

Translate this page into:
Treating Bimaxillary Protrusion and Crowding with the Invisalign G6 First Premolar Extraction Solution and Invisalign Aligners
Address for correspondence: Dr. Ronny K. P. Lie Ken Jie, Cameron Dental Centre, 2/F, Grand Right Centre, 10 Cameron Road, Tsimshatsui, Kowloon, Hong Kong. E-mail: rogatio@gmail.com
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
In cases requiring extraction of four first premolars, ensuring maintenance of adequate posterior anchorage and proper inclination of the teeth adjacent to the extraction sites during space closure can be difficult. The Invisalign G6 first premolar extraction solution has been developed to specifically address these problems. This case report describes the treatment of a 30-year-old woman whose main concerns were related to her protrusive and malaligned anterior teeth. Clinical findings revealed, among others, bimaxillary anterior protrusion and moderate-to-severe anterior crowding. A treatment approach involving extraction of the four first premolars was chosen, followed by orthodontic treatment with the Invisalign G6 first premolar extraction solution and Invisalign aligners. At the completion of 19.5 months of aligner treatment, the patient’s anterior teeth were retracted and uprighted, resulting in an improvement in her lip profile. Normal overjet and overbite were also achieved along with alleviation of the anterior crowding. The patient was extremely happy with the treatment results.
Keywords
Bimaxillary protrusion
clear aligner treatment
crowding
incisor protrusion
Invisalign aligners
Invisalign G6 solution
orthodontic treatment
premolar extraction
space closure

Introduction
Bimaxillary protrusion and dental crowding are orthodontic problems commonly observed among Asian populations.[1,2] Treatment of these complex issues often involves extraction of the four first premolars to relieve crowding, and subsequent retraction of the maxillary and mandibular anterior teeth to close the extraction spaces. This can also improve lip protrusion and facial esthetics in these patients, which is a common concern.[1,3]
However, orthodontic treatment involving premolar extraction can present several challenges. These include maintenance of adequate posterior anchorage to avoid unwanted mesial movement of the posterior teeth,[3,4] as well as ensure root parallelism of the teeth adjacent to the extraction sites to preserve stability of the closed spaces.[5,6]
The introduction of clear and removable Invisalign aligners by Align Technology, Inc., has provided clinicians with an alternative modality of orthodontic treatment. Although initially indicated for the treatment of mild orthodontic conditions, refinement and specialization of the Invisalign System (Align Technology, Inc., San Jose, CA, USA) has allowed successful treatment of more complex orthodontic cases with Invisalign aligners.[7-9] Nevertheless, mixed outcomes have been reported with the Invisalign System in cases requiring extraction of the first premolars,[8,10,11] with the need for further treatment with a fixed appliance to correct tipping of the teeth adjacent to extraction sites being highlighted.[11,12]
To improve the clinical outcomes of patients requiring extraction of their four first premolars, Align Technology, Inc., has introduced the Invisalign G6 first premolar extraction solution.[13] Features of the system have been developed to provide maximum posterior anchorage while preventing unfavorable tipping of the canines during space closure. This ensures that the roots of the teeth adjacent to extraction sites remain parallel.[13]
This case report illustrates the successful correction of bimaxillary anterior protrusion and alleviation of crowding in a patient who underwent extraction of her four first premolars. Extraction was followed by treatment with the Invisalign G6 first premolar extraction solution (henceforth referred to as the G6 solution) and Invisalign aligners. To the best of our knowledge, this case is one of only a few to be published illustrating treatment outcomes with the Invisalign G6 solution.
Clinical Presentation and Diagnosis
A 30-year-old female patient presented with protrusive and malaligned anterior teeth, which affected her confidence and willingness to smile. Her medical and dental histories were unremarkable. The patient indicated preference for a treatment option with clear aligners for esthetic reasons. She demonstrated unsatisfactory oral hygiene.
