2.01 mm and A-N-Pg; ‒2.01 ± 0.59°).
| Cephalometric parameters | Before treatment (T1) (mean±SD) | After treatment (T2) (mean±SD) | Mean difference (T2-T1) (mean±SD) | P-value | |
|---|---|---|---|---|---|
| Maxillary skeletal | |||||
| SNA (angle) | 81.66±2.19 | 80.72±2.66 | ‒0.94±0.97 | 0.006 * | |
| N-ANS (mm) | 45.51±3.65 | 45.59±2.59 | 0.08±3.24 | 0.955 | |
| N-PNS (mm) | 49.67±3.65 | 49.74±4.51 | 0.06±2.25 | 0.864 | |
| Ans-pns (mm) | 54.27±3.63 | 53.81±3.76 | ‒0.46±2.95 | 0.861 | |
| Mandibular skeletal | |||||
| SNB (angle) | 75.28±1.98 | 76.07±2.33 | 0.78±0.72 | 0.006 * | |
| SN-Go-Gn (angle) | 26.25±3.58 | 26.21±3.55 | ‒0.04±1.68 | 1.00 | |
| Saddle angle | 126.47±6.58 | 126.54±7.41 | 0.07±2.75 | 0.57 | |
| Articular angle | 138.88±8.43 | 139.24±8.97 | 0.36±5.61 | 0.753 | |
| Go-pg (mm) | 66.53±3.32 | 68.51±3.54 | 1.97±2.49 | 0.006 * | |
| Ar-go (mm) | 41.93±5.35 | 43.95±4.25 | 2.02±2.17 | 0.002 * | |
| B-pg (mm) | 6.47±2.57 | 6.27±2.54 | ‒0.21±0.54 | 0.168 | |
| Co-Gn (mm) | 102.53±8.35 | 105.25±6.28 | 2.72±4.26 | 0.057 | |
| Maxillomandibular relationship | |||||
| ANB (angle) | 6.38±2.37 | 4.65±2.26 | ‒1.72±1.14 | 0.001 * | |
| A-N-Pg angle | 3.65±2.59 | 1.65±2.22 | ‒2.01±0.59 | 0.001 * | |
| Wits appraisal (mm) | 4.98±2.24 | 2.53±2.92 | ‒2.44±2.01 | 0.001 * | |
| Dentoalveolar | |||||
| IMPA (angle) | 107.11±8.15 | 110.66±5.19 | 3.55±5.62 | 0.05 * | |
| UI-NA (angle) | 33.21±8.14 | 29.06±6.23 | ‒4.14±5.79 | 0.044 * | |
| LI-NB (angle) | 28.91±9.15 | 33.77±8.16 | 4.85±3.61 | 0.002 * | |
| U6-NF (mm) | 20.33±2.88 | 21.39±4.76 | 1.06±4.34 | 0.73 | |
| L6-MF (mm) | 27.41±3.21 | 27.38±3.64 | ‒0.02±1.38 | 0.861 | |
| Overjet (mm) | 8.21±1.73 | 5.27±1.62 | ‒2.94±1.61 | 0.001 * | |
| U6-ptv (mm) | 15.82±2.02 | 14.74±1.85 | ‒1.08±1.25 | 0.008 * | |
Dentoalveolar effects showed mandibular incisor proclination (IMPA; 3.55 ± 5.62° and L1-NB; 4.85 ± 3.61°), maxillary incisors retroclination (U1-NA; ‒4.14 ± 5.79°), and distalization of the upper molars (U6-Ptv; ‒1.08 ± 1.25 mm). [Figure 5] illustrates a typical overall superimposition of a patient treated with the AdvanSync2 in Group B.
- Typical overall superimposition (along SN at S) of a Group B patient: Blue (pre-treatment) and red (post-treatment).
On comparison between Group A and Group B, there was no statistically significant differences in terms of maxillary position, size of maxilla, as well as upper and lower incisor inclinations in Group A except for the improvement of mandibular position (SNB; P ≤ 0.01) and greater amount of chin growth (B -Pg; P ≤ 0.01) with respect to Group B.
