

Translate this page into:
Volumetric measurements of mandibular incisor root resorption following Forsus FRD EZ2 and Bionator appliance treatment using cone-beam computed tomography: A preliminary study

*Corresponding author: Dr. Pamir Meriç, Department of Orthodontics, Faculty of Dentistry, Trakya University, Edirne, Turkey. pamirmeric@trakya.edu.tr
-
Received: ,
Accepted: ,
How to cite this article: Meriç P, Zortuk FB, Karadede MI. Volumetric measurements of mandibular incisor root resorption following Forsus FRD EZ2 and Bionator appliance treatment using cone-beam computed tomography: A preliminary study. APOS Trends Orthod 2020;10(2):96-104.
Abstract
Objectives:
Root resorption is one of the frequently encountered problems in orthodontic treatments. The effects of functional appliances on root resorption have not been clearly demonstrated. The aim of this study was to compare volumetric root resorption of mandibular incisors after Bionator and Forsus appliance treatment using cone-beam computed tomography (CBCT).
Materials and Methods:
The study sample (n = 30) was selected from Class II div. 1 mandibular retrognathia patients treated with the Bionator and Forsus appliances. The first CBCT scans were taken before Bionator use and after 6 months. In the Forsus group, the first CBCT scans were taken before Forsus appliance use and after an overcorrected Class I relationship was obtained. The mean treatment time with the Forsus appliance was 5 ± 1.2 months. Mimics software was used for segmentation and volumetric measurements of mandibular incisor teeth root resorption.
Results:
In the Bionator group, statistically significant root volume loss was not found. In the Forsus group, the differences between before and after the treatment were not statistically significant for teeth 41, 31, and 32 (P > 0.05), whereas the difference was statistically significant for the lower right second incisor (P < 0.002). The percentage of volume loss (%) and root volume loss (mm3) was not statistically significant between groups.
Conclusions:
Following functional treatment with the Bionator and Forsus, statistically significant difference was not found between groups for mandibular incisor root resorption.
Keywords
Root resorption
Forsus
Bionator
Class II
Cone-beam computed tomography

INTRODUCTION
Orthodontically induced inflammatory root resorption is considered to be a particularly important sequelae associated with orthodontic treatment. Loss of apical root material is unpredictable and, when extending into the dentin, irreversible. Root resorption is a multifactorial problem[1,2] that is associated with patient characteristics such as age, gender, systemic conditions, type of malocclusion, and tooth structure, as well as with treatment factors such as the type of appliance, duration of treatment, orthodontic force magnitude, and type of tooth movement. The duration and magnitude of orthodontic forces have been evaluated from various aspects, and conflicting results have been reported in connection with root resorption.[3-6]
The previous research has shown that intrusive tooth movements may cause severe root resorption.[3,7,8] Clinically, root resorption can be detected with radiographs, but the limitations of 2D measurement of a 3D phenomenon make the quantitative value of these radiographs questionable.[9-11] As an alternative, cone-beam computed tomography (CBCT) offers a 3D evaluation of the roots in vivo and avoids the superimposition of structures.[12-14]
In correcting mandibular retrognathia, several removable and fixed functional appliances have been used to stimulate mandibular growth.[15-17] The main drawback of removable functional appliances is that patient compliance is an important factor in reaching treatment goals. For this reason, several fixed functional systems have been developed for Class II correction to eliminate the patient compliance issue. The efficacy of fixed functional appliances has been demonstrated in published studies,[15,16] which also reported that protrusion and intrusion of mandibular incisors were common.
Despite the common use of the fixed and removable functional appliances, literature about the consequences of its use is still lacking. To the best of our knowledge, no reported study has evaluated volumetric changes in mandibular incisor roots after Bionator and Forsus FRD EZ2 treatment. The purpose of this study was to evaluate the following null hypothesis: Root resorption degrees of the mandibular incisors are similar following the use of the Bionator and Forsus FRD EZ2 appliances.
MATERIALS AND METHODS
Subjects
A sample of 30 subjects (8 girls and 7 boys, mean age 12, 1 years in the Bionator group; 6 girls and 9 boys, mean age 12.7 years in the Forsus group) who had undergone functional treatment with the Bionator and the Forsus FRD EZ2 appliances was retrospectively selected from the archive of the Dicle University, Faculty of Dentistry, Department of Orthodontics. The patients were not exposed to extra radiation, particularly for this retrospective study. The study protocol was approved by the Research Ethics Committee at Trakya University, Faculty of Medicine (approval number TÜTF-BAEK 2016/203).
Inclusion criteria were as follows: (i) Skeletal Class II malocclusion (ANB >4°) due to a retrognathic mandible (SNB <78°), (ii) at least end-to-end Class II molar relationship on both sides, (iii) normodivergent growth pattern (SN-GoMe°: 32 ± 5), (iv) peak growth period (CS3), (v) lower dental arch crowding < 3 mm, and (vi) overjet <9 mm.
Exclusion criteria were as follows: (i) Unilateral Class II molar relationship, (ii) previous fixed/removable orthodontic treatment history, (iii) extracted or congenitally missing permanent teeth, (iv) systemic disease, and (v) severe proclination or crowding that requires extraction in the lower arch.
According to the power analysis at the 0.05 level and 80% power (based on a 0.56 mm standard deviation (SD) and a 0.6 mm detectable group difference regarding intrusion rates),[18] the minimum sample size needed for each group was 14.
Methods
Bionator appliance was constructed with the mandible protruded in an edge-to-edge incisor relationship, and bite was raised 2 mm [Figure 1a]. During the treatment period, patients were asked to wear the appliance for 24 h/day, except while eating. To facilitate lower molar extrusion, interocclusal acrylic was trimmed in the molar area and patients were checked at 4-week intervals.

- (a) Bionator appliance, (b) Forsus FRD EZ2 appliance.
In the Forsus group, patients were bonded with 0.018 inch slot pre-adjusted MBT prescription brackets (Gemini; 3M Unitek Corp., Monrovia, CA). The distance between the distal of the upper headgear tube and distal point of the lower canine tooth was measured using manufacturer’s ruler and appropriate size determined when the patient is closed in the centric occlusion. The Forsus was applied at the end of the leveling and aligning phase, when a 0.017 × 0.025 inch stainless steel archwire was inserted in both arches. Mandibular and maxillary archwires were cinched distal to the molars; the entire arch was in a figure eight pattern. The pushrods of the Forsus were placed on a by- pass archwire, bent from a 0.017 × 0.025 inch stainless steel wire. A by-pass archwire was connected from the lower first molar auxiliary tube to the distal side of the lower canine [Figure 1b]. A transpalatal archwire (0.9 mm diameter) was used to avoid buccal tipping of the maxillary molars. Patients were observed at 4-week intervals, and the appliances were activated with a split crimp, as required.
