

Translate this page into:
Cortical Piezo-Puncture as a Minimally Invasive Method for Reducing MiniScrew Implant Insertion Torque: A Preliminary in vitro Study
Address for correspondence: Prof. Juan Pablo Gomez, Calle 14 #23-26 of. 104 Pereira, Colombia. E-mail: jgomez@autonoma.edu.co
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Objective
The objective of this study was to determine the effect of cortical piezo-puncture (CPP) on maximum insertion torque (MIT), maximum removal torque (MRT), and maximum axial load (MAL) during the insertion of self-drilling miniscrew implants (MSI), in an experimental model with proximal epiphysis of bovine tibia.
Materials and Methods
A comparative study was conducted using two groups of 20 self-drilling MSI inserted in intact bone (control group) and in bone with previous CPP (experimental group). MIT, MRT, and MAL of the 20 mini implants of each group were measured. Using SPSS software, Student’s t-test was applied to compare MIT and MRT and the U-test Mann–Whitney test was applied to compare MAL in both groups as well as Pearson and Spearman correlation.
Results
In the experimental group, average values of 12.85 (±4,32) Newton x centimeters (Ncm), 13.7 (±4,54) Ncm, and 22,474 (±895,95) gF for MIT, MRT, and MAL were found, respectively. In the control group, average values found for MIT, MRT, and MAL were 20.2 (±4,7) Ncm, 22.3 (±5,17) Ncm, and 4688,7 (±320,18) gF, respectively. Statistically significant differences were observed in MIT, MRT, and MAL between control and experimental groups (P < 0,001).
Conclusions
CPP before insertion of orthodontic MSI in bovine tibia significantly reduces MIT, MRT, and MAL.
Keywords
Orthodontic anchorage procedures
piezosurgery
torque

Introduction
In 1880, when Jean and Marie Curie first described the piezoelectric effect, they were unaware that the phenomenon would give birth to piezosurgery, an innovative surgical technique that emerged from the need to find a safer and more accurate procedure to perform bone surgery.[1] Clinical and in vitro studies have shown that piezosurgery produces clean and precise osteotomies with smooth walls and reduced bleeding.[2,3] This method uses electric current to provoke oscillation of specialized tips that in contact with bone produce localized destruction of mineralized interface.[1] The piezoelectric device generates ultrasonic vibration with an average frequency of 25–29 kHz, allowing selective elimination of bone structure, without producing soft-tissue damage,[4,5] or heat-related osteonecrosis.
Various studies by Eriksson et al.[6-10] described the effect of heat generated during preimplant drilling on local hard tissue, concluding that temperatures above 47° during 1 min reduced bone’s ability to osseointegrate with implant material.
Preti et al.[11] assessed the osseointegration level of titanium implants located in a surgical field prepared with piezosurgery versus conventional rotary instruments in the mini-pig tibia. They observed fewer inflammatory cells, increased number of osteoblasts, increased bone morphogenetic protein-4 and transforming growth factor-B2 expression, and decreased expression of pro-inflammatory cytokines in the piezosurgery group, 7 and 14 days after osteotomy.
Kanomi[12] described for the first time the use of a micro screw inserted in bone for temporary orthodontic anchorage in 1997.
Miniscrew implants (MSIs), also known as temporary anchorage devices, have become an important part of orthodontic mechanotherapy. This group of devices is inserted intraorally in bone structures to provide anchorage, to prevent unwanted tooth movement, and disentangling age-old dilemmas in orthodontic biomechanics.
Two categories of MSI are currently available, according to its insertion technique: (1) self-tapping technique, in which the mini-implant is inserted after drilling a pilot hole in bone, using a motorized handpiece and (2) self-drilling technique in which the mini-implant has a sharp tip that directly perforates the bone, either manually or with a low-speed handpiece.[13]
Mini-crew “torque” has been described as the result of frictional resistance between the screw threads and bone tissue.[13] Maximum insertion torque (MIT) is expressed in Newton x centimeters (Ncm) and is the maximum torque value recorded during insertion of MSI. Maximum removal torque (MRT) is also expressed in Ncm and is the value of the maximum torque recorded during removal of MSI. Stability of MSI can be characterized as primary and secondary. The first is the mechanical stabilization immediately achieved after insertion, and the second is completed when new bone is formed at the bone-screw interface.[14]
To achieve initial stability after inserting a mini-implant, a minimum level of torque is required during insertion.[15] Studies have shown that increase in insertion torque can reduce the amount of micro motion and increase the success rate of dental implants.[15] However, excessive bone stress can cause necrosis and local ischemia and may reduce osseointegration and secondarily stability.[14] Animal studies have associated high-insertion torque with excessive retention of MSI and fracture of the cortical bone.[16]
It is fairly accepted that predrilling offers advantages in MSI success as it permits control of noxious high-insertion torque. Furthermore, it is acknowledged that conventional drilling implies risk of injurious hard-tissue heating and soft-tissue damage. Nonetheless, a minimally invasive, nonheating technique for MSI insertion site preparation has not been proposed.
