

Translate this page into:
Treatment of severe skeletal Class III patient with buccally impacted canines and severe crowding using a bone-anchored facemask and Alt-RAMEC protocol: A case report

*Corresponding author: Hasan Sabah Al-Nuaimi, Department of Pediatrics Dentistry and Orthodontics, Faculty of Dentistry, University of Malaya, Kuala Lumpur, Malaysia. hsh.ortho@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Al-Nuaimi HS, Radzi ZB, Venugopal A. Treatment of severe skeletal Class III patient with buccally impacted canines and severe crowding using a bone-anchored facemask and AltRAMEC protocol: A case report. APOS Trends Orthod. doi: 10.25259/APOS_264_2024
Abstract
A 14-year-10-month-old female patient presented with a chief complaint of being dissatisfied with the looks of her teeth and face. She had a pronounced misalignment of her dentition, defined by a Class III skeletal relationship and an average vertical proportion of the face. The patient had an anterior crossbite and bilateral posterior crossbites, with the upper left canine impacted in a buccal position. After a comprehensive consultation with the patient and her parents, we decided to implement a treatment strategy that entailed utilizing a maxillary bone borne expander in conjunction with a facemask. This treatment followed a protocol that consisted of alternating between rapidly expanding and contracting the maxilla. The purpose of this was to stimulate the advancement of the midface. After the treatment was carried out to treat the crossbites, a fixed appliance (MBT prescription) was bonded on the maxillary and mandibular arches. In addition, four premolars were extracted, and the upper left canine was brought to occlusion. Temporary anchorage devices were used in the lower arch to provide skeletal anchorage. The patient underwent active treatment for a period of 24 months following which we were able to achieve satisfactory occlusal and esthetic results.
Keywords
MARPE
Maxillary skeletal expander
Facemask
Skeletal expander
Temporary anchorage devices
Class III
Expansion

INTRODUCTION
The necessity of treating Class III malocclusions at an early age has long been a topic of discussion. A highly discussed topic in orthodontic literature focuses on transverse anomalies of the jaw in a developing child.[1,2] The literature supports early facemask therapy for maxillary protraction before the age of ten, either with or without rapid palatal expansion.[3] However, the timing of treatment is crucial for achieving the best skeletal maxillary expansion outcomes.[4] The unpredictable nature of mandibular growth has also caused controversy and could potentially compromise the efficacy of early treatment.[1,5] With the help of rapid maxillary expansion appliances like miniscrew-assisted rapid palatal expander (MARPE), it has been possible to address the issue of early treatment of skeletal Class III due to maxillary retrognathia. Positive results have been reported when using bone-borne appliances for facemask traction instead of tooth-borne appliances.[6]
Class III malocclusion is common, especially in Asian countries, and affects around 1% of the population in North America. The etiology of Class III malocclusion is complex and includes both hereditary and environmental factors, including maxillary retrusion (25%), mandibular prognathism (20%) and, a combination (22%).[7,8]
Based on the principle of separating and remodeling the mid-palatal suture and circum-maxillary sutures, early treatment with a rapid maxillary expander (RME) and face mask is the most effective way to correct the anteroposterior and transverse relationship in a growing patient.[9] However, compared to the forces needed to move teeth, the force needed to separate the mid-palatal suture is roughly 900–4500 g, which is relatively high.[10] There are several drawbacks when palatal expansion is performed only using tooth borne anchorage. Some of them include sub-optimal dental-periodontal integrity of anchor teeth, mandibular rotation in a clockwise direction, relapse, and tipping of anchor teeth buccally as the palatal cusps of the posterior teeth extrude.[9,11,12]
A MARPE was proposed by Lee et al.[13] to maximize skeletal expansion and minimize undesired dento-alveolar consequences. The force distribution in hybrid devices is significantly better than in devices that use dental anchorage alone, as shown by Seong et al.[14] By utilizing these techniques, the therapeutic indications for surgically assisted rapid palatal expansion appear to be somewhat reduced, which, in turn, lowers the operational risk related to this kind of surgery.[9,14] When using the Alternate Rapid Maxillary Expansion and Constriction (Alt-RAMEC) protocol, which was introduced by Liou and Tsai, face mask therapy applied to MARPE-based appliances also demonstrates fewer adverse effects and a more efficient distribution of forces over the nasomaxillary complex.[15-17] This is because the protocol allows for sutural mobilization with repeated opening and closing of the screw for 7 to 9 consecutive weeks without actual expansion. This enhances the maxilla’s mobilization in relation to the surrounding sutures.[15]
A 14-year-10-month-old female with maxillary retrusion and maxillary transverse deficiency and a Class III relationship is presented in this paper. In addition to treatment with a fixed appliance to correct the dentition, she had facemask therapy in conjunction with maxillary skeletal expansion.