Pretreatment facial photographs showed that the patient had balanced facial proportions and that her lips were competent at rest but protrusive [Figure 1]. Analysis of the pretreatment diagnostic records [Figure 1] revealed a bilateral Class I molar relationship and a Class II canine relationship on the right side with a Class I relationship on the left side. The patient had bimaxillary anterior protrusion with a mild overjet and overbite of 4 mm and 2.5 mm, respectively. She also showed moderate-to-severe anterior crowding in both arches (maxilla, 4.2 mm; mandible, 6.2 mm), and an anterior Bolton ratio of 74.1% was measured. In addition, she had deviated dental midlines, with the maxillary and mandibular midlines deviated by 1 mm and 2 mm to the right, respectively. Anterior crossbite of the upper right lateral incisor was also noted. The panoramic radiograph showed impacted mandibular third molars, as well as an over-erupted maxillary third molar on the right side [Figure 2]. Cephalometric analysis confirmed a normal skeletal relationship [Figure 2].

- Pretreatment extraoral and intraoral photographs
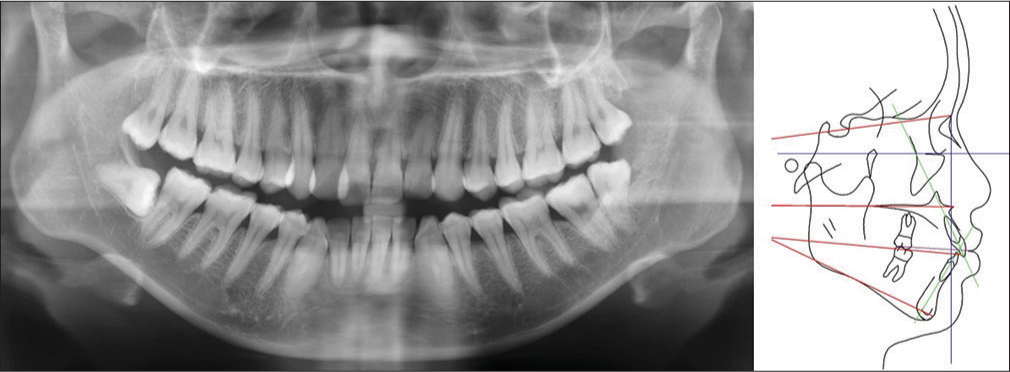
- Pretreatment panoramic radiograph (left) and lateral cephalometric tracing (right)
Treatment Objectives
The treatment objectives were to: (1) reduce the patient’s anterior protrusion to improve her lip profile, (2) achieve a normal overjet and overbite, (3) alleviate the anterior crowding, (4) maintain the bilateral Class I molar relationship, (5) achieve a Class I canine relationship on the right, (6) coordinate the deviated dental midlines with the facial midline, (7) correct crossbite of the upper right lateral incisor, and (8) align the arches.
Treatment Alternatives
The focus of treatment for this patient was to address her main concerns of protrusive and malaligned anterior teeth. A nonextraction treatment approach to relieve crowding was considered, which involved the development of a more rounded arch form with Invisalign aligners[14] and the use of judicious interproximal reduction (IPR). However, this approach would not adequately address the patient’s anterior protrusion. Thus, to enable correction of both anterior protrusion and crowding, an alternative approach involving extraction of the four first premolars, followed by treatment with the Invisalign G6 solution and Invisalign aligners, was chosen. Intermaxillary elastics were also recommended to aid in coordination of the dental arches and enhance posterior anchorage, as was IPR to help further relieve crowding and address the Bolton discrepancy. Extraction of all the third molars was also discussed; however, the patient declined to have these removed before treatment.
Treatment Progress
Before treatment, polyvinyl siloxane (PVS) impressions were taken for the development of a ClinCheck treatment plan (Align Technology, Inc., San Jose, CA, USA). This digital plan was used to determine the number of aligners needed for the patient, treatment duration and to visualize the treatment outcomes [Figure 3]. Treatment was conducted across two phases, as detailed below, and she was additionally seen at regular 6-month intervals to ensure satisfactory oral hygiene and periodontal conditions.