Cephalometric measurements were performed with Nemoceph software (Nemoceph NX 2006, Madrid, Spain).
Anteroposterior linear changes were analyzed with a reference line (RL) drawn perpendicularly from the sella point to the occlusal line. This line was transferred from the first to the second tracing by superimposition on the cranial base [Figure 2].[19]
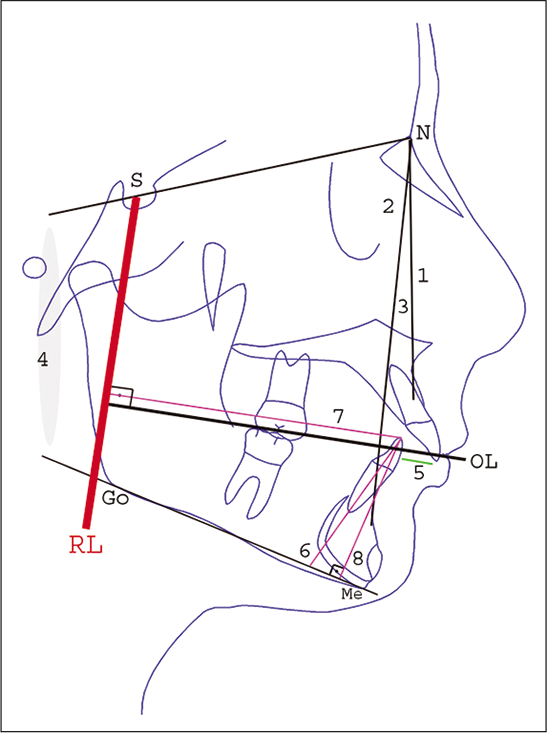
- Cephalometric analysis: (1) SNA (°), (2) SNB (°), (3) ANB (°), (4) SN-GoMe (°), (5) overjet (mm), (6) IMPA (°), (7) L1┴ RL (mm), (8) L1┴ MP (mm), RL indicates the reference line and OL indicates the occlusal line.
An i-CAT extraoral imaging system (Imaging Sciences International 17-19, Hatfield, PA) was used at 5 mA tube current, 120 kV tube voltage, and a scan time of 9.6 s, with a voxel size of 0.3 mm.
In the Bionator group, the first CBCT images (T1) were taken before appliance use and second images (T2) were taken after an overcorrected Class I molar relationship was obtained. The mean treatment time with bionator appliance was 6 months. In the Forsus group, the first CBCT images (T1) were taken when a 0.017 × 0.025 inch stainless steel archwire was inserted. The second CBCT images (T2) were taken after an overcorrected Class I molar relationship was obtained without the Forsus appliance in place. The mean treatment time with the Forsus appliance was 5 ± 1.2 months.
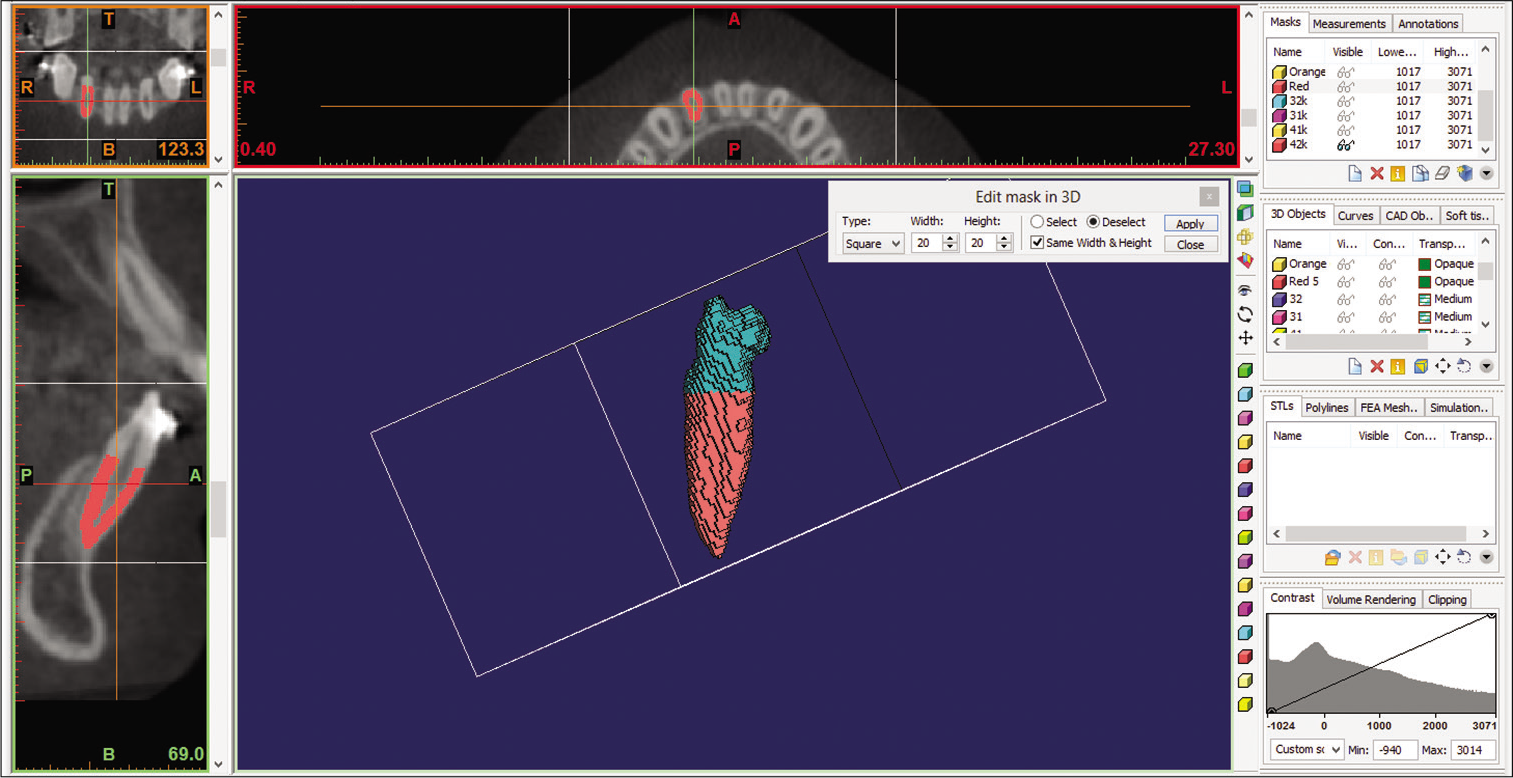
For 3D evaluations, segmentation was performed using Mimics software (Materialise NV, Leuven, Belgium) by the same researcher (PM). First segmentation process was performed in four steps: Selecting the threshold value, editing the mask in 3D, editing the mask in 2D, and reconstructing in 3D.[20] Each tooth was color coded [Figure 3]. Threshold values were set individually for each patient. The same Hounsfield units were used for the segmentation and reconstruction of before (T1) and after (T2) images for each patient.