CASE REPORT
A 14-year-10-month old female presented to the clinic with a chief complaint, “I do not like how my teeth and face look.” The patient was regular with her routine dental visits but with fair oral hygiene. She described that her mother had the same “jaw shape” as one of her cousins from her mother’s side. Simple occlusal caries were evident in the posterior teeth in the upper and lower jaws. No signs or symptoms of temporomandibular disorders were observed. A Class III incisor relationship over a severe skeletal Class III base due to maxillary retrognathia with average vertical proportion and maxillary constriction was evident. The upper arch showed severe crowding (16 mm), while the lower arch showed mild crowding (4 mm) with reverse overjet (5 mm) and overbite (7 mm). The upper midline was shifted 1 mm to the right side of the facial midline with an anterior and posterior bilateral crossbite. The upper right canine was in a Class III half-unit relationship, while the left upper canine was buccally impacted, and the molars were in Class III full-unit relationships on both sides. The profile was concave with competent lips and increased nasolabial angle [Figure 1; Table 1].
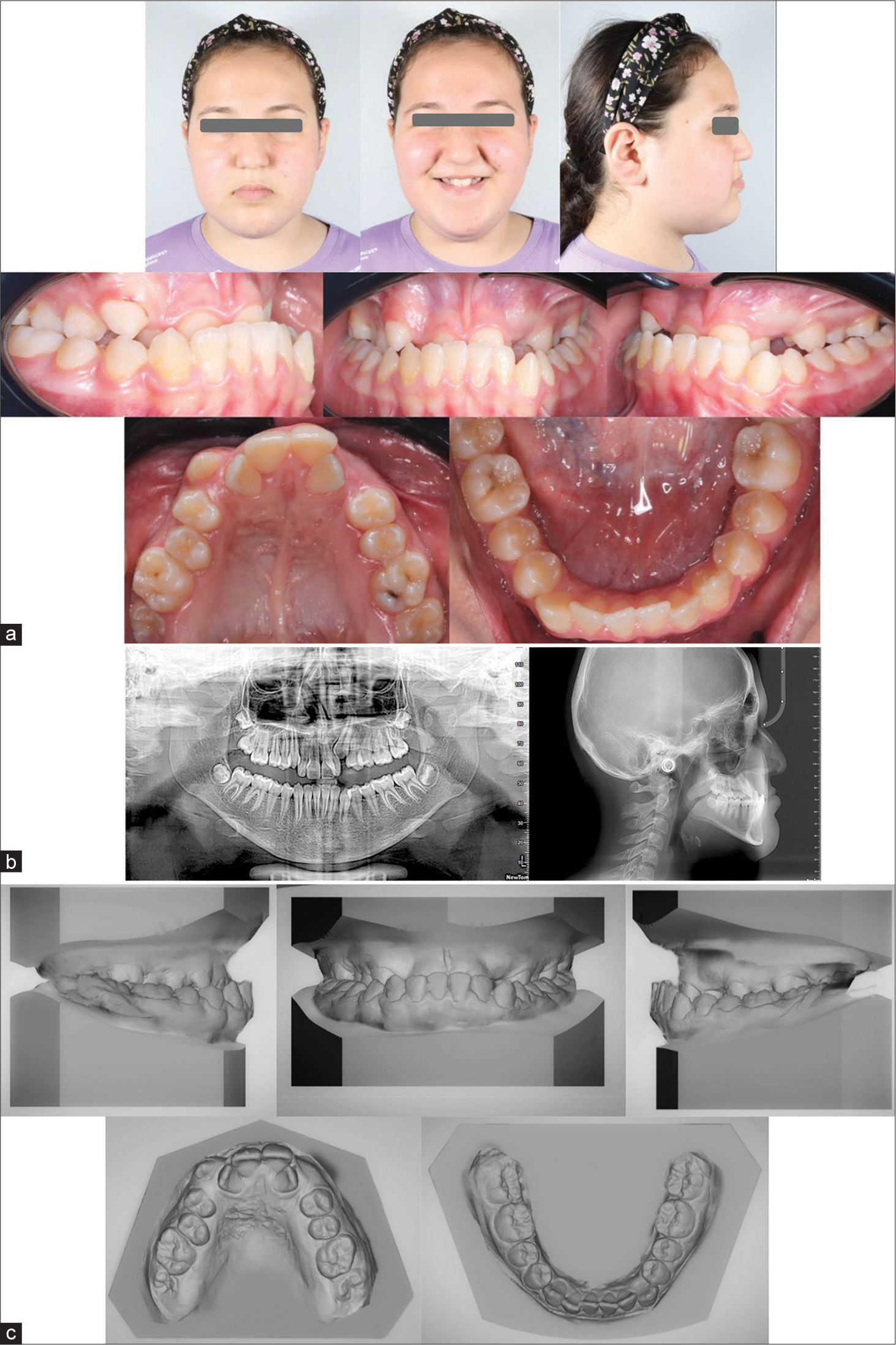
- Shows (a) Pre-treatment extra and intra-oral photograph; (b) Pre-treatment radiography (O.P.G) and Cephalometric analysis (T1); (c) Pre-treatment models.