The present study aims to determine the effect of a novel approach to preinsertion site preparation called “Cortical Piezo-Puncture” (CPP) on MIT, MRT, and MAL, with self-drilling mini-implant screws in an experimental surrogate bone model.
Materials and Methods
The project was submitted to the Bioethics Committee of Universidad Autónoma de Manizales. The suggested changes in biosafety protocols, management, and final disposal of residues were made, and the approval for the project by the Bioethics Committee was obtained by Act Number 44 of May 13, 2015.
For this experimental study, a total of 40 self-drilling conical, titanium alloy MSI (Royal Brand – GAC International) were used. CPP was performed with a Satelec-Acteon Piezotome 1® with TKW1 insert or piezo tip [Figure 1].
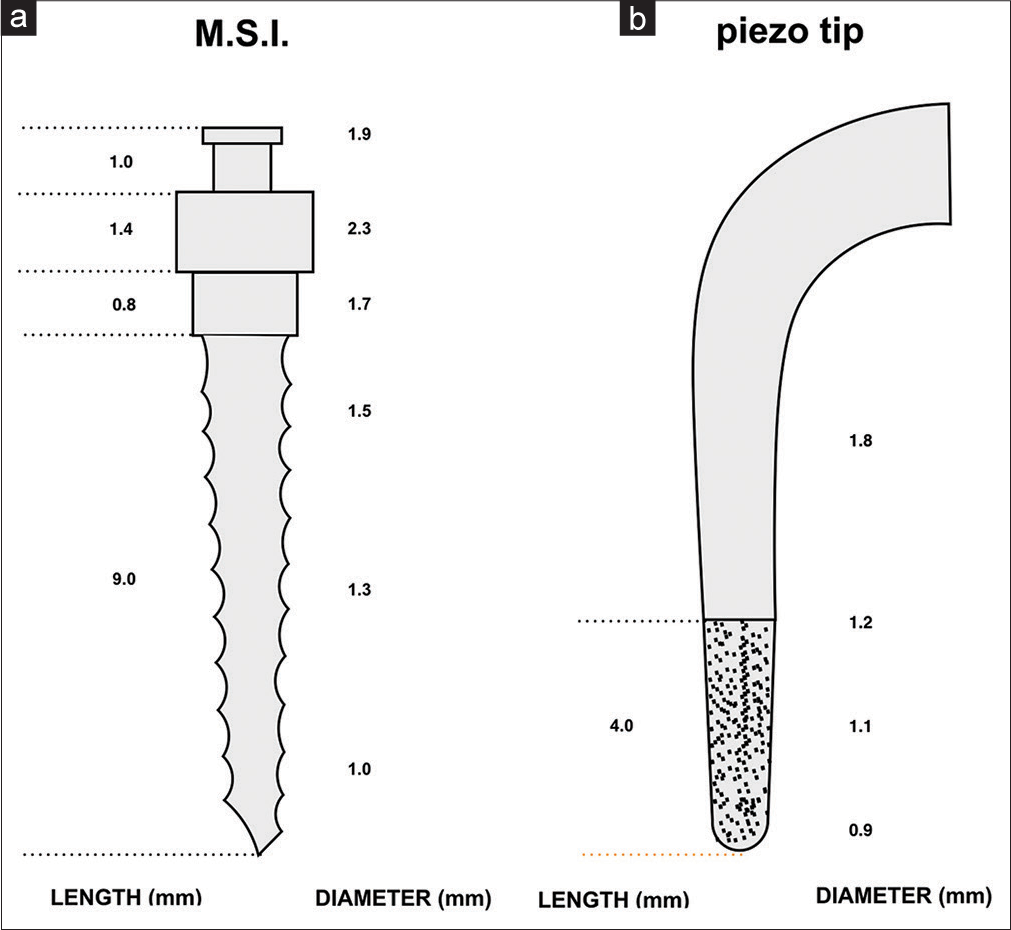
- Miniscrew implants (a) and TKW1 piezotome tip dimensions (b)
A confidence level of 95%, P = 0.05, the statistical power of 85%, standard deviation of 3.3 Ncm, and an expected difference of 3.3 Ncm were used, determined according to Meursinge et al. study in 2012.[17]
Bone sample inclusion criteria
Bovine tibias from the same animal, freshly slaughtered, intact, and clean [Figure 2]. Bovine tibias with obvious morphological alterations or belonging to two different animals were excluded from the study.