DISCUSSION
This single arm clinical trial evaluated the therapeutic effects of AdvanSync2 has been evaluated. AdvanSync2 is a molar- to-molar Class II corrector, which is based on the principles of the Herbst appliance. A total of 48 subjects were selected, with both skeletal and dental Class II malocclusion attributed to retrognathic mandible. The sample was divided into two groups (circumpubertal and post-pubertal), with 24 patients in each group. Group A had 18 girls and six boys, whereas Group B had 19 girls and five boys. As per Gomes and Lima,[12] this sexual dimorphism did not act as a confounding factor in the intragroup homogeneity because when patients are considered according to their skeletal maturation stages, no clear sex differences in annual growth rates have been noted. Hence, classifying subjects by their skeletal stages will diminish or even eliminate sex differences.
The skeletal maturity of the subjects was determined using modified version of the cervical vertebra maturation proposed by Baccetti et al. in the year 2005.[13] The study stated that circumpubertal stage is considered ideal for growth modification by functional appliance therapy. Therefore, in this study, Group A comprised patients in their circumpubertal age, i.e., CVMI 2 and 3. Patients in developmental stage falling in between CVMI 3 and 4 were also included in Group A.
Ruf and Pancherz,[14,15] Konik et al.,[16] and Kinzinger and Diedrich,[17] in separate studies showed that FFAs given in post-pubertal age utilizes the residual growth potential and shows significant skeletal changes. Therefore, our study considered study participants in developmental stages CVMI- 4 and 5 as post-pubertal growth stage, to be part of Group B.
Comparison of the treatment results of circumpubertal and post-pubertal subjects was based on the cumulative effect of physiologic growth and AdvanSync2-induced effects. Since this study was done to differentiate between the skeletal effect induced in circumpubertal and post-pubertal disintegration of the cumulative effects into its components was not intended in this study. Control group, i.e., group of untreated Class II subjects was not formed in this study. The most important reason for this decision was the ethical concern. No subject seeking treatment can be left untreated and hence we did not create any control group for this study.
According to a FEM study by Panigrahi and Vineeth,[18] the biomechanical effect of FFAs showed the posterosuperior displacement of the maxillary dentition and pterygoid plate while the forward and downward displacement of mandible and mandibular dentition, contributing to the correction of Class II malocclusion. The results of this study showed similar effects with some exceptions.
Therapeutic effects of AdvanSync2 on maxilla
The headgear effect of Herbst appliance is well documented in the literature in various studies such as Pancherz and Anehus-Pancherz,[19] Valant and Sinclair,[20] and Wieslander[21] Similarly, Siara-Olds et al.,[22] in their retrospective study, showed that MARA appliance showed a significant headgear effect. Al-Jewair et al.[23] compared skeletal and dentoalveolar effects of MARA and AdvanSync appliances . Both the appliances showed significant increase in total mandibular length, ramus height, and anterior/posterior facial height. However, AdvanSync showed significant headgear effect through maxillary restriction 1° more than MARA.
In our study also, Group B (post-pubertal) showed a reduction in SNA angle by 0.94 ± 0.972° and decrease in linear maxillary length by 0.46 ± 2.954 mm, showing a maxillary restrictive effect which is in accordance with the results of Al-Jewair et al.[23]
In Group A (circumpubertal), there was a reduction in SNA by 0.52 ± 1.296° and increase in ANS-PNS by 0.893 ± 2.260 mm. This statistically insignificant increase in ANS-PNS may be because of the concomitant growth of the maxilla which may have nullified the maxillary restrictive effect of the appliance.
Jayachandran et al.[24] in their study comparing skeletal changes brought about by AdvanSync and Class II elastics showed significant maxillary restriction relative to controls with AdvanSync. SNA was restricted by 2.57° while maxillary length was shorter by 2 mm (A-Nperp.). The results achieved in our study were in accordance with the above study but the amount of change was not as much. This could probably be because of the fact that our study did not include untreated control group.
Therapeutic effects of AdvanSync2 on the mandible
In this study, both groups showed a statistically significant increase in the mandibular length. In Group A, the results showed a mean increase in SNB by 1.76 ± 1.01° (P = 0.001), Go-Pg by 3.01 ± 2.45 mm (P = 0.001), Co-Gn by 3.98 ± 2.65 mm (P = 0.001), Ar-Go by 1.65 ± 1.79 mm (P = 0.004), and B-Pg by 0.6 ± 0.91 mm (P = 0.02), whereas Group B showed a mean increase in SNB by 0.78 ± 0.72° (P = 0.006), Go-Pg by 1.97 ± 2.49 mm (P = 0.006), and Ar-Go by 2.02 ± 2.17 (P = 0.002). The increase in linear mandibular length was more in Group A (circumpubertal), as compared to Group B (post pubertal), though it was statistically insignificant. This may be due to the normal growth potential, present in patients in circumpubertal group.