| Variable | *Norms | T1 |
|---|---|---|
| SNA | 81±3° | 72.4° |
| SNB | 78±3° | 80.6° |
| ANB | 3±2° | −8.2° |
| MMPA | 27±5° | 24° |
| Face height ratio | 55%±2%° | 52% |
| SN to maxillary plane | 8±3° | 7° |
| Upper incisor to maxillary plane | 109±6° | 118° |
| Lower incisor to mandibular plane | 93±6° | 86° |
| Interincisal angle | 135±10° | 137° |
| Wits appraisal | 0–1mm | 10mm |
| Lower incisor to APo line | 1±2mm | 9mm |
| Upper lip to E-line | −3±2mm | −4mm |
| Lower lip to E-line | −1 mm±2mm | +3mm |
| Nasolabial angle | 100±10° | 100° |
Treatment plan and treatment objectives
The primary objectives of this treatment were as follows:
To improve the antero-posterior positioning of her upper jaw and encourage a clockwise rotation of her lower jaw
Achieve a proper overbite and overjet, eliminate the transverse deficiency, establish a Class I canine relationship, and, if possible, achieve overcorrection
Enhance maxillary incisor visibility and restore the natural curvature of the smile
To achieve these objectives, we proposed the implementation of the following treatment strategy: Referring the patient for scaling, polishing, and promoting the attainment and maintenance of appropriate oral hygiene. Subsequently, the patient was referred to a restorative dentist for further examinations and treatment. The treatment consisted of two steps. A bone-anchored facemask was employed as the initial approach to address skeletal anteroposterior and transverse discrepancies in conjunction with the Alt-RAMEC protocol. The second phase of therapy lasted for 24 months and focused on correcting dentoalveolar discrepancies, which included issues such as crowding, canine impaction, and incisor inclination. The extraction pattern involving the upper and lower first premolars was decided on with the usage of skeletal anchorage to close spaces.
Treatment alternatives
Opting to wait until growth was complete was considered as an alternative treatment approach. In this case, the surgical procedures would include a Le Fort I osteotomy for expansion, followed by maxillary advancement and rotation of the maxilla to correct the occlusal plane. In addition, mandibular setback surgery might be necessary to address mandibular prognathism. It was concluded that these procedures would be very effective in achieving a stable and esthetically pleasing facial result, addressing both dental and skeletal concerns.
The patient and her parents wanted to explore non-surgical treatment options. Before beginning treatment, they were thoroughly informed of all potential risks and adverse effects, with a clear understanding that surgical intervention might still be necessary if significant mandibular growth continued after treatment.
After careful consideration, the patient chose the current non-surgical treatment plan to complete her treatment before her university graduation.
Treatment progress
Bands were placed on the maxillary first molars, and a pickup impression was taken in order to fabricate a maxillary skeletal expander (Biomaterials Korea Inc., Seoul, South Korea). Following the cementation of the skeletal expander to the maxillary first molars, four mini-screws (1.5 × 11 mm, ACR screws, Biomaterials Korea Inc.) were inserted with the help of cone-beam computed tomography visuals. For the 1st week, the rate of expansion was 0.5 mm each day. We modified the Alt-RAMEC procedure to aid in the loosening of the circum-maxillary sutures. For 8 weeks, at a rate of (0.5 mm/day), we alternated between 1 week of constriction and 1 week of expansion. Following a week of midline diastema observation, the activation rate was adjusted to 0.25 mm/day for an additional 2 weeks. A facemask (Orthotechnologes-USA) was fastened to the hooks of the palatal expander using forces of 450 g/side using extraoral elastics (16 oz, Dentaurum, Germany). In 2 weeks, without the use of any fixed appliance, a positive overjet was seen, and the diastema gradually closed on its own [Figure 2].
![Shows (a) intraoral and extraoral changes after using a facemask with (MARPE) appliance; (b) radiographical transverse changes (Occlusal radiography) after maxillary expansion; (c) cephalometric radiographic anteroposterior skeletal and incisor inclination changes after facemask therapy; (d) superimposition after facemask therapy [Black line: before treatment; Red line: after treatment].](/content/9/2024/0/1/img/APOS-264-2024-g002.png)
- Shows (a) intraoral and extraoral changes after using a facemask with (MARPE) appliance; (b) radiographical transverse changes (Occlusal radiography) after maxillary expansion; (c) cephalometric radiographic anteroposterior skeletal and incisor inclination changes after facemask therapy; (d) superimposition after facemask therapy [Black line: before treatment; Red line: after treatment].
Fixed appliances (0.022 × 0.028”) were placed in the 10th month of treatment, along with the extraction of the upper and lower first premolars. By gradually progressing through a series of nickel-titanium archwires, leveling and alignment were carried out until the curve of Spee was flat in both arches. Lace-back mechanics in the lower anterior segment were used to reduce round-tripping. The upper left canine was disimpacted utilizing an open flap technique, tractioned by a power chain in an uncontrolled tipping action. The probability of relapse of achieved expansion during the fixed appliance stage is reduced by the use of a modified transpalatal arch that was fixed onto two temporary anchorage devices (TADs) (Tomas, Dentaurum, Germany) in the palate.