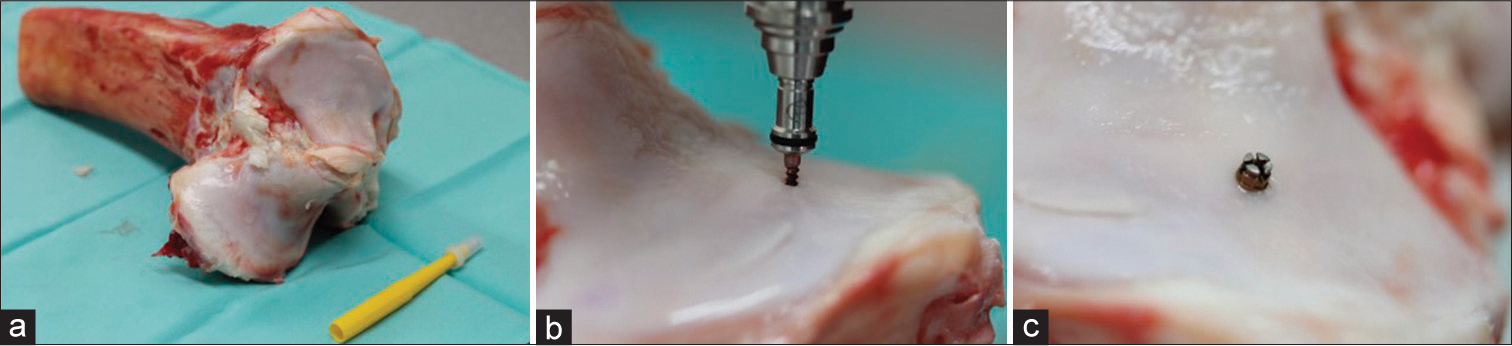
- (a) Proximal epiphysis of bovine tibia. (b) Miniscrew implants insertion. (c) Miniscrew implants in final position
The 40 self-drilling MSI used were divided into two groups: the experimental group comprising 20 mini-implants inserted into piezo-punctured sites and the control group that included 20 mini-implants inserted into the intact bone.
The day of the field test, two bovine proximal tibia epiphysis with articular cartilage was obtained from the same freshly slaughtered animal, which was stored in a polystyrene refrigerator with coolant bags at −7°C, properly sealed and labeled. Once transported to a dental laboratory, the worktable was disinfected with 80% ethyl alcohol spray and covered with plastic wrapping, which was also disinfected.
Sites for experimental group MSI insertion of were marked and numbered with blue ink. At approximately 1 cm of each blue mark, a red mark was added, corresponding to control group MSI insertion sites. The minimum distance between insertion sites was 1 cm. Cartilage thickness was measured in both groups with periodontal probe (1.5 mm average). Cortical thickness in the areas perforated was assessed using tomographic images, establishing a mean breadth of approximately 3 mm. 20 perforations were performed with TKW1 insert, each 4 mm deep, with approximately 2.5 mm penetration into the cortical bone tissue [Figure 3].
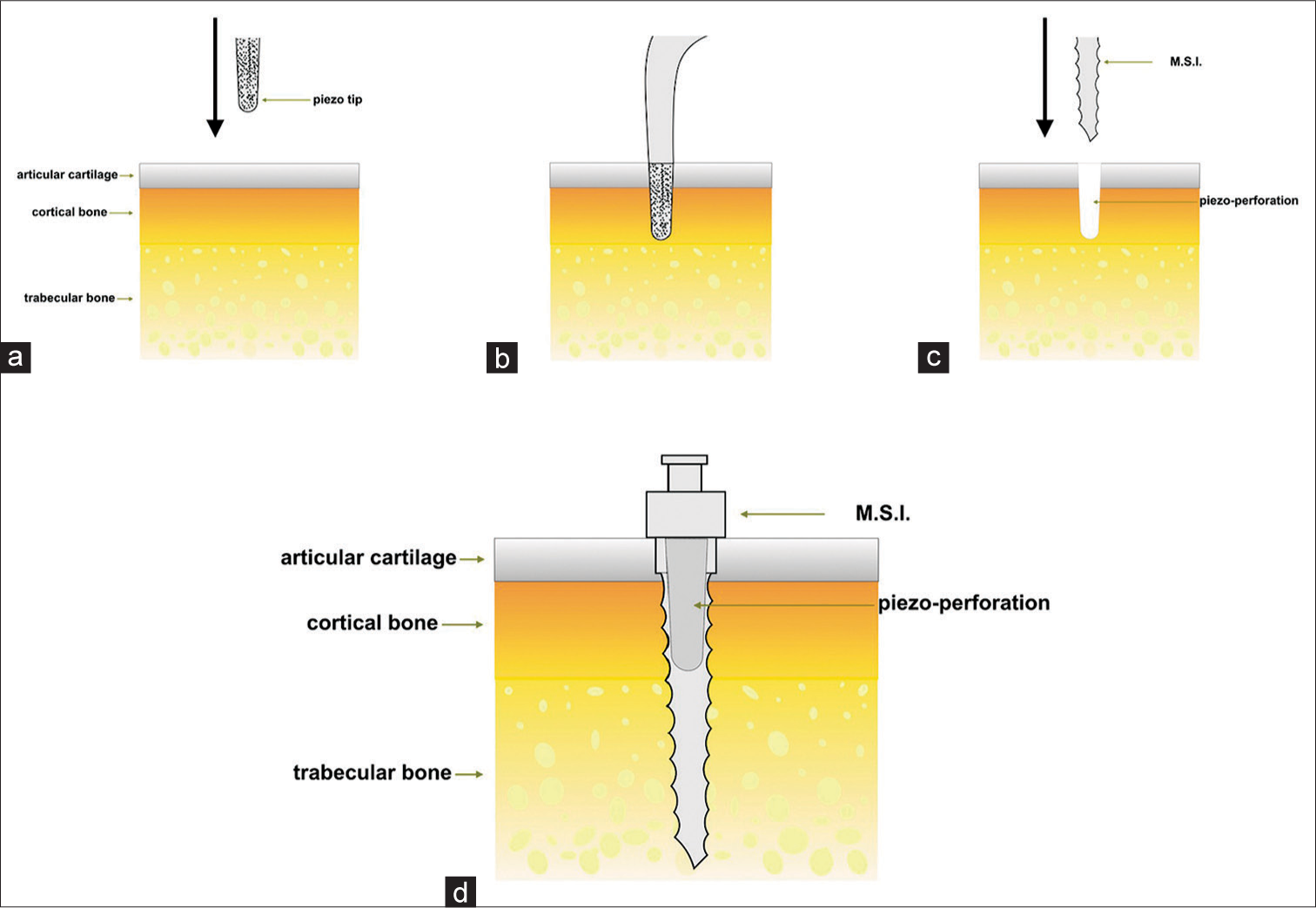
- Morphological description of cortical piezo-puncture with piezotome insert (a and b). Subsequent insertion of miniscrew implants (c and d)
The 20 MSI of the control group were inserted and removed in designated intact bone sites. MIT and MRT were measured using a digital torque meter (DTM PCE-TM 80, PCE Holding, GmbH). In addition, MAL value was registered using a digital gram scale (Constant®) on top of which the bone specimen was placed during MSI insertion. Identical procedure was repeated with the experimental group [Figure 4].

- Digital torque meter PCE-TM 80