Accordingly, SNB was significantly increased (P = 0.012) in Group A (1.76 ± 1.012°), when compared to Group B (0.78 ± 0.72°). Hence, Group A (circumpubertal) showed a greater skeletal change, as compared to Group B (post-pubertal).
Group B also showed statistically significant change in mandibular length which was similar to what was observed by Ruf and Pancherz[14] and Konik et al.[16] In their studies, the effect of the Herbst appliance was seen on young adults and post-adolescent patients. Ruf and Pancherz[14] reasoned that even though condylar cartilage matures with age to an adult hypertrophic form, zones of unmineralized growth cartilage and undifferentiated mesenchyme are seen in the adult mandibular condyle. Thus, increase in the mandibular length in young adult group could possibly be due to a reactivation of the cells in the pre-chondroblastic zone.
This growth is induced in post-pubertal stage, when the mandible is allowed to grow in an unrestrictive environment so that its true genetic potential is expressed. This phenomenon is called as “catch-up growth,” which is defined as the height velocity that exceeds the normal limits for the age, for at least 1 year after a period of depressed growth. Catch-up velocity in height can reach 4 times the normal velocity of the chronological age.[1]
Therapeutic effects of AdvanSync2 on the maxillomandibular relationship
AdvanSync2 showed a marked improvement in the Class II profile of the patients. In both the groups of skeletal maturation, there was a statistically significant change in the Class II skeletal pattern of the patients. For both Group A and Group B, there was a decrease in ANB by 2.33 ± 1.31 and 1.72 ± 1.14° (P = 0.001), wits appraisal by 2.78 ± 1.69 mm and 2.44 ± 2.01 mm (P = 0.001) and A-N-Pg by 2.2 ± 1.17 and 2.01 ± 0.59° (P = 0.001), respectively. These readings were in accordance to the change in maxillomandibular relationship seen in some other studies done on AdvanSync.[23,24]
Therapeutic effects of AdvanSync2 on the dentoalveolar relationship
In a systematic review of FFA by Zymperdikas et al.,[25] proclination of the lower incisors was a commonly observed dentoalveolar change due to FFA. Similar results were observed in this study, where the dentoalveolar effect on mandible showed a statistically significant increase in the inclination of the lower incisors in both the groups. Groups A and B (circumpubertal and post-pubertal) showed a mean increase in IMPA by 2.21 ± 3.51° and 3.55 ± 5.62° and L1-NB by 3.14 ± 2.24° and 4.85 ± 3.61°. Although the change in inclination was more in Group B as compared to Group A, the difference between both the groups was statistically insignificant, while comparing other FFAs with AdvanSync2, Aras et al.[26] and Cacciatore et al.[27] who used Forsus device in their studies showed a mean increase in IMPA by 6.14 ± 0.45 and 6.2 ± 5.9, respectively. This greater increase in IMPA can be due to the fact that the Forsus device is attached anteriorly to the main arch wire, while AdvanSync2 is a molar-to-molar FFA, hence showing lesser degree of proclination of the lower anterior.
In the maxillary dentition, treatment with FFA is known to show a distalizing effect on the upper molars with retroclination of maxillary incisors.[20,25] Similar to these effects, the current study also showed retroclination of the upper incisors in both the groups. In Group A, the upper incisors retroclined by 1.61 ± 6.21°, which was statistically insignificant, and in Group B the upper incisors showed a statistically significant amount of retroclination of 4.14 ± 5.79°. This may be due the fact, that the patients in post- pubertal group were bonded before FFA therapy and were on a rigid wire, hence the space created by distalization was utilized by simultaneous retraction, whereas, the patients in pre-pubertal age group were given FFA before bonding.
Along with the retroclination of the upper incisors, a distalizing effect was also seen in the maxillary dentition. There was a statistically significant decrease in U6-Ptv by 1.08 ± 1.25 mm (P = 0.008) in Group B. This distal movement of the upper first molars can be explained by the headgear effect of FFA as stated by Panigrahi et al.[18] in their FEM study, where they observed distalization of maxillary molars as an effect of FFA.
In Group A, the change in U6-Ptv was statistically insignificant, with a mean increase by 0.68 mm (P = 0.494). This may be due to the physiological increase in the maxillary length (ANS-PNS) at the maxillary tuberosity region, hence negating the distalizing effect of the maxillary molars.
Overall, Group B (post-pubertal) showed a statistically insignificant difference (P = 0.058) in the amount of distalization as compared to Group A (circumpubertal).