For the en mass retraction of the lower anterior segment, two TADs (1.6 × 8 mm, Dentaurum-Tomas, Germany) were positioned between the lower second premolar and first molar. The crimpable hooks were longer than the position of the head of the TADs. This created a force vector that resulted in labial tipping of the lower anterior segment while being retracted into the extraction space. This was beneficial, as initially, the lower incisors were lingually tipped and retraction usually tends to worsen the lingual tipping due to torque loss secondary to increased play within the bracket slot-wire interface. To achieve maximum intercuspation, box elastics were used [Figure 3].
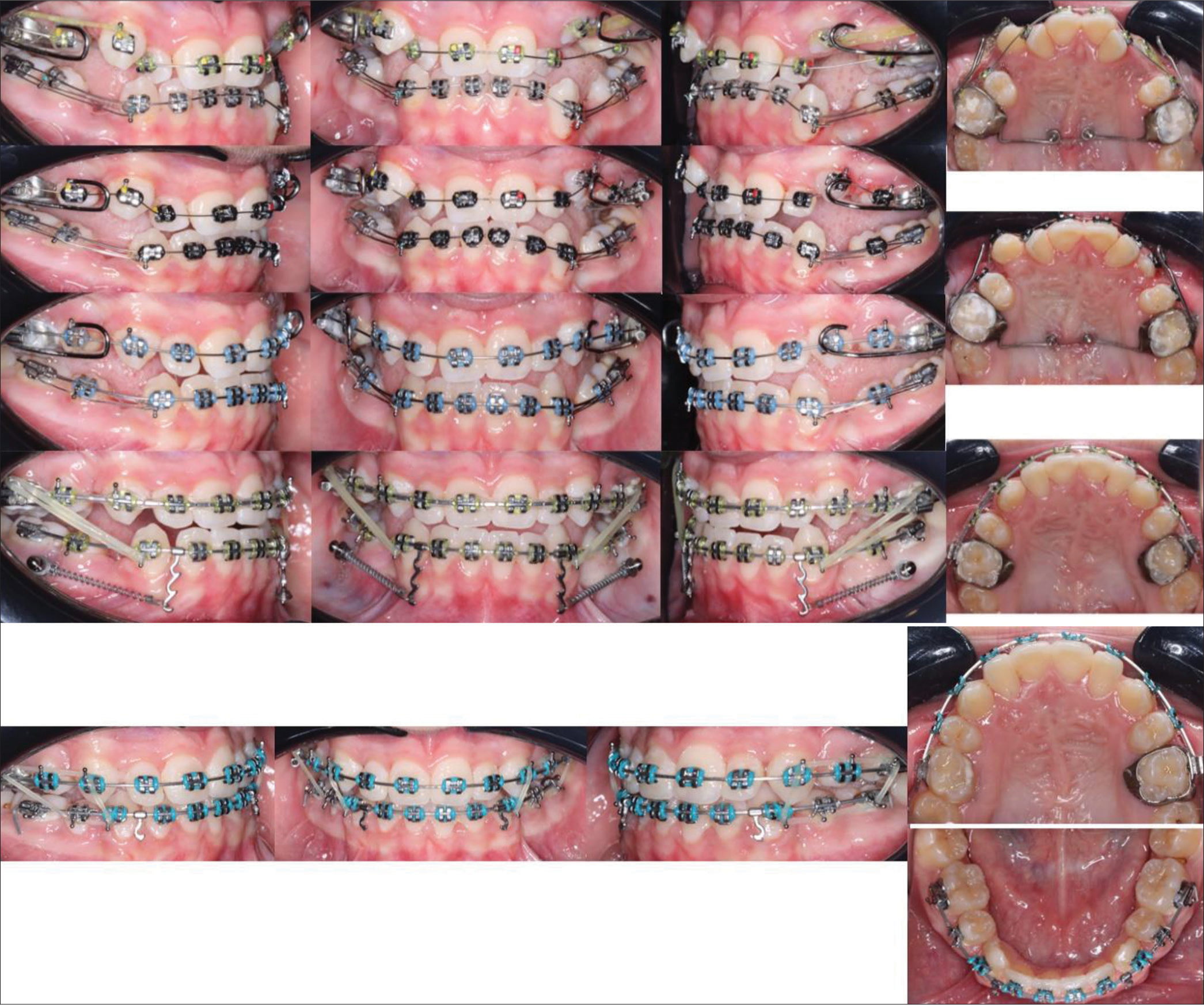
- Mid treatment (mechanics) intra oral pictures with fixed appliances.