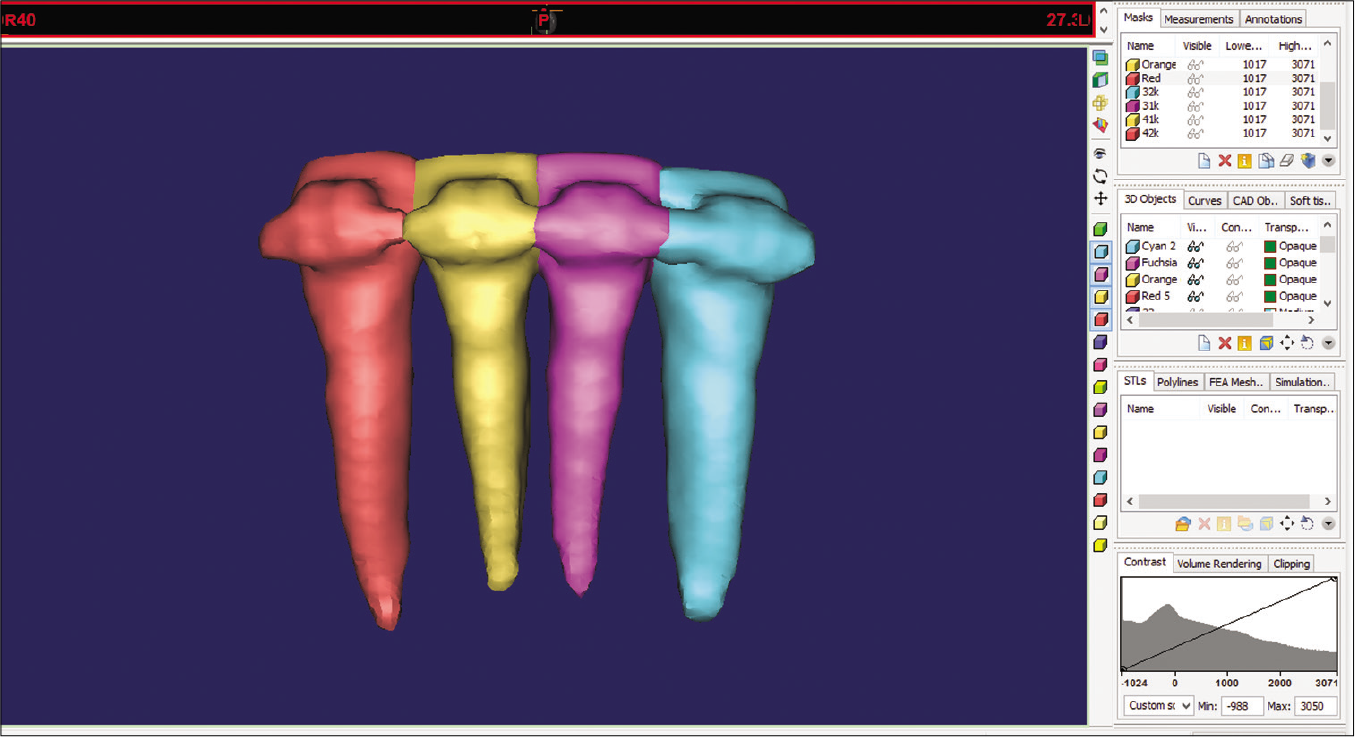
- Segmentation and reconstruction of the incisor teeth. Each tooth was color coded. Segmentation was performed in four steps: Selecting the threshold value, editing the mask in 3D, editing the mask in 2D, and reconstructing in 3D.
After the initial segmentation, an additional segmentation was performed to separate the root from the crown at the cementoenamel junction (CEJ). The incisal edge adjusted parallel to the floor [Figures 4 and 5]. Root volumes were measured from the CEJ to the tip of the root apex. Root volume was calculated automatically using Mimics software [Figure 6].
- 3D orientation of the incisor teeth. Incisal edges adjusted parallel to the floor.