The data of each group were recorded in a digital format and photographs of the process of insertion and removal of all mini-implants were taken. The residues were discarded in a red bag. Final disposition was undertaken according to the toxic waste management protocol, with input from the collection company RH, which was finally responsible for its incineration.
For statistical analysis, samples were assigned to two groups: experimental and control using a database editor, before being transferred to IBM SPSS® version 21 software package (IBM Corp., Armonk, NY). Descriptive statistics for each variable were performed; Shapiro–Wilk normality test and Levene homoscedasticity test were completed to determine whether comparative parametric or nonparametric tests were applied. Student’s t-test, U-test Mann–Whitney test, and Pearson and Spearman coefficient correlation were applied. All statistical tests were performed with 95% significance and 0.05 α.
Linear regression models were conducted to establish the association between MIT and MRT and between MIT and MAL, the adjusting of data significance for each model was validated by analysis of variance, the determination coefficient (R2), and residues analysis (Durbin–Watson).
Results
Descriptive statistics are observed in Table 1. MIT, MRT, and MAL average in the experimental group were lower than those observed in the control group.
| Variable | Average | CI | SE | SD |
|---|---|---|---|---|
| MIT experimental group | 12.8 Ncm | 10.8-14.8 | 0.97 | 4.3 |
| MIT control group | 20.2 Ncm | 18-22.4 | 1.05 | 4.7 |
| MRT experimental group | 13.7 Ncm | 11.5-15.8 | 1.02 | 4.5 |
| MRT control group | 22.3 Ncm | 19.8-24.7 | 1.16 | 5.1 |
| MAL experimental group | 2247.4 gF | 1828.08-2666.7 | 200.3 | 895.9 |
| MAL control group | 4688.7 gF | 4538.85-4838.5 | 71.60 | 320.1 |
MIT – Maximum insertion torque; MRT – Maximum removal torque; MAL – Maximum axial load; CI – Confidence interval; SE – Standard deviation; SD – Standard deviation
Normality test of Shapiro–Wilk and homoscedasticity Levene test was performed for each variable, which indicated that MIT and MRT are parametric variables, while MAL is nonparametric. This implied that to establish differences between groups, Student’s t test would be used for MIT and MRT and U Mann–Whitney for MAL [Table 2].