All these factors, along with an increase in mandibular length and restriction of maxillary growth, contribute to the significant reduction of overjet, seen in both Groups A and B [Table 4]. All the sagittal dentoalveolar effects are similar to the effects shown by Al-Jewair et al.[23] and Jayachandran et al.[24] in their studies on AdvanSync.
| Cephalometric parameters | Group A mean difference (T2-T1) (mean±SD) | Group B mean difference (T2-T1) (mean±SD) | P-value | |
|---|---|---|---|---|
| Maxillary skeletal | ||||
| SNA (angle) | ‒0.52±1.29 | ‒0.94±0.97 | 0.454 | |
| N-ANS (mm) | 0.25±2.19 | 0.08±3.24 | 0.884 | |
| N-PNS (mm) | ‒0.6±2.82 | 0.06±2.25 | 0.493 | |
| Ans-pns (mm) | 0.89±2.26 | ‒0.46±2.95 | 0.158 | |
| Mandibular skeletal | ||||
| SNB (angle) | 1.76±1.01 | 0.78±0.72 | 0.012 * | |
| SN-Go-Gn (angle) | 0.05±2.17 | ‒0.04±1.68 | 1.00 | |
| Saddle angle | ‒0.34±2.91 | 0.07±2.75 | 0.633 | |
| Articular angle | ‒0.53±4.18 | 0.36±5.61 | 0.633 | |
| Go-pg (mm) | 3.01±2.45 | 1.97±2.49 | 0.152 | |
| Ar-go (mm) | 1.65±1.79 | 2.02±2.17 | 0.574 | |
| B-pg (mm) | 0.6±0.91 | ‒0.21±0.54 | 0.005 * | |
| Co-Gn (mm) | 3.98±2.65 | 2.72±4.26 | 0.115 | |
| Maxillomandibular relationship | ||||
| ANB (angle) | ‒2.33±1.31 | ‒1.72±1.14 | 0.28 | |
| A-N-Pg angle | ‒2.2±1.17 | ‒2.01±0.59 | 0.868 | |
| Wits appraisal (mm) | ‒2.78±1.69 | ‒2.44±2.01 | 0.589 | |
| Dentoalveolar | ||||
| IMPA (angle) | 2.21±3.51 | 3.55±5.62 | 0.819 | |
| UI-NA (angle) | ‒1.61±6.21 | ‒4.14±5.79 | 0.48 | |
| LI-NB (angle) | 3.14±2.24 | 4.85±3.61 | 0.308 | |
| U6-NF (mm) | 1.34±1.46 | 1.06±4.34 | 0.084 | |
| L6-MF (mm) | 0.15±2.31 | ‒0.02±1.38 | 0.575 | |
| Overjet (mm) | ‒3.01±.76 | ‒2.94±1.61 | 0.561 | |
| U6-ptv (mm) | 0.68±2.36 | ‒1.08±1.25 | 0.058 | |
Limitations of the study
The division of groups in our study was based on CVMI staging into Group A – CVMI 2, and 3 and Group B – CVMI 4, 5, and 6. Even though the patients between CVMI 3 and 4 were categorized in circumpubertal, CVMI 4 was categorized in the post-pubertal group, i.e., after peak height velocity. This might have brought an overlap in the ideal age of functional appliance therapy, as many studies showed that the mean increase in mandibular length is between CVMI 3 and 4.[28] This could have attributed to the significant skeletal change seen in Group B.
Second, this study was based on the pre and immediate post- AdvanSync2 cephalograms, which did not account for the long-term stability of the results achieved.
Finally, the sample size of this study was comprised only 48 patients with 24 patients in each group. A larger sample size and a multi-centered trial could have given a better understanding of the effects of AdvanSync2 at different stages of skeletal maturation.
CONCLUSION
On comparing the therapeutic effect of molar-to-molar FFA (AdvanSync2) in Class II malocclusion at different stage of skeletal maturity, the following conclusions were drawn:
There was a significant increase in mandibular length in both groups (circumpubertal and post-pubertal). The circumpubertal group (Group A) showed a greater mandibular advancement (SNB) when compared to post-pubertal (Group B)
Maxillary restrictive effect was observed in both the groups, but the effect was significant in post-pubertal group (Group B), showing a significant decrease in SNA
Both Groups A and B, showed mandibular dentoalveolar effects, with proclination of lower incisors, but the mean increase in IMPA was more in post-pubertal group (Group B) when compared to circumpubertal group (Group A)
The distalizing effect on the upper molars and retroclination of the upper incisors was significant in Group B (post-pubertal group), when compared to Group A (circumpubertal group).