RESULTS
The anterior and transverse crossbites were effectively corrected by the use of the MARPE, facemask treatment, and fixed appliances, which lasted for 24 months. Class I canine relationship on both sides was achieved at the end of treatment. On comparing the photographs taken before and after the treatment, it was clear that the patient’s lateral profile had seen a noticeable improvement, transitioning from a concave to a straight profile [Figures 4 and 5]. When the cephalometric tracings were superimposed, it was observed that the maxillary segment showed a slight shift anteriorly and inferiorly. The treatment led to a backward rotation of the mandible, causing an increase in the mandibular plane angle. The position of the maxillary molars remained mainly unchanged at the beginning and end of the face mask therapy [Figure 2, Table 2]. The lower incisors were retracted and labially tipped. After undergoing 2 years of treatment, the fixed appliance was removed, and a fixed lingual retainer along with vacuum formed retainer was provided for the upper and lower arches. The patient was instructed to wear the retainer every night to avoid any relapses or changes in occlusion [Figure 6]. Although the girl’s mandibular growth potential was still unknown and required continual monitoring, both the patient and her parents expressed satisfaction with the results. After a 3-year follow-up, it is evident that the outcome remained stable [Figure 7].
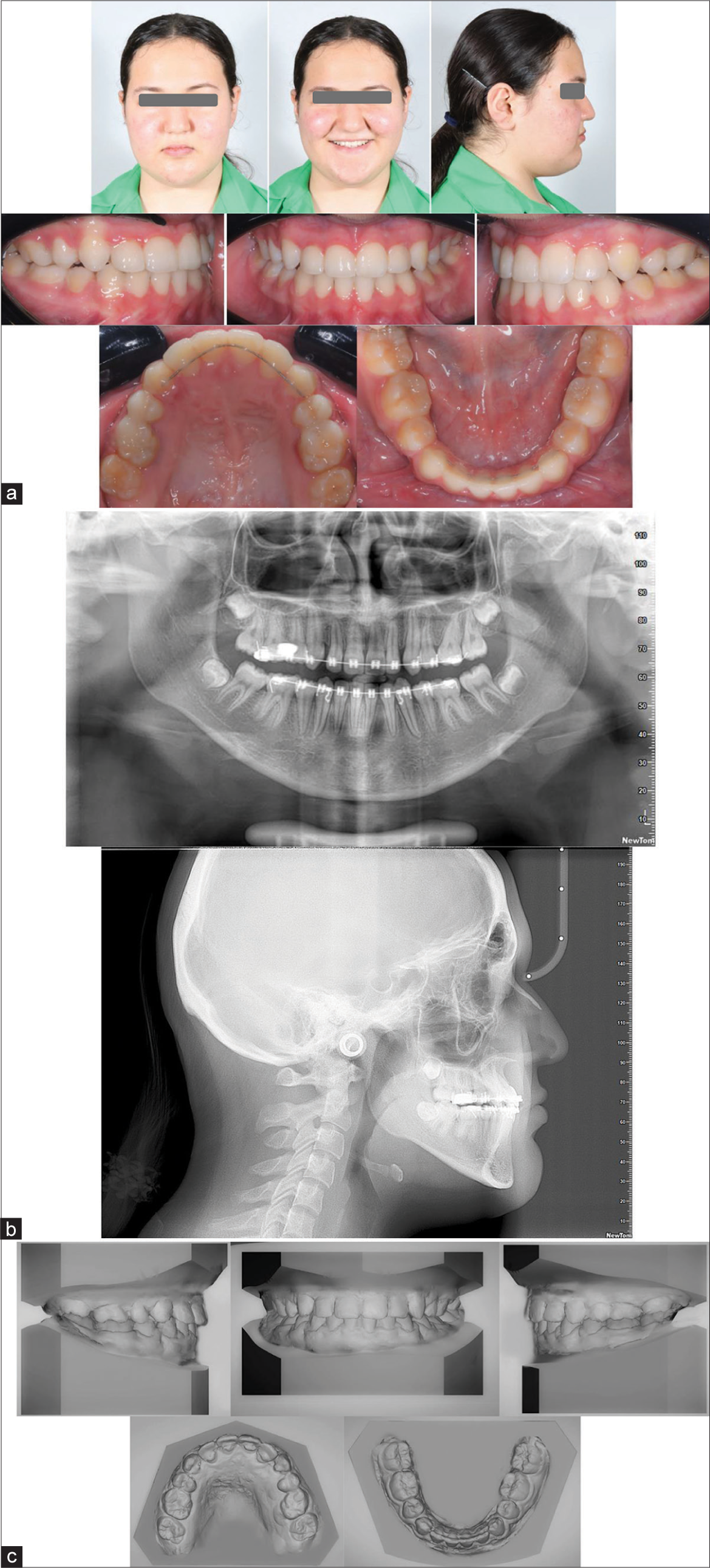
- Show (a) Post-treatment extra and intra-oral photography; (b) Post-treatment radiograph (O.P.G. and cephalogram), pre-treatment (T1) and post-treatment (T2) cephalometric measurements; (c) Post-treatment models.
![Cephalometric superimposition [black line: before treatment; Red line: after tretment]: (a) General superimposition over Sella-Nasion plane; (b) Maxillary superimposition; (c) Mandibular superimposition.](/content/9/2024/0/1/img/APOS-264-2024-g005.png)
- Cephalometric superimposition [black line: before treatment; Red line: after tretment]: (a) General superimposition over Sella-Nasion plane; (b) Maxillary superimposition; (c) Mandibular superimposition.