| Variable | Test | P |
|---|---|---|
| MIT | Student’s t test (t=5.15) | <0.001* |
| MRT | Student’s t test (t=5.56) | <0.001* |
| MAL | U Mann–Whitney (Z=5.19) | <0.001* |
MIT – Maximum insertion torque; MRT – Maximum removal torque; MAL – Maximum axial load
Statistically significant differences between MIT, MRT, and MAL between experimental and control group (P < 0.001) were found.
The effect of experimental or control group over MIT, MRT, and MAL variables was assessed with a simple linear regression for each variable. The result for the three cases was a directly proportional relation, statistically significant, where the MSI inserted with previous CPP obtained lower values for the three variables [Figures 5-7].
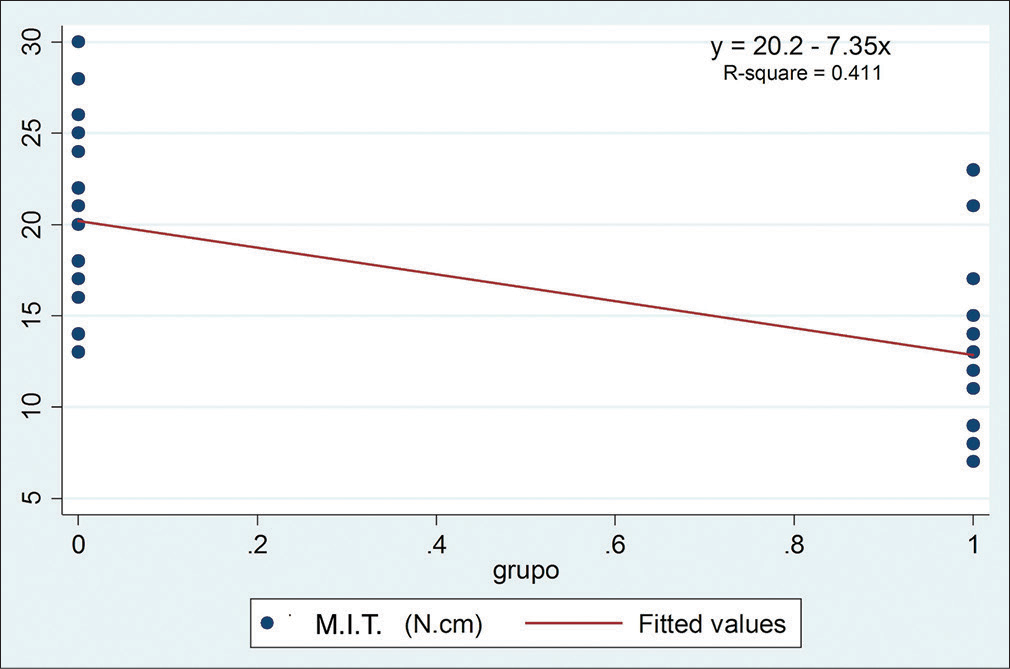
- Simple linear regression of maximum insertion torque in control and experimental groups
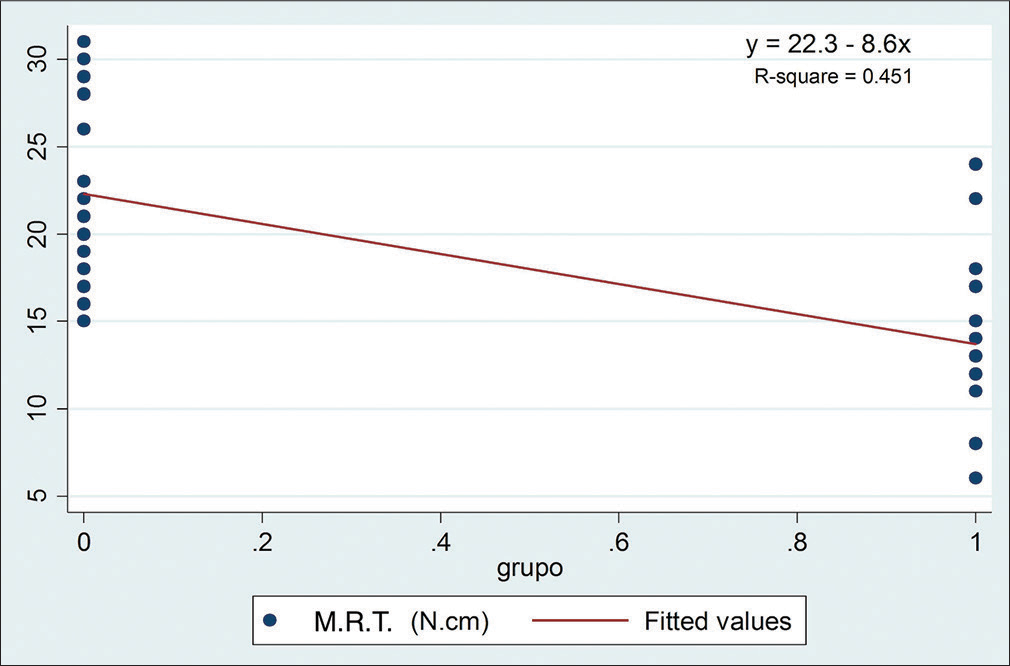