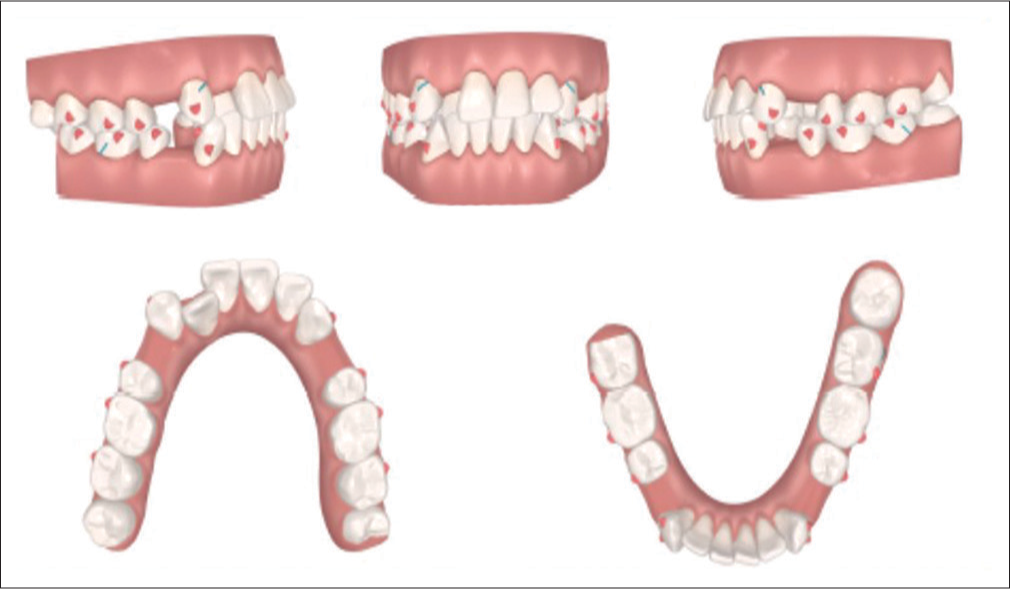
- Pretreatment ClinCheck treatment Plan
Initial Treatment Phase
Goals of the initial treatment phase were to retract the anterior teeth in the upper and lower arches for closure of the extraction spaces, alleviate the anterior crowding and align the dentition. Treatment was initiated with extraction of the four first premolars. A total of 50 sets of Invisalign aligners were used over 14 months and changed every 10 days for 8 months of treatment, and every 7 days thereafter. The patient was seen at monthly intervals. SmartForce features (specialized attachments) of the G6 solution were bonded to the teeth before commencing treatment with the second set of aligners; Optimized Retraction Attachments were used on the upper and lower canines; and Optimized Anchorage Attachments were used on the upper and lower posterior teeth [Figure 4]. Class II 3.5 oz elastics were worn full time on both sides of the dentition throughout the treatment phase [Figure 5]. IPR was carried out over the entire treatment phase in accordance with the ClinCheck treatment plan [Figure 4]. Facial and intraoral photographs taken at completion of the initial treatment phase are shown in Figure 6.
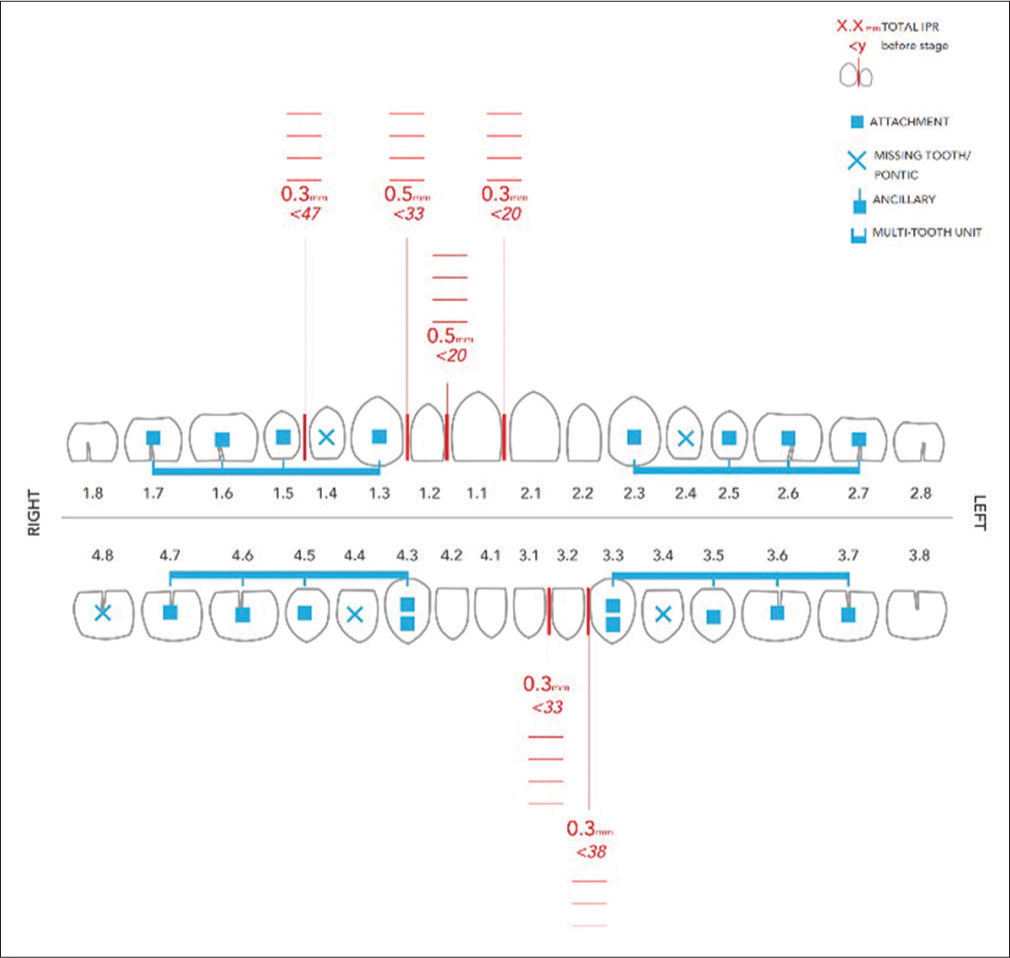
- Placement of SmartForce features (specialized attachments) of the Invisalign G6 solution and use of interproximal reduction during the initial treatment phase

- Intraoral images of the Class II elastics used during the initial treatment phase

- Extraoral and intraoral photographs following the initial treatment phase
Refinement Phase