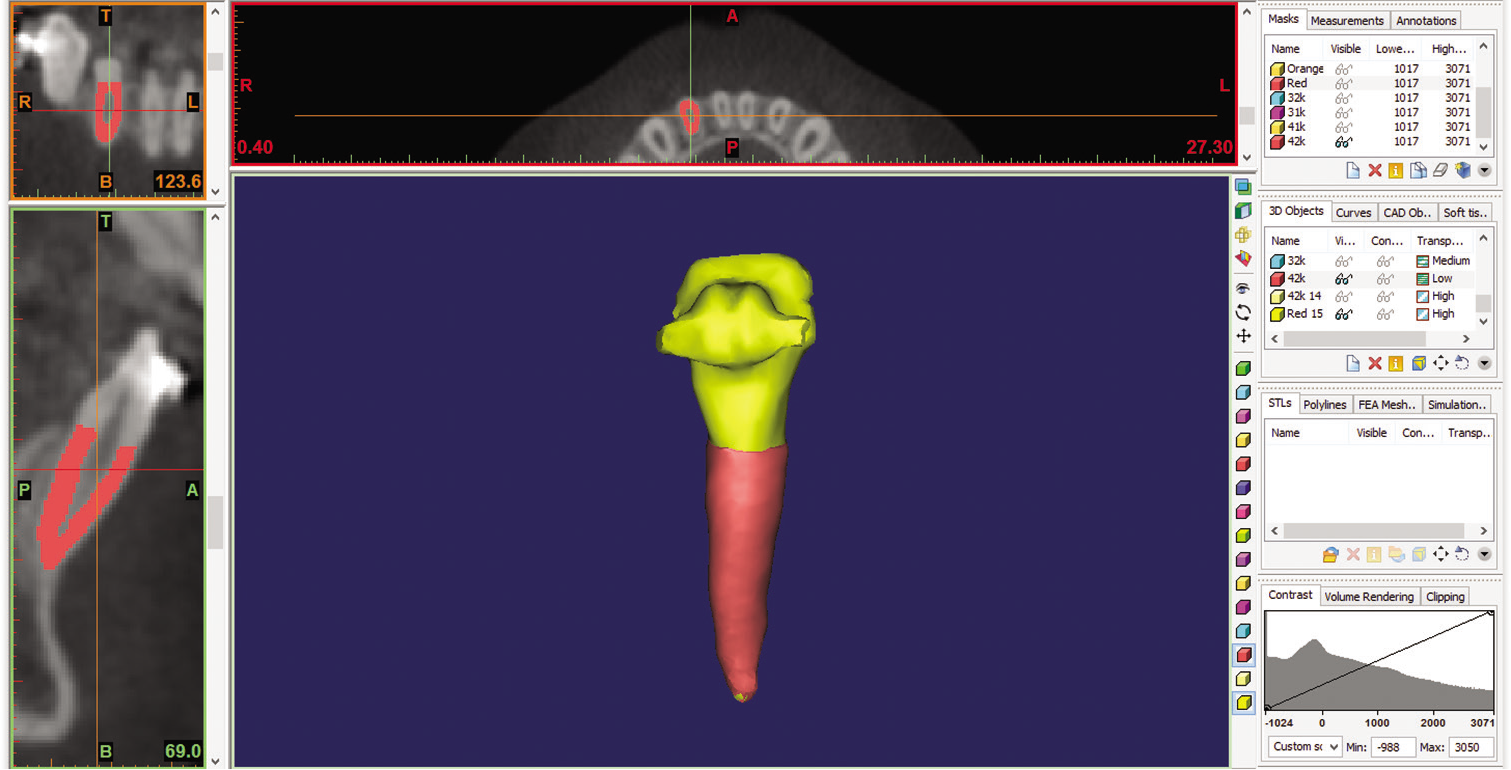
- Crown and root separation.
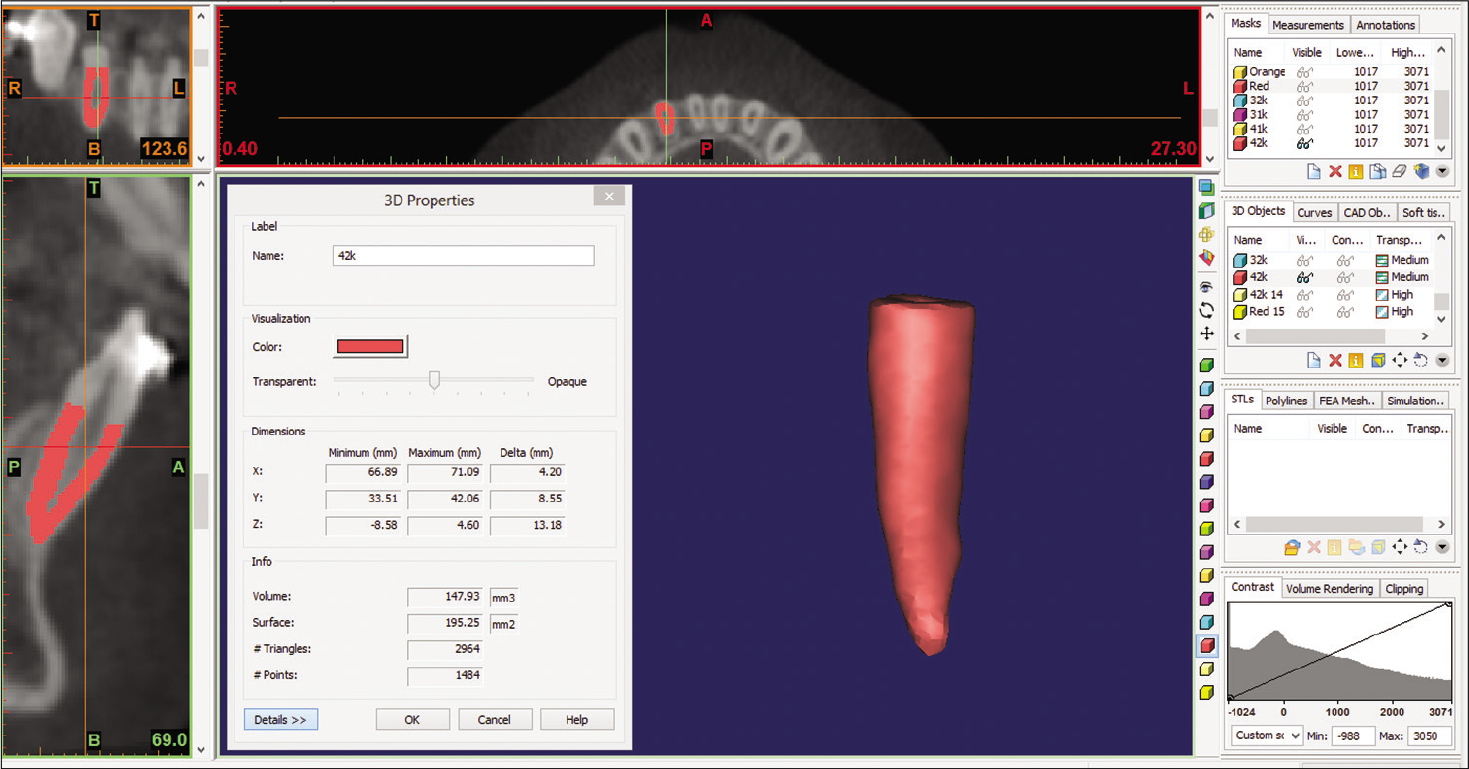
- Volumes were measured from the cementoenamel junction to the tip of the apex. Root volumes were calculated automatically using the software.