- Retention protocol used double fused vacuum formed retainer with upper and lower fixed lingual retainers.

- Three years retention follow-up.
| Variable | T1 | T2 |
|---|---|---|
| SNA | 72.4° | 79.2° |
| SNB | 80.6° | 80° |
| ANB | −8.2° | −0.8° |
| MMPA | 27° | 28° |
| Face height ratio | 52% | 54% |
| SN to maxillary plane | 7° | 9° |
| Upper incisor to maxillary plane | 118° | 116° |
| Lower incisor to mandibular plane | 86° | 90° |
| Interincisal angle | 137° | 138° |
| Wits appraisal | 10 mm | 2 mm |
| Lower incisor to Apo line | 9 mm | 3 mm |
| Upper lip to E-line | −4 mm | −3 |
| Lower lip to E-line | +3 | −1 |
| Nasolabial angle | 100° | 105° |
SNA: Sella-Nasion-point A; SNB: Sella-Nasion-point B; ANB: point A-Nasion-point B; MMPA: Maxillomandibular plane angle
DISCUSSION
Multiple studies have demonstrated the need for timely treatment in patients with Class III maloccliusions.[1,2,7,9] To induce maxillary skeletal protraction and redirect mandibular growth in a downward and backward trajectory, we chose to employ a facemask therapy.[17-19] Maxillary protraction is recommended for patients who have a deficiency in the upper jaw and a skeletal Class III malocclusion in their mixed dentiton phase. For the majority of adult individuals with Class III malocclusion and midface deficiency, an orthodontic-surgical treatment or camouflage is the most often suggested alternative.[4,7]
Combining a facemask with RME is expected to stimulate the midfacial sutures into some form of distraction, leading to an improved protraction response.[3] Class III correction while wearing a conventional facemask also carries the risk of complications. The forces required for maxillary protraction frequently operate on the maxillary anchor teeth. As a result, the upper teeth migrate anteriorly. This might result in significant anterior crowding or space loss, which would make orthopedic treatment less effective.[9]
To achieve substantial treatment results, it is recommended to initiate facemask treatment when the individual is at least 10 years old. The concurrent expansion of the palate can potentially amplify the skeletal effects of the facemask.[4,20,21] The question of whether facemasks with and without RME have significant differences in correcting the sagittal position of the maxilla is still a subject of controversy. Liou and Tsai proposed an alternative technique, known as Alt-RAMEC, for the disarticulation of the maxilla with the aim of promoting maxillary growth.[22] Recent clinical trials and systematic reviews have confirmed the effectiveness of the Alt-RAMEC strategy in increasing maxillary growth when used in combination with RME and facemask treatment.[22,23]
The predicted range for maxillary protraction is typically between 2 and 4 mm.[24,25] However, Liou and Tsai[16] found that the Alt-RAMEC regimen resulted in more sagittal gain when applied along with facemask treatment. The exact degree of maxillary skeletal protraction remains uncertain when treatment is provided after this age, as these case reports focused solely on interventions during pre-adolescence. The case study by Wilmes et al.[26] demonstrated that the hybrid hyrax, when combined with the Alt-RAMEC protocol, resulted in a 7 mm improvement in the Wits assessment without any negative effects on the dentition. Recent case reports on the use of bone-anchored facemasks have consistently shown positive skeletal outcomes with few dental changes.[23]
In their research, Ngan et al.[23] compared the outcomes of RME combined with facemask therapy in patients using both tooth-anchored and bone-anchored approaches. They observed that the group with tooth-anchored facemasks experienced a more pronounced forward shift of the incisors, improved molar relationship, and a decrease in overjet. Conversely, the bone-anchored facemask group showed minimal alteration in the vertical dimension. While the findings indicated a decrease in dental complications, the study was limited to participants in the pre-adolescent age range.
Unlike other bone expansion devices, the appliance planned for this patient was placed further back and closer to the center of resistance of the maxilla. In addition, to facilitate the parallel expansion, the screws were firmly inserted through both cortices.[27]
MARPE can disarticulate the pterygopalatine and circummaxillary sutures during maxillary expansion. The zygomaticomaxillary complex rotates around a center of rotation located near the proximal aspect of the zygomatic process of the temporal bone.[27] This technique can result in spontaneous maxillary advancement, reduction of reverse overjet, and mandibular backward rotation, making it effective for correcting Class III malocclusions in the sagittal plane.[28] In addition, significant soft-tissue changes occur in the nasal region, with the nose tending to widen, move forward, and shift downward. Combining intermaxillary elastics with skeletal anchorage post-MARPE expansion may prove to be an alternative approach for treating non-growing patients with skeletal Class III malocclusion.[29]
Unlike the strategy used by Liu et al.,[22] we adjusted the level of activation to be approximately 0.5 mm each day. This was done to mitigate the risk of bone anchor loosening caused by stress concentration. Regarding the treatment outcome, the overall superimposition revealed that there was an anterior positioning of her point A [Figure 2]. Furthermore, the analysis of regional superimposition revealed no significant molar extrusion, although there was some buccal tipping of molars. There was no incisor proclination observed following the treatment. These undesirable effects, commonly observed in maxillary protraction using a facemask with conventional RME, were greatly diminished.[30-32] To provide more conclusive evidence of this intervention, further clinical research must be conducted.