Thus, to conclude, the skeletal and dentoalveolar changes were significant in both Groups A and B for the correction of Class II malocclusion and AdvanSync2 can also be used as an effective FFA in post-pubertal group for sagittal mandibular correction in skeletal Class II patients.
Trial registration number
This was a prospective single arm clinical trial registered in Indian Council of Medical Research with CTRI No. CTRI/2018/03/012423.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Orthodontics: Diagnosis and Management of Malocclusion and Dentofacial Deformities India: Elsevier; 2009.
- [Google Scholar]
- The effect of early intervention on skeletal pattern in Class II malocclusion: A randomized clinical trial. Am J Orthod Dentofacial Orthop. 1997;111:391-400.
- [CrossRef] [Google Scholar]
- History, background, and development of the Herbst appliance. Semin Orthod. 2003;1:3-11.
- [CrossRef] [Google Scholar]
- Treatment outcomes in the sagittal and vertical dimensions with the advansync 2 Class II corrector-a case series. J Contemp Orthod. 2018;2:14-26.
- [Google Scholar]
- Perspectives in the clinical application of cephalometrics. The first fifty years. Angle Orthod. 1981;51:115-50.
- [Google Scholar]
- The diagnostic facial triangle in the control of treatment objectives. Am J Orthod. 1969;55:651-67.
- [CrossRef] [Google Scholar]
- The cervical vertebral maturation (CVM) method for the assessment of optimal treatment timing in dentofacial orthopedics. Semin Orthod. 2005;3:119-29.
- [CrossRef] [Google Scholar]
- Dentoskeletal effects and facial profile changes in young adults treated with the Herbst appliance. Angle Orthod. 1999;69:239-46.
- [Google Scholar]
- Herbst/multibracket appliance treatment of Class II division 1 malocclusions in early and late adulthood. A prospective cephalometric study of consecutively treated subjects. Eur J Orthod. 2006;28:352-60.
- [CrossRef] [PubMed] [Google Scholar]
- The mechanism of Class II correction in late Herbst treatment. Am J Orthod Dentofacial Orthop. 1997;112:87-91.
- [CrossRef] [Google Scholar]
- Skeletal effects in Class II treatment with the functional mandibular advancer (FMA) J Orofac Orthop. 2005;66:469-90.
- [CrossRef] [PubMed] [Google Scholar]
- Biomechanical effects of fixed functional appliance on craniofacial structures. Angle Orthod. 2009;79:668-75.
- [CrossRef] [PubMed] [Google Scholar]
- The headgear effect of the Herbst appliance: A cephalometric long-term study. Am J Orthod Dentofacial Orthop. 1993;103:510-20.
- [CrossRef] [Google Scholar]
- Treatment effects of the Herbst appliance. Am J Orthod Dentofacial Orthop. 1989;95:138-47.
- [CrossRef] [Google Scholar]
- Intensive treatment of severe Class II malocclusions with a headgear-Herbst appliance in the early mixed dentition. Am J Orthod. 1984;86:1-13.
- [CrossRef] [Google Scholar]
- Long-term dentoskeletal changes with the Bionator, Herbst, Twin Block, and MARA functional appliances. Angle Orthod. 2010;80:18-29.
- [CrossRef] [PubMed] [Google Scholar]
- A comparison of the MARA and the advansync functional appliances in the treatment of Class II malocclusion. Angle Orthod. 2012;82:907-14.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of advansync and intermaxillary elastics in the correction of Class II malocclusions: A retrospective clinical study. Am J Orthod Dentofacial Orthop. 2016;150:979-88.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment effects of fixed functional appliances in patients with Class II malocclusion: A systematic review and meta-analysis. Eur J Orthod. 2015;38:113-26.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of treatments with the forsus fatigue resistant device in relation to skeletal maturity: A cephalometric and magnetic resonance imaging study. Am J Orthod Dentofacial Orthop. 2011;140:616-25.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment and posttreatment effects induced by the forsus appliance: A controlled clinical study. Angle Orthod. 2014;84:1010-7.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of dentoskeletal changes accompanying the treatment of Class II malocclusion by advansync appliance versus intermaxillary coil spring mechanics. Al-Azhar Dent J Girls. 2018;5:373-83.
- [CrossRef] [Google Scholar]