Statistical analysis
All statistical analyses were performed using IBM SPSS software (ver. 23). P < 0.05 was considered to indicate statistical significance. The Shapiro–Wilk test was used to test the normality of the data. Normally distributed data were evaluated with paired t-test to compare pre- (T1) and post- treatment (T2) cephalometric and root volume changes. To compare intergroup cephalometric differences, root volume losses, and percentages, independent samples t-test was used. The percentage of root volume loss was calculated by subtracting the T2 root volume from the T1 root volume, dividing the difference by the T1 volume, and multiplying by 100. To test the root volume losses and percentages for each tooth with another (42 vs. 41 vs. 31 vs. 32), the one-way analysis of variance test was used. CBCT images of 25 teeth were randomly selected 1 month later. Segmentation and volumetric measurements were repeated, and intraobserver reliability was evaluated using Bland–Altman plots.
RESULTS
The Bland–Altman plot [Figure 7] shows 95% limits of agreement (upper and lower lines), estimated by mean difference ± 1.96 SD of the difference.
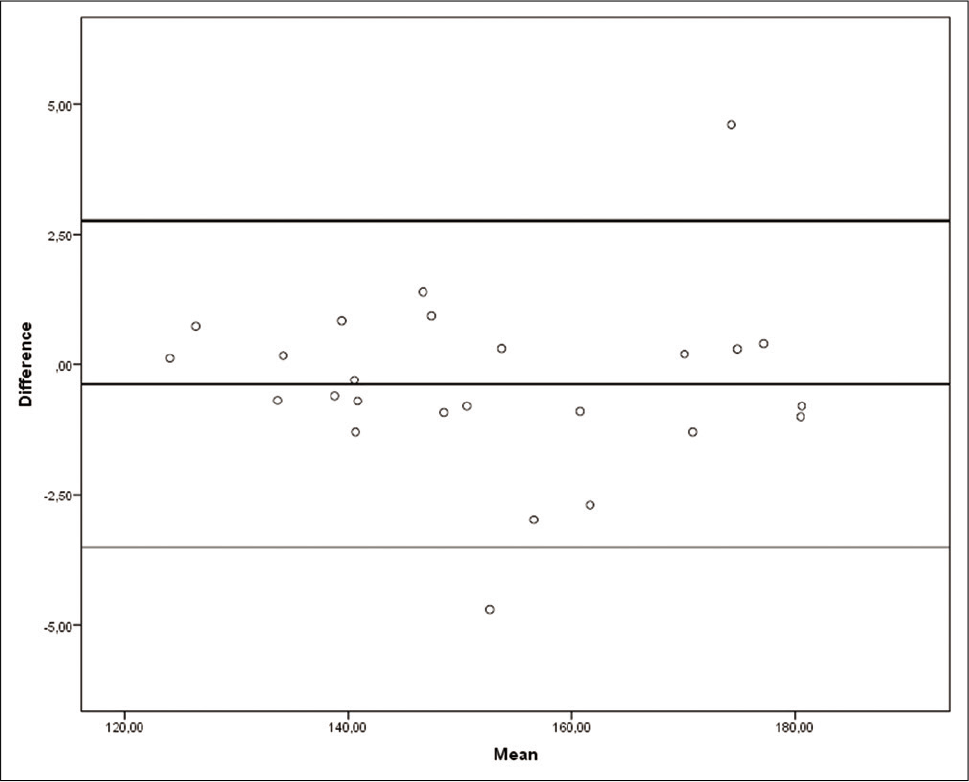
- Bland–Altman plots showing intraobserver reliability. Upper and lower lines show level of agreement. The range of agreement was defined as mean bias ± 1.96 SD.
Cephalometric findings
Descriptive statistics and statistical significance of T1 (pre- treatment) cephalometric values in Bionator and Forsus groups are shown in [Table 1].
| Cephalometric measures | n | Bionator | Forsus | P value |
|---|---|---|---|---|
| Mean±SD | ||||
| SNA (°) | 15 | 80.5±1.7 | 79.1±3 | NS |
| SNB (°) | 15 | 73.5±2.2 | 72.8±2.8 | NS |
| ANB (°) | 15 | 7±1.5 | 6.1±1.9 | NS |
| SN-GoMe (°) | 15 | 34.6±1.5 | 36.1±1.7 | NS |
| Overjet (mm) | 15 | 7.9±1.5 | 8.6±1.4 | NS |
| IMPA (°) | 15 | 100.6±5.7 | 94.8±5.5 | ** |
| L1┴RL (mm) | 15 | 70.3±5.6 | 67.3±4.2 | NS |
| L1┴MP (mm) | 15 | 36.8±3 | 37±2.4 | NS |
L1: Lower incisor, RL: Reference line, MP: Mandibular plane, NS: Not significant. **P <0.01
Statistical significance of the cephalometric changes between T1 and T2 time points in each group and between groups is presented in [Table 2].
| Bionator (T1-T2) n=15 | Forsus (T1-T2) n=15 | P value - significance | |||
|---|---|---|---|---|---|
| Cephalometric measures | Mean±SD | Mean±SD | Bionator T1-T2 | Forsus T1-T2 | Bionator versus Forsus |
| SNA (°) | 0.25±0.89 | 0.46±1.33 | NS | NS | NS |
| SNB (°) | ‒1.26±1.11 | ‒1.17±1.06 | *** | *** | NS |
| ANB (°) | 1.5±0.94 | 1.62±0.92 | *** | *** | NS |
| SN-GoMe (°) | ‒0.41±3.03 | ‒0.02±1.47 | NS | NS | NS |
| Overjet (mm) | 4.83±2 | 8.96±2.56 | *** | *** | *** |
| Mandibular dentoalveolar | |||||
| IMPA (°) | ‒3.66±3.53 | ‒8.12±4.77 | ** | *** | ** |
| L1┴RL (mm) | ‒3.96±2.15 | ‒4.68±2.66 | *** | *** | NS |
| L1┴MP (mm) | 0.06±0.76 | 2.11±1.39 | NS | *** | *** |
L1: Lower incisor, RL: Reference line, MP: Mandibular plane, NS: Not significant, SD: Standard deviation. **P <0.01, ***P <0.001
The cephalometric comparison showed that lower incisors showed significant proclination (IMPA) and protrusion (L1┴RL) in both groups. Lower incisor intrusion (L1┴MP, 2.11 ± 1.39 mm) was observed in the Forsus group.