In our case, the inter-molar width expansion measured 6 mm, inter-premolar width was 5 mm. The skeletal expansion accounted for about 65% of the expansion, which is about the same as reported in the previous studies.[33]
Two factors that are predictive of positive long-term results from Class III early treatment are overcorrection of overjet and overbite and proper vertical dentoalveolar control to avoid an undesirable clockwise rotation of the mandible.[34,35] In our case, since the patient was normodivergent, it was beneficial to gain some clockwise rotation of the mandible for Class III correction.
Sugawara et al.[34] noted that the predominant mandibular growth in both groups took place before the age of fifteen. This was achieved by tracking a group of sixty-three Class III patients who were getting chin cup treatment and conducting a comparative analysis with untreated children of various ages. Mandibular growth in Class III patients exhibited significant variability, with some individuals experiencing growth that continued until the post-pubertal stage. During a 10-year study, Wells et al.[32] found that 25–30% of participants experienced relapse. In contrast, Mitani et al.[35] found no discernible differences in the rate of growth between the Class III and control groups during their investigation of post-pubertal mandibular growth. It may be inferred that, notwithstanding the possibility of a few exceptional cases, the growth of the mandible in Class III patients is generally similar to that in controls. The patient’s skeletal maturation stage was cervical vertebral maturation stage (CVMS) 3 before treatment and CVMS 4 after treatment, indicating that our intervention occurred during a period of rapid growth toward the postpubertal stage.[36] Therefore, after undergoing treatment, it is expected that there will be some residual growth of the mandible. The current treatment resulted in notable alterations to the facial profile and facial convexity angle. Surprisingly, the proclination of the front teeth was restricted, and the first molar in the upper jaw remained almost in its original location. The maxillary incisors were not affected much by the extraction of the maxillary first premolars due to the fact that all the space was utilized for correction of crowding and disimpaction of the maxillary canine. The smile arc and tooth show exhibited improvement when compared to pre-treatment photos. To cultivate the patient-provider relationship and instill trust, alleviate apprehension, and promote favorable behavior, as well as offer solace to the patient and her parents, it was imperative to prioritize pain avoidance and management throughout and following the procedures.[37]
CONCLUSION
Utilizing a maxillary bone expander (MARPE) with AltRAMEC activation protocol along with facemask protraction successfully enhanced the facial profile in a 14-year-10-month patient, as shown by the obvious maxillary protraction and expansion. Nevertheless, due to the patient’s age and the possibility of latent mandibular growth, it is crucial to regularly monitor long-term stability.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm the use of AI for assisting with writing the manuscript, but no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Developing class III malocclusions: Challenges and solutions. Clin Cosmet Investig Dent. 2018;10:99-116.
- [CrossRef] [PubMed] [Google Scholar]
- Importance of orthodontic intervention of the class III malocclusion in mixed dentition. Dental Press J Orthod. 2020;25:57-65.
- [CrossRef] [PubMed] [Google Scholar]
- Early treatment of class III malocclusion with facemask therapy. Clin Exp Dent Res. 2018;4:279-283.
- [CrossRef] [PubMed] [Google Scholar]
- The effects of maxillary protraction with or without rapid maxillary expansion and age factors in treating class III malocclusion: A meta-analysis. PLoS One. 2015;10:e0130096.
- [CrossRef] [PubMed] [Google Scholar]
- Difference in using protrusion face mask before or after rapid palatal expansion in skeletal class III Children: A preliminary study. Children (Basel). 2022;9:1535.
- [CrossRef] [PubMed] [Google Scholar]
- Management of class III malocclusion and maxillary transverse deficiency with Microimplant-assisted Rapid Palatal Expansion (MARPE): A case report. Medicina (Kaunas). 2022;58:1052.
- [CrossRef] [PubMed] [Google Scholar]
- TAD driven class III camouflage: Eight point protocol to optimize efficiency, aesthetics and stability. Semin Orthod. 2022;28:164-94.
- [CrossRef] [Google Scholar]
- Maxillary protraction using skeletal anchorage and intermaxillary elastics in skeletal class III patients. Korean J Orthod. 2015;45:95-101.
- [CrossRef] [PubMed] [Google Scholar]
- A clinician's perspective on indications and failures of bone-borne maxillary expanders. Semin Orthod 2023
- [CrossRef] [Google Scholar]
- Prediction of rapid maxillary expansion by assessing the maturation of the midpalatal suture on cone beam CT. Dental Press J Orthod. 2016;21:115-25.
- [CrossRef] [PubMed] [Google Scholar]
- Rapid maxillary expansion and external root resorption in man: A scanning electron microscope study. Am J Orthod. 1981;79:630-52.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of rapid maxillary expansion and facemask therapy on the soft tissue profiles of class III patients at different growth stages. Eur J Dent. 2019;13:143-9.