- Simple linear regression of maximum removal torque in control and experimental groups
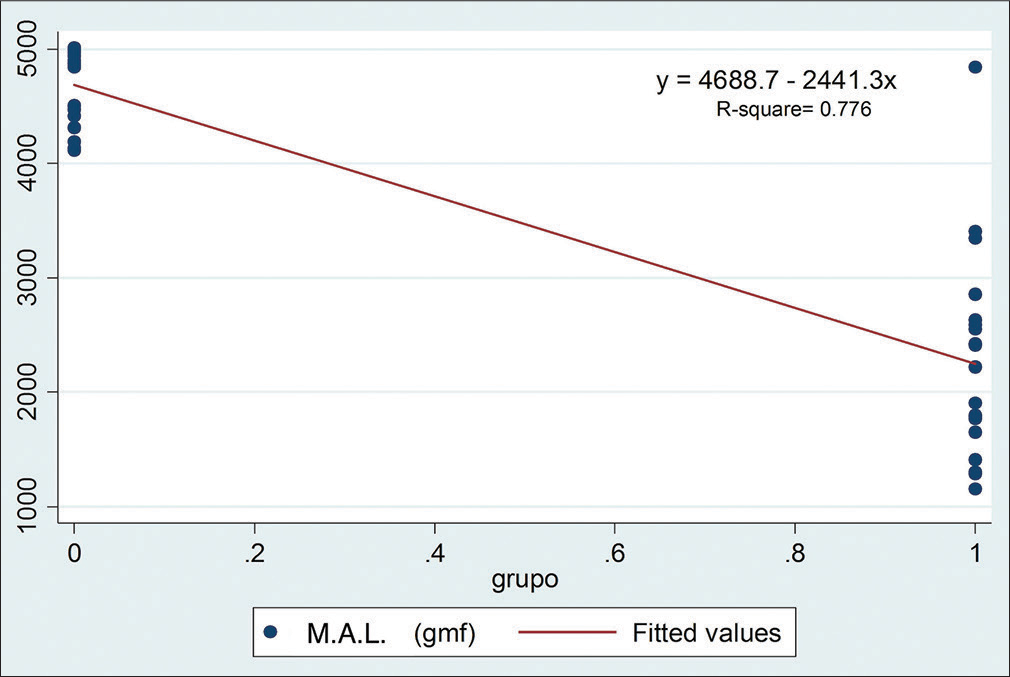
- Simple linear regression of maximum axial load in control and experimental groups
Discussion
Piezoelectric technique has gained popularity as a surgical resource that surmounts important limitations involved in conventional osteotomies. In this experimental study, the use of CPP demonstrated lower values of MIT, MRT, and MAL in comparison to the control group with statistically significant differences, during insertion of mini-implant screws. MRT values found were higher than the MIT in both groups. In a similar study, Suzuki and Suzuki[18] found results that are consistent with those found in the present study. These researchers reported that MRT values of mini-implants (self-drilling and self-tapping) were significantly higher than the MIT values in all inserted sites.