PVS impressions were again taken to develop the refinement stage of the ClinCheck treatment plan [Figure 7]. Refinement was conducted for correction of the mild posterior open bite that developed during treatment with the final sets of aligners in the initial treatment phase [Figure 6]. Correction of the posterior open bite was performed with proper alignment of the upper right lateral incisor and closure of the residual extraction spaces in the lower arch. This allowed for retraction of the lower incisors and autorotation of the mandible. During refinement, 18 upper and 23 lower aligners were used over 5.5 months, with the aligners being changed every 7 days. Invisalign Optimized Attachments as well as conventional attachments were also used, while IPR was carried out before initiation of the aligners [Figure 8]. The patient’s progress was reviewed monthly and refinement was followed by nightly retention.

- Refinement stage: ClinCheck treatment plan

- Placement of SmartForce features (specialized attachments) of the Invisalign G6 solution and use of interproximal reduction during the refinement phase
Retention
Vivera retainers for the upper and lower arches are currently worn nightly by the patient. The minimal residual posterior open bite observed following the refinement phase is expected to be fully corrected during retention, given that the teeth can settle within the Vivera retainers, which were fabricated based on the last aligner stage. Retention is expected to be life-long so as to minimize the risk of relapse.
Treatment Results
Posttreatment records show that all treatment objectives were achieved with good esthetic and occlusal results [Figures 9 and 10]. At the completion of treatment, the patient’s incisors were retracted and uprighted, improving her lip profile and facial esthetics [Figure 11 and Table 1].