- [CrossRef] [PubMed] [Google Scholar]
- Miniscrew-assisted nonsurgical palatal expansion before orthognathic surgery for a patient with severe mandibular prognathism. Am J Orthod Dentofacial Orthop. 2010;137:830-9.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of the effects of miniscrew incorporation in palatal expanders for young adults using finite element analysis. Korean J Orthod. 2018;48:81-9.
- [CrossRef] [PubMed] [Google Scholar]
- Alternate Rapid maxillary expansion and constriction (Alt-RAMEC) protocol: A comprehensive literature review. Turk J Orthod. 2019;32:47-51.
- [CrossRef] [PubMed] [Google Scholar]
- A new protocol for maxillary protraction in cleft patients: Repetitive weekly protocol of alternate rapid maxillary expansions and constrictions. Cleft Palate Craniofac J. 2005;42:121-7.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of the skeletodental effects of miniscrew-anchored and tooth-anchored facemask treatment in growing patients with skeletal class III malocclusions. Orthod Craniofac Res. 2023;26:695-703.
- [CrossRef] [PubMed] [Google Scholar]
- Application of combined maxillary skeletal expander and facemask treatment with an alternating rapid maxillary expansion and constriction protocol in a female adolescent with a class III Skeletal relationship. Taiwan J Orthod. 2018;30:43-55.
- [Google Scholar]
- Managing the developing Class III malocclusion with palatal expansion and facemask therapy. Am J Orthod Dentofacial Orthop. 2002;122:349-52.
- [CrossRef] [PubMed] [Google Scholar]
- Dentofacial effects of miniscrew-anchored maxillary protraction on prepubertal children with maxillary deficiency: A randomized controlled trial. Prog Orthod. 2023;24:22.
- [CrossRef] [PubMed] [Google Scholar]
- Class III treatment using facial mask: Stability after 10 years. Dental Press J Orthod. 2014;19:123-35.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of maxillary protraction with alternating rapid palatal expansion and constriction vs expansion alone in maxillary retrusive patients: A single-center, randomized controlled trial. Am J Orthod Dentofacial Orthop. 2015;148:641-51.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of two maxillary protraction protocols: Tooth-borne versus bone-anchored protraction facemask treatment. Prog Orthod. 2015;16:26.
- [CrossRef] [PubMed] [Google Scholar]
- Dentofacial effects of bone-anchored maxillary protraction: A controlled study of consecutively treated class III patients. Am J Orthod Dentofacial Orthop. 2010;138:577-81.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of two protocols for maxillary protraction: Bone anchors versus face mask with rapid maxillary expansion. Angle Orthod. 2010;80:799-806.
- [CrossRef] [PubMed] [Google Scholar]
- Early class III facemask treatment with the hybrid hyrax and AltRAMEC protocol. J Clin Orthod. 2014;48:84-93.
- [Google Scholar]
- Changes in the midpalatal and pterygopalatine sutures induced by micro-implant-supported skeletal expander, analyzed with a novel 3D method based on CBCT imaging. Prog Orthod. 2017;18:34.
- [CrossRef] [PubMed] [Google Scholar]
- Skeletal and dental changes after microimplant-assisted rapid palatal expansion (MARPE)-a Cephalometric and Cone-Beam Computed Tomography (CBCT) study. Clin Investig Orthod. 2022;81:84-92.
- [CrossRef] [Google Scholar]
- Short-term impact of microimplant-assisted rapid palatal expansion on the nasal soft tissues in adults: A three-dimensional stereophotogrammetry study. Korean J Orthod. 2020;50:75-85.
- [CrossRef] [PubMed] [Google Scholar]
- Nonsurgical miniscrew-assisted rapid maxillary expansion results in acceptable stability in young adults. Angle Orthod. 2016;86:713-20.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontic treatment and healthcare goals: Evaluation of multibrackets treatment results using PAR index (Peer Assessment Rating) Healthcare (Basel). 2020;8:473.
- [CrossRef] [PubMed] [Google Scholar]
- Long-term efficacy of reverse pull headgear therapy. Angle Orthod. 2006;76:915-22.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of miniscrew-supported rapid maxillary expansion in adolescents: A prospective randomized clinical trial. Angle Orthod. 2018;88:702-9.
- [CrossRef] [PubMed] [Google Scholar]
- Long-term effects of chincap therapy on skeletal profile in mandibular prognathism. Am J Orthod Dentofacial Orthop. 1990;98:127-33.
- [CrossRef] [PubMed] [Google Scholar]
- Growth of mandibular prognathism after pubertal growth peak. Am J Orthod Dentofacial Orthop. 1993;104:330-6.
- [CrossRef] [PubMed] [Google Scholar]
- The difference in cervical vertebral skeletal maturation between cleft lip/palate and non-cleft lip/palate orthodontic patients. Biomed Res Int. 2018;2018:5405376.
- [CrossRef] [PubMed] [Google Scholar]
- The values and value of patient-centered care. Ann Fam Med. 2011;9:100-3.
- [CrossRef] [PubMed] [Google Scholar]