Prior studies suggest that large MIT values generate high levels of stress that cause local ischemia and tissue necrosis at bone-implant interface, which leads to poor osseointegration and consequent MSI failure. Consequently, one may safely assume that the relatively lower values of MIT are more favorable for higher MIS success rate.[15,19]
Meursinge et al.[17] in 2012 recognized that the multiple variables that affect the stability of orthodontic mini-implants are not yet entirely understood. It has been suggested that excessive torque forces applied during insertion of MIS can cause necrosis of surrounding bone and compromise its success rate.[14,15] Thus, it is crucial to recognize the levels of localized stress produced by torque to guarantee postinsertion stability of MSI.[17] Studies of dental implants have shown that increases in torque can reduce the amount of micromotion and increase its success rate.[20,21] However, excessive bone stress may cause necrosis and local ischemia and can prevent osseointegration and thus secondary stability.[14]
Motoyoshi et al. found that to favor MSI clinical success, the ideal level of torque required during insertion is between 5 and 10 Ncm. In addition, they concluded that cortical plate thickness conditioned the ideal diameter of the bur-drilled pilot hole (the thicker the cortical bone, the wider the recommended pilot hole diameter) but not the MIS overall success rate, although recommending a minimum of 1-mm cortical bone thickness at the placement site.[15,19] The present found MIT values considerably higher than those reported by Motoyoshi.
To register MIT maximum values, high precision sensors are required. Meursinge et al.[17] recommend digital sensors over mechanical devices because they can record consecutive MIT levels at higher frequency ranges and generate an immediate curve with these values. Accordingly, a digital torque sensor was used during this investigation to ensure more precise readings.
In an in vivo study, Suzuki and Suzuki found that MSI insertion and removal torque average values vary considerably depending on the screw type. They observed that self-drilling screws evidenced higher MIT than predrilling screws. Besides, MRT values for predrilling and self-drilling screws were significantly higher than its MIT in all inserted sites. These results suggest that relatively lower values of MIT are more favorable for osseointegration than higher values.[18]
The most common reason for fracture of mini-implants is exposure to increased torsional stress during its insertion or removal.[22]
After studying peak torque values in acrylic implant sites, Whang et al.[13] concluded that using a torque-limiting screwdriver or to perform predrilling of cortical bone seems justified for some MIS insertion to reduce its risk of fracture.
Laboratory experiments have shown that MIT forces of 23 Ncm and higher can cause fracture of mini implant.[23] Fracture incidence in clinical use is 3%–4% according to Chen et al.[24] Maximum insertion and removal torque values found in the present study were slightly under the values reported to involve a high risk of fracture, while still maintaining appropriate levels of initial stability associated with sufficient initial torque values.
Pithon et al.[25] in their research of MIT and MRT of mini-implants conclude, as, in this study, that insertion torques were clearly associated with removal torques. Similar studies in animals have shown that self-drilling or self-tapping technique and the diameter of pilot hole can significantly influence the MIT values.[26,27] By changing these variables, clinicians can insert mini implants with MIT desired levels and then achieve adequate primary stability even in places with fragile or rigid bone. Surgical procedures can also be modified to reduce MIT values, preventing mini-implant fracture.[28] In this case, CPP previous to mini-implant insertion was used as a method to reduce MIT and MRT values.
Wilmes et al.[29] in 2011 claimed that the reduced diameter of mini-implants involves risk of fracture when MRT values are too high. Another study by Wilmes and Drescher[30] in the same year, reported that predrilling is required in regions with high bone densities, which include the jaw, medial parts of the upper alveolar ridge, and palate. Under these considerations, CPP should be considered as an alternative procedure to bur drilled pilot holes to reduce fracture risk during MSI insertion, especially when low screw diameter and high bone density and width are a clinical concern.
A high axial load applied during insertion of MSI increases the risk of accidents and produces a greater level of discomfort perceived by the patient. Although this variable (patient discomfort) was not measured, one could safely argue that the significant reduction of MAL observed after CPP was performed could improve patient experience during MSI insertion.
The present study used proximal epiphysis of the bovine tibia as a surrogate model, given its similarity to the characteristics of the human jawbone,[31] including the morphological and mechanical resemblance between articular cartilage of tibia and alveolar gingival tissue and the presence of cortical and trabecular bone. Research models using animal specimens to study problems concerning human beings are considered simplified representations of reality. Although comparable to human jawbone in certain microarchitectural and biomechanical characteristics, the inference of results to human setting must be done with caution. Accordingly, the results of this work require corroboration through clinical studies in human maxillary and mandibular bone, and ideally, through controlled clinical trials.
Conclusions
In an in vitro, experimental model, CPP, before insertion of self-drilling mini-implants in bovine bone significantly reduced MIT, MRT, and MAL values when compared to its insertion in intact bone.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Piezoelectric surgery: Twenty years of use. Br J Oral Maxillofac Surg. 2008;46:265-9.
- [Google Scholar]
- Characterisation of bone following ultrasonic cutting. Clin Oral Investig. 2013;17:905-12.
- [Google Scholar]
- The piezoelectric and rotatory osteotomy technique in impacted third molar surgery: Comparison of postoperative recovery. J Oral Maxillofac Surg. 2008;66:2444-8.