Volumetric findings
Descriptive statistics and statistical significance of T1 (pre- treatment) and T2 (post-treatment) volumetric values between Bionator and Forsus groups are shown in [Tables 3 and 4], respectively.
| Tooth | n | Bionator | Forsus | P |
|---|---|---|---|---|
| Mean±SD (mm3) | ||||
| 42 | 15 | 161.5±30.3 | 147.8±26.2 | NS |
| 41 | 15 | 120.1±28 | 121.4±27 | NS |
| 31 | 15 | 122.1±29.3 | 122.6±27.5 | NS |
| 32 | 15 | 161.4±29.8 | 151.4±28.5 | NS |
NS: Not significant
| Tooth | n | Bionator | Forsus | P |
|---|---|---|---|---|
| Mean±SD (mm3) | ||||
| 42 | 15 | 156.7±30.1 | 141.7±28.3 | NS |
| 41 | 15 | 117.9±26.7 | 120.1±29.5 | NS |
| 31 | 15 | 120.3±28.8 | 120.1±28.3 | NS |
| 32 | 15 | 160.6±30.7 | 148.1±26.6 | NS |
NS: Not significant
Descriptive statistics and statistical comparison of volumetric changes in Bionator and Forsus groups are shown in [Table 5].
| Tooth | N | Bionator (T1-T2) (mm3) | P Significance | Forsus (T1-T2) (mm3) | P Significance |
|---|---|---|---|---|---|
| Mean±SD | Mean±SD | ||||
| 42 | 15 | 4.83±11.54 | NS | 6.13±6.28 | ** |
| 41 | 15 | 2.25±9.71 | NS | 1.24±7.87 | NS |
| 31 | 15 | 1.83±7.77 | NS | 2.50±8.25 | NS |
| 32 | 15 | 0.75±7.34 | NS | 3.29±6.84 | NS |
NS: Not significant, SD: Standard deviation. **P <0.01
The amounts of root volume loss in teeth 42, 41, 31, and 32 were 4.83 mm3, 2.25 mm3, 1.83 mm3, and 0.75 mm3 and 6.13 mm3, 1.24 mm3, 2.5 mm3, and 3.29 mm3, in Bionator [Figure 8] and Forsus [Figure 9] groups, respectively. These losses were not statistically significant in the Bionator group (P > 0.05), whereas in the Forsus group, significant root volume loss was observed in teeth 42 (P = 0.002). No significant difference was found between two groups.
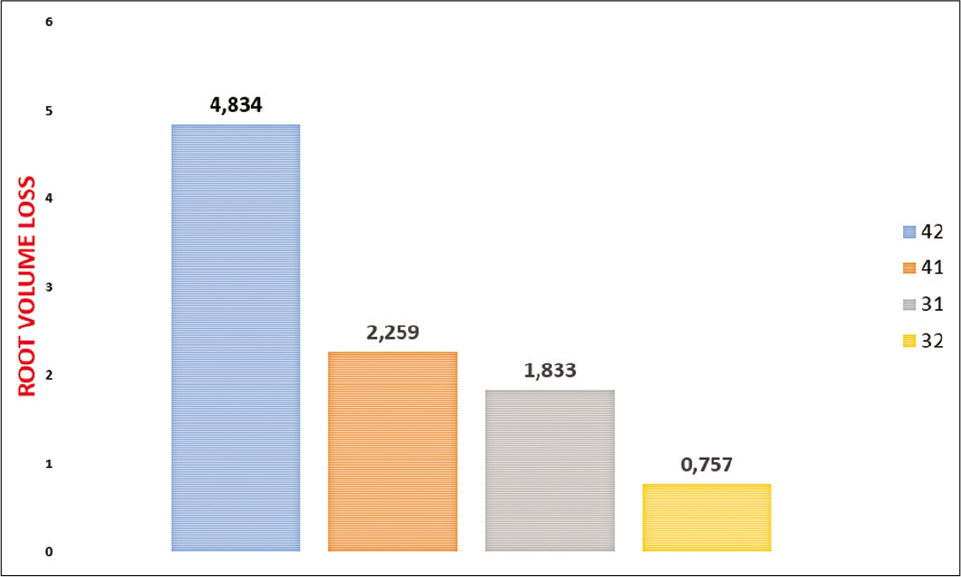
- Mean volume loss (mm3) in the Bionator group.
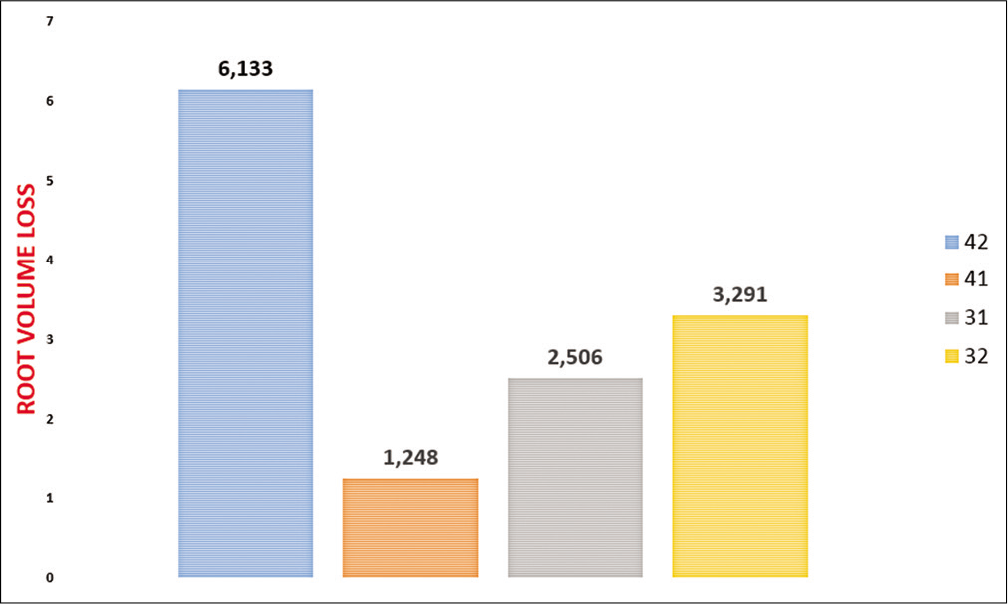
- Mean volume loss (mm3) in the Forsus group.