| Measurement | Pretreatment | Posttreatment | Norm±SD |
|---|---|---|---|
| NSBa (°) | 132 | 132 | 130±4.5 |
| SNA (°) | 81.7 | 81.5 | 82±3.5 |
| SNB (°) | 79.2 | 78.7 | 79±3 |
| ANB (°) | 2.5 | 2.8 | 3±2 |
| SNPg (°) | 78 | 77 | 81±3.5 |
| SN/MnPl (°) | 35.2 | 34.6 | 34±4.5 |
| SN/MxPl (°) | 7 | 12 | 8±3 |
| MxPl/MnPl (°) | 25.2 | 22.6 | 26±5 |
| UI/MnPl (°) | 116 | 106 | 118±6 |
| LI/MnPl (°) | 93.5 | 90.8 | 97±7 |
| UI/LI (°) | 122.7 | 138.9 | 115±8 |
| Li to Apo (mm) | 7.4 | 4.5 | 5.5±2.8 |
| UFH (%) | 46.7 | 48.9 | 54.2 |
| LFH (%) | 59.1 | 57.5 | 65.2 |
| Upper lip to E-plane (mm) | 1.5 | 0 | 3±2.5 |
| Lower lip to E-plane (mm) | 4.3 | 2.5 | 4±2.5 |
| Wits appraisal (mm) | −7.4 | −2.7 | 4.5±3 |
SD – Standard deviation

- Posttreatment extraoral and intraoral photographs

- Posttreatment panoramic radiograph (left) and lateral cephalometric tracing (right)

- Superimposed tracings of the pretreatment and posttreatment lateral cephalometric radiographs
Normal overjet and overbite were also achieved. The anterior crowding was corrected through staged movement of the teeth during their alignment and the use of IPR, while a proper occlusal relationship was also established. The bilateral Class I molar relationship was maintained, and a Class I canine relationship was achieved on the right. In addition, the upper and lower dental midlines were coincident with the facial midline. Overall, good alignment, angulation, and inclination of the dentition were achieved.
As confirmed by relative positions of the canines, second premolars and molars before, and after treatment, good root parallelism and adequate posterior anchorage were maintained with SmartForce features of the Invisalign G6 solution [Figure 11]. The patient was highly motivated and compliant in wearing her aligners and elastics. She was extremely happy with the treatment results and reported being comfortable while using the Invisalign System. Arrangements will be made in the future for extraction of all the third molars.
Discussion
Extraction of the four first premolars is often conducted to correct bimaxillary protrusion and crowding in patients with Class I malocclusions.[15] In a retrospective study of 542 patients with Class I skeletal and dental malocclusions, approximately one-fourth of the patients were observed to have had their four first premolars extracted as part of their treatment.[15] The study also showed that severity of the upper and lower crowding, lower lip to E-plane, and overjet were the four significant factors contributing toward a decision to extract the premolars.[15]
The patient described in this case had, among other issues, bimaxillary anterior protrusion and moderate-to-severe anterior crowding. To address these issues together, extraction of her four first premolars was decided upon, followed by treatment with the Invisalign G6 solution and Invisalign aligners.
One of the concerns in premolar extraction cases involves maintaining root parallelism of the teeth adjacent to the extraction spaces during space closure.[5,6] Use of the Invisalign G6 solution in this case aided timely staged movement of the anterior teeth, resulting in translation of the canines without any unwanted tipping. Another advantage of staged movement of teeth is that it allows for better aligner fit by increasing the predictability of teeth movement.
An additional concern in premolar extraction cases involves the maintenance of adequate posterior anchorage during space closure.[3,4] Treatment with the G6 solution was chosen as its specialized features have been developed to ensure maximum posterior anchorage.[13] Class II elastics were also used throughout the initial treatment phase to enhance posterior anchorage, to minimize mesial tipping of the posterior teeth, and to avoid unwanted “bowing effects” on the occlusal plane. Undesirable effects of Class II elastics include extrusion of the maxillary incisors and mandibular molars;[16] however, the Invisalign aligners were able to counteract this by simultaneously intruding the upper anterior teeth while retracting them. Similarly, the lower aligners offset the extrusive effects of the elastics on the molars.
The patient in this case was eager to undergo treatment with clear aligners for esthetic reasons; thus, the Invisalign System was chosen for alignment of the dentition. In addition to esthetics, clear and removable aligners offer several advantages over fixed appliances, including comfort and simplicity of care.[12]
Patient compliance in aligner wear and timely recall are the two key factors contributing toward successful treatment outcomes when undergoing treatment with clear and removable aligners. A 10-day aligner change protocol was used for the first 8 months, followed by a 7-day change protocol until treatment completion (14 months). Invisalign SmartTrack aligner material and SmartForce features are engineered to express optimal programmed tooth movement with weekly aligner change.[13] More frequent aligner change may allow for clinical results to be obtained sooner by avoiding excessive lag phase and expression of movement from new aligners and holds potential to enhance patient compliance and motivation during lengthy treatments.[13,17] As exemplified during monthly follow-up checks, the patient was highly motivated and compliant in her aligner wear.