- [Google Scholar]
- Piezosurgery: An ultrasound device for cutting bone and its use and limitations in maxillofacial surgery. Br J Oral Maxillofac Surg. 2004;42:451-3.
- [CrossRef] [Google Scholar]
- Piezoelectric osteotomy in hand surgery: First experiences with a new technique. BMC Musculoskelet Disord. 2006;7:36.
- [Google Scholar]
- Temperatures during drilling for the placement of implants using the osseointegration technique. J Oral Maxillofac Surg. 1986;44:4-7.
- [Google Scholar]
- Thermal injury to bone. A vital-microscopic description of heat effects. Int J Oral Surg. 1982;11:115-21.
- [CrossRef] [Google Scholar]
- The effect of heat on bone regeneration: An experimental study in the rabbit using the bone growth chamber. J Oral Maxillofac Surg. 1984;42:705-11.
- [CrossRef] [Google Scholar]
- Heat caused by drilling cortical bone. Temperature measured in vivo in patients and animals. Acta Orthop Scand. 1984;55:629-31.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of bone viability after heat trauma. A histological, histochemical and vital microscopic study in the rabbit. Scand J Plast Reconstr Surg. 1984;18:261-8.
- [Google Scholar]
- Cytokines and growth factors involved in the osseointegration of oral titanium implants positioned using piezoelectric bone surgery versus a drill technique: A pilot study in minipigs. J Periodontol. 2007;78:716-22.
- [CrossRef] [PubMed] [Google Scholar]
- An in vitro investigation of peak insertion torque values of six commercially available mini-implants. Eur J Orthod. 2011;33:660-6.
- [Google Scholar]
- Assessment of implant stability as a prognostic determinant. Int J Prosthodont. 1998;11:491-501.
- [CrossRef] [PubMed] [Google Scholar]
- Recommended placement torque when tightening an orthodontic mini-implant. Clin Oral Implants Res. 2006;17:109-14.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of the diameter and shape of orthodontic mini-implants on microdamage to the cortical bone. Am J Orthod Dentofacial Orthop. 2010;138(8):e1-8.
- [Google Scholar]
- Insertion torque and success of orthodontic mini-implants: A systematic review. Am J Orthod Dentofacial Orthop. 2012;142:596-614.e5.
- [CrossRef] [PubMed] [Google Scholar]
- Placement and removal torque values of orthodontic miniscrew implants. Am J Orthod Dentofacial Orthop. 2011;139:669-78.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of cortical bone thickness and implant placement torque on stability of orthodontic mini-implants. Int J Oral Maxillofac Implants. 2007;22:779-84.
- [Google Scholar]
- Implant micromotion is related to peak insertion torque and bone density. Clin Oral Implants Res. 2009;20:467-71.
- [CrossRef] [PubMed] [Google Scholar]
- Correlation between placement torque and survival of single-tooth implants. Int J Oral Maxillofac Implants. 2005;20:769-76.
- [Google Scholar]
- Risks and complications of orthodontic miniscrews. Am J Orthod Dentofacial Orthop. 2007;131:S43-51.
- [Google Scholar]
- Peak torque values at fracture of orthodontic miniscrews. J Clin Orthod. 2007;41:326-8.
- [Google Scholar]
- The use of microimplants in orthodontic anchorage. J Oral Maxillofac Surg. 2006;64:1209-13.
- [Google Scholar]
- In vitro evaluation of insertion and removal torques of orthodontic mini-implants. Int J Oral Maxillofac Surg. 2011;40:80-5.
- [Google Scholar]
- Biomechanical and histological comparison of self-drilling and self-tapping orthodontic microimplants in dogs. Am J Orthod Dentofacial Orthop. 2008;133:44-50.
- [Google Scholar]
- A torque removal study on the primary stability of orthodontic titanium screw mini-implants in the cortical bone of dog femurs. Int J Oral Maxillofac Surg. 2008;37:647-50.
- [Google Scholar]
- Potential of self-drilling orthodontic microimplants under immediate loading. Am J Orthod Dentofacial Orthop. 2010;137:496-502.
- [Google Scholar]
- Fracture resistance of orthodontic mini-implants: A biomechanical in vitro study. Eur J Orthod. 2011;33:396-401.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of bone quality, implant type, and implantation site preparation on insertion torques of mini-implants used for orthodontic anchorage. Int J Oral Maxillofac Surg. 2011;40:697-703.
- [CrossRef] [PubMed] [Google Scholar]
- An in Vitro Surrogate Model of the Human jaw for the Biomechanical Evaluation of Dental Implants [Thesis doctoral] thesis
- [Google Scholar]