Percentages of root volume losses are shown in [Table 6]. When the lower incisors were compared with one another, the highest mean volume loss was found in tooth 42. However, no significant difference was found among the roots when the percentage of root volume loss was considered (P > 0.05; Table 6).
| Tooth | N | Bionator | Forsus | Bionator versusForsus | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Volume loss (mm3) (mean±SD) | Volume loss (%) (mean±SD) | P (mm3) (42 vs. 41 vs. 31 vs. 32) | P (%) (42 vs. 41 vs. 31 vs. 32) | Volume loss (mm3) (Mean±SD) | Volume loss (%) (mean±SD) | P (mm3) (42 vs. 41 vs. 31 vs. 32) | P (%) (42 vs. 41 vs. 31 vs. 32) | P | |||
| (mm3) | (%) | ||||||||||
| 42 41 31 32 |
15 15 15 15 |
4.83±11.54 2.25±9.71 1.83±7.77 0.75±7.34 |
2.77±6.84 1.43±8.19 1.33±6.58 0.45±4.51 |
NS | NS | 6.13±6.28 1.24±7.87 2.50±8.25 3.29±6.84 |
4.42±4.72 1.17±7.01 2.16±6.86 1.94±4.42 |
NS | NS | NS NS NS NS |
NS NS NS NS |
NS: Not significant, SD: Standard deviation
DISCUSSION
The introduction of fixed functional appliances eliminated the patient compliance problem in Class II correction. The nature of these appliances keeps the mandible in a forward position by applying continuous forces to the dentition.
The results here showed that Forsus and Bionator appliances created highly significant dentoalveolar changes. Due to the downward and forward forces to the mandibular dentition; the dentoalveolar changes consisted of significant lower incisor proclination, protrusion, and intrusion which were observed in the Forsus group. These results are consistent with previous reports.[15,16]
Except lower incisor intrusion, similar results were observed in the removable appliance group.[21]
Conventional intraoral imaging is not adequate for evaluating resorption cavities.[22,23] Follin[24] reported that 2D radiography was an inaccurate diagnostic tool for the detection of lingual root resorption. Scanning electron microscopy, histological sections, and micro-computed tomography evaluation require tooth extraction and are, therefore, not viable options for vital teeth.
However, it is now possible to detect root resorption in vivo with CBCT technology. A high level of reproducibility,[25] efficacy in detecting even minimal degrees of resorption,[26] and detection of slanted resorption[27] are possible with CBCT.
Segmentation and volume calculations of the roots in the present study may have been influenced by the voxel size, artifacts, and image quality of CBCT. According to Liedke et al.,[28] 0.4, 0.3, and 0.2 mm voxel resolutions produced the same results in detecting cavities that simulated external root resorption Wang et al.[29] reported that diagnosis was easier with 0.3 mm and 0.2 mm voxel resolutions. In the current study, we used 0.3 mm voxel resolution.
The concentration of the applied orthodontic forces can cause biological changes in the root, especially at the apex, resulting in root resorption.[2,3] Biological variability, genetic predispositions, and the effect of mechanical factors also cause root resorption.[14,30] In our study, the Forsus FRD EZ2 applied continuous forward and downward forces to the mandibular anterior dentition.
As mentioned before, to our knowledge, there is no other report assessing volumetric root resorption induced by the Forsus and Bionator, so it is difficult to make direct comparisons with the previous studies on root resorption.
In a CBCT study, Schwartz et al.[31] reported that the effects of the Herbst appliance in a group of post-pubertal patients showed minimal apical root resorption (<0.5 mm), mostly in the anchoring teeth. However, root structure loss was minimal and clinically insignificant. Nasiopoulos et al.[32] found a statistically significant decrease in the root surfaces of the lower first premolars in a banded Herbst group. In the mandibular first premolars, patients with already developed roots have more tendency to root length decrease. On the other hand, the length of these teeth increased in patients whose root development was not completed at the beginning of the fixed functional treatment. Janson et al.[33] evaluated mandibular and maxillary incisor root resorption and they reported that non-extraction treatment of Class II malocclusion with Class II elastics associated with fixed appliances causes similar root resorption as treatment with extraoral headgear and fixed appliances. Apical root resorption was predominantly mild and similar in the two groups. However, these studies evaluated root resorption using 2D periapical radiography. In another CBCT study, Lund et al.[27] reported that almost all patients and 55–91% of teeth showed some degree of root shortening, but few patients and teeth had root shortenings >4 mm. Teeth with incomplete root formation also show a higher biologic tolerance against to resorption. Even with application of strong forces, a wide open apex ensures that the tooth is exposed to fewer circulatory disorders.[34] Root length increases were found in all areas in patients whose root formation of the premolars was not fully completed at the beginning of the treatment. Immature, uncalcified tissues show better resistance to root resorption than their calcified forms.[35-37]
When the lower incisors were compared with one another, the highest mean volume loss was found in tooth 42 (6.13 mm3) in the Forsus group. This difference may be caused by the chewing and/or parafunctionally crux/clenching habits of the patients predominantly on the right side. However, no significant difference was found between two groups.
The results of this investigation may be attributed to the fact that the forces transmitted by the fixed functional appliance to the mandibular anterior dentition are mainly low in magnitude and within physiological limits. Similar results were observed in the removable appliance group.
Limitations
As mentioned, the results of this study were obtained from images having a voxel resolution of 0.3 mm. A recent study[29] evaluated the accuracy of volumetric measurement with CBCT using a 0.125 mm voxel resolution; they stated that the CBCT method was not sufficient for detecting cavities smaller than 1.07 mm3. Thus, small changes might not have been detected, causing an underestimation of volumetric changes. In the Forsus group, the first CBCT images were taken after the leveling and aligning phase. This could be lead to some resorption around the roots.
CONCLUSIONS
Within the limitations of the study;
Significant lower incisor proclination, protrusion, and intrusion were observed in the Forsus group. Similar results were observed in the Bionator group, except lower incisor intrusion
In the Forsus group, significant root volume loss was observed in teeth 42
In terms of root resorption, 3D volumetric evaluations did not show significant difference between the two treatment groups and the null hypothesis is accepted.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Orthodontically induced inflammatory root resorption. Part II: The clinical aspects. Angle Orthod. 2002;72:180-4.
- [Google Scholar]
- Root resorption after orthodontic treatment: Part 1. Literature review. Am J Orthod Dentofacial Orthop. 1993;103:62-6.
- [CrossRef] [Google Scholar]
- Ultrastructure of cementum and periodontal ligament after continuous intrusion in humans: A transmission electron microscopy study. Eur J Orthod. 2001;23:35-49.