All treatment objectives were met at the completion of treatment, including improvement in the patient’s lip profile and correction of the anterior crowding. However, challenges were encountered during the treatment process. Despite the patient’s compliance in her aligner and elastic wear, a mild degree of posterior open bite was observed at the end of the initial treatment phase. The posterior open bite arose mainly due to the inability to fully align the instanding upper right lateral incisor, resulting in premature contact on closing. In retrospect, closer monitoring of the incisor during its labial movement, as well as timely relief of tight interproximal contacts with light abrasive strips to aid in tooth movement, may have helped to obtain a more favorable initial treatment outcome.
The patient is currently undergoing retention with Vivera retainers, which is expected to continue for a prolonged period. To date, no relapse or negative effects of the extractions have been observed.
Conclusion
This case demonstrates that the Invisalign G6 solution, when used after premolar extraction, is effective in the correction of bimaxillary anterior protrusion and crowding. At the completion of treatment, the patient’s lip profile had been improved and the crowding of her teeth was corrected.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that her name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Acknowledgements
Editorial assistance in the preparation of this manuscript was provided by Priya Shreedhar and Katie Qi of MediTech Media Asia Pacific and funded by Align Technology, Inc.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Bimaxillary protrusion: An overview of the surgical-orthodontic treatment. Semin Plast Surg. 2009;23:32-9.
- [Google Scholar]
- Current status of orthodontic Professionals in the Asian Pacific region. APOS Trends Orthod. 2016;6:58-77.
- [CrossRef] [Google Scholar]
- First or second premolar extraction effects on facial vertical dimension. Angle Orthod. 2005;75:177-82.
- [Google Scholar]
- Efficacy of intraarch mechanics using differential moments for achieving anchorage control in extraction cases. Am J Orthod Dentofacial Orthop. 1997;112:441-8.
- [Google Scholar]
- A radiographic study of roots in extraction sites. Angle Orthod. 1976;46:64-8.
- [CrossRef] [Google Scholar]
- Root parallelism of canine and second premolar in pre-adjusted and standard edgewise systems: A comparative study. GMJ. 2014;3:176-81.
- [Google Scholar]
- Management of overbite with the invisalign appliance. Am J Orthod Dentofacial Orthop. 2017;151:691-900.
- [Google Scholar]
- Four-premolar extraction treatment with invisalign. J Clin Orthod. 2006;40:493-500.
- [CrossRef] [Google Scholar]
- Esthetic orthodontic treatment using the invisalign appliance for moderate to complex malocclusions. J Dent Educ. 2008;72:948-67.
- [Google Scholar]
- A premolar extraction case using the invisalign system. J Orofac Orthop. 2006;67:385-94.
- [CrossRef] [PubMed] [Google Scholar]
- Activation time and material stiffness of sequential removable orthodontic appliances. Part 3: Premolar extraction patients. Am J Orthod Dentofacial Orthop. 2008;133:837-45.
- [Google Scholar]
- Invisalign G6. Available from: http://www.invisalign-g6.com/en-XA. [Last accessed on 2018 Feb 20]
- [Google Scholar]
- The predictability of transverse changes with invisalign. Angle Orthod. 2017;87:19-24.
- [CrossRef] [Google Scholar]
- Extraction decision and identification of treatment predictors in class I malocclusions. Prog Orthod. 2013;14:47.
- [Google Scholar]
- Correction of class II malocclusion with class II elastics: A systematic review. Am J Orthod Dentofacial Orthop. 2013;143:383-92.
- [Google Scholar]
- Changes in force associated with the amount of aligner activation and lingual bodily movement of the maxillary central incisor. Korean J Orthod. 2016;46:65-72.
- [CrossRef] [Google Scholar]