- [CrossRef] [PubMed] [Google Scholar]
- Continuous vs. Discontinuous force application and root resorption. Angle Orthod. 1999;69:159-63.
- [Google Scholar]
- Constant versus dissipating forces in orthodontics: The effect on initial tooth movement and root resorption. Eur J Orthod. 2003;25:335-42.
- [CrossRef] [PubMed] [Google Scholar]
- Continuous versus interrupted continuous orthodontic force related to early tooth movement and root resorption. Angle Orthod. 1995;65:395-401.
- [Google Scholar]
- Physical properties of root cementum: Part 8. Volumetric analysis of root resorption craters after application of controlled intrusive light and heavy orthodontic forces: A microcomputed tomography scan study. Am J Orthod Dentofacial Orthop. 2006;130:639-47.
- [CrossRef] [PubMed] [Google Scholar]
- Root resorption after orthodontic intrusion and extrusion: An intraindividual study. Angle Orthod. 2005;75:912-8.
- [Google Scholar]
- Root resorption associated with orthodontic tooth movement: A systematic review. Am J Orthod Dentofacial Orthop. 2010;137:462-76.
- [CrossRef] [PubMed] [Google Scholar]
- Exploring the third dimension in root resorption. Orthod Craniofac Res. 2004;7:64-70.
- [CrossRef] [PubMed] [Google Scholar]
- Detection of apical root resorption after orthodontic treatment by using panoramic radiography and cone-beam computed tomography of super-high resolution. Am J Orthod Dentofacial Orthop. 2009;135:434-7.
- [CrossRef] [PubMed] [Google Scholar]
- Radiologically determined orthodontically induced external apical root resorption in incisors after non-surgical orthodontic treatment of Class II division 1 malocclusion: A systematic review. Prog Orthod. 2014;15:48.
- [CrossRef] [PubMed] [Google Scholar]
- Accuracy of volumetric measurement of teeth in vivo based on cone beam computer tomography. Orthod Craniofac Res. 2011;14:206-12.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of voxel size and partial volume effect on accuracy of tooth volumetric measurements with cone beam CT. Dentomaxillofac Radiol. 2013;42:20130070.
- [CrossRef] [PubMed] [Google Scholar]
- Effectiveness of comprehensive fixed appliance treatment used with the forsus fatigue resistant device in Class II patients. Angle Orthod. 2011;81:678-83.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment and posttreatment effects induced by the forsus appliance: A controlled clinical study. Angle Orthod. 2014;84:1010-7.
- [CrossRef] [PubMed] [Google Scholar]
- Long-term skeletal and dental effects and treatment timing for functional appliances in Class II malocclusion. Angle Orthod. 2013;83:334-40.
- [CrossRef] [Google Scholar]
- Treatment effects of intrusion arches and mini-implant systems in deepbite patients. Am J Orthod Dentofacial Orthop. 2012;141:723-33.
- [CrossRef] [PubMed] [Google Scholar]
- A cephalometric analysis of skeletal and dental changes contributing to Class II correction in activator treatment. Am J Orthod. 1984;85:125-34.
- [CrossRef] [Google Scholar]
- Evaluation and comparison of root resorption between tooth-borne and tooth-tissue-borne rapid maxillary expansion appliances: A CBCT study. Angle Orthod. 2015;86:46-52.
- [CrossRef] [PubMed] [Google Scholar]
- Cephalometric appraisal of Class II treatment effects after functional and fixed appliances: A retrospective study. Eur J Orthod. 2017;39:334-41.
- [CrossRef] [PubMed] [Google Scholar]
- Radiographic assessment of simulated root resorption cavities. Endod Dent Traumatol. 1987;3:21-7.
- [CrossRef] [PubMed] [Google Scholar]
- External root resorption: An experimental radiographic evaluation. Oral Surg Oral Med Oral Pathol. 1989;67:578-82.
- [CrossRef] [Google Scholar]
- Detection of lingual root resorptions in the intraoral radiographs. An experimental study. Swed Dent J. 2005;29:35-42.
- [Google Scholar]
- Cone beam computed tomography for assessment of root length and marginal bone level during orthodontic treatment. Angle Orthod. 2010;80:466-73.
- [CrossRef] [PubMed] [Google Scholar]
- Apical root resorption due to orthodontic treatment detected by cone beam computed tomography. Angle Orthod. 2013;83:196-203.
- [CrossRef] [PubMed] [Google Scholar]
- Apical root resorption during orthodontic treatment. Angle Orthod. 2012;82:480-7.
- [CrossRef] [PubMed] [Google Scholar]
- Influence of voxel size in the diagnostic ability of cone beam tomography to evaluate simulated external root resorption. J Endod. 2009;35:233-5.
- [CrossRef] [PubMed] [Google Scholar]
- Accuracy of volumetric measurement of simulated root resorption lacunas based on cone beam computed tomography. Orthod Craniofac Res. 2013;16:169-76.
- [CrossRef] [PubMed] [Google Scholar]
- Apical root resorption is associated with comprehensive orthodontic treatment but not clearly dependent on prior tooth characteristics or orthodontic techniques. J Am Dent Assoc. 2011;142:66-8.
- [CrossRef] [PubMed] [Google Scholar]
- Cone beam computed tomography study of apical root resorption induced by Herbst appliance. J Appl Oral Sci. 2015;23:479-85.
- [CrossRef] [PubMed] [Google Scholar]
- Premolar root changes following treatment with the banded herbst appliance. J Orofac Orthop. 2006;67:261-71.
- [CrossRef] [PubMed] [Google Scholar]
- Root resorption in Class II malocclusion treatment with Class II elastics. Am J Orthod Dentofacial Orthop. 2016;150:585-91.
- [CrossRef] [PubMed] [Google Scholar]
- Changes in root length during orthodontic treatment: Advantages for immature teeth. Eur J Orthod. 2002;24:91-7.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of class ii treatment with a banded herbst appliance on root lengths in the posterior dentition. Am J Orthod Dentofacial Orthop. 2011;139:465-9.
- [CrossRef] [PubMed] [Google Scholar]
- Changes in the physical properties of human premolar cementum after application of 4 weeks of controlled orthodontic forces. Eur J Orthod. 2006;28:313-8.
- [CrossRef] [PubMed] [Google Scholar]
- Predicting and preventing root resorption: Part I. Diagnostic factors. Am J Orthod Dentofacial Orthop. 2001;119:505-10.
- [CrossRef] [PubMed] [Google Scholar]




