

Translate this page into:
Interdisciplinary Management of an Orthodontic Patient with Temporomandibular Disorder
Address for correspondence: Dr. Franklin Tsang Tsang She, Faculty of Dentistry, The University of Hong Kong, Hong Kong, China. E-mail: she@smileclinic.com.hk
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
A 21-year-old female patient presented with temporomandibular disorder, skeletal Class II, Angle Class II division 2 malocclusion, gummy smile, and incomplete overbite was managed successfully by splint therapy and orthodontic camouflage with miniscrew anchorage and extraction. She was treated with occlusal splint to alleviate signs and symptoms of anterior disc displacement without reduction and the associated masticatory dysfunction and revealed the true malocclusion before orthodontic treatment. Computer software facilitated the formulation of visual treatment objective (VTO) and occlusogram which guided the whole arch intrusion, retraction of the upper anterior segment, mesialization of lower left dentition, and distalization of lower right dentition. In this case report, the rationale and importance of preorthodontic splint therapy and specific considerations in orthodontic mechanics for managing this patient were discussed.
Keywords
Miniscrew anchorage
orthodontic camouflage
splint therapy
temporomandibular disorder
whole arch intrusion

Introduction
There is a significant proportion of orthodontic patients presenting with temporomandibular disorder (TMD) prior to treatment.[1,2] Since the etiology of TMD is multifactorial, there is a lack of consensus on its management before the commencement of orthodontic treatment. Over the years, there are numerous investigations showing controversial findings on the influence of orthodontic treatment over the signs and symptoms of TMD.[3] Even though some studies have indicated that certain malocclusions might relate to TMD and there are some influences of orthodontic treatment on TMD patients,[4] significant scientific evidences have demonstrated negative correlation between orthodontic treatment and aggravation of TMD.[5] In many cases, orthodontists would therefore assume that TMD can be ignored and orthodontic treatment itself would improve the problem.[6]
In this case report, interdisciplinary management of prosthodontic and orthodontic approaches is described. The patient was treated with occlusal splint which eliminated the occlusal interferences in relation to the presence of TMD temporarily before orthodontic treatment. It relieved TMD signs and symptoms and revealed the true malocclusion at centric relation. Computer software formulated visual treatment objective (VTO) and occlusogram guided the orthodontic treatment. Skeletal Class II camouflage therapy with miniscrew anchorage was performed followed by occlusal equilibrium and direct composite buildups of peg-shaped lateral incisors. The collaboration of splint therapy, orthodontic treatment, and dental restorations improved function and esthetics of the dentofacial complex. In this case report, the rationale and importance of preorthodontic splint therapy, design and materials for occlusal splints, and specific considerations of orthodontic mechanics in managing patients with TMD were discussed.
Case Report
The patient was a 21-year-old female who requested orthodontic treatment from the first author with the chief complaint of crooked teeth. Extraoral examination revealed convex profile, protrusive maxilla, retrusive mandible, increased incisal exposure at rest, gummy smile, and chin deviation to the left side [Figure 1]. In sagittal dimension, she presented with Class II half unit molar and canine relationship with retroclined upper and lower incisors. Skeletal Class II base with protrusive maxillary dentoalveolar process and retrognathic mandible were recorded [Figures 2, 3 and Table 1]. In the vertical dimension, she presented with increased overbite due to increased curve of Spee and overeruption of upper incisors. There was incomplete overbite meaning that upper and lower incisors presented with vertical overlap without inter-occlusal contact. In the transverse dimension, the condylar head was resorbed on the left side with lower dental midline deviated to the same side [Figure 4]. Based on the history that the occlusion was stable over a few years and there was negative finding of rheumatoid and antinuclear factors on blood test, the left condyle lesion was suggestive of stable idiopathic condylar resorption. In addition, peg-shaped upper lateral incisors, impacted lower right third molar, and dental crowding were noted.

- Pretreatment extra- and intra-oral photographs
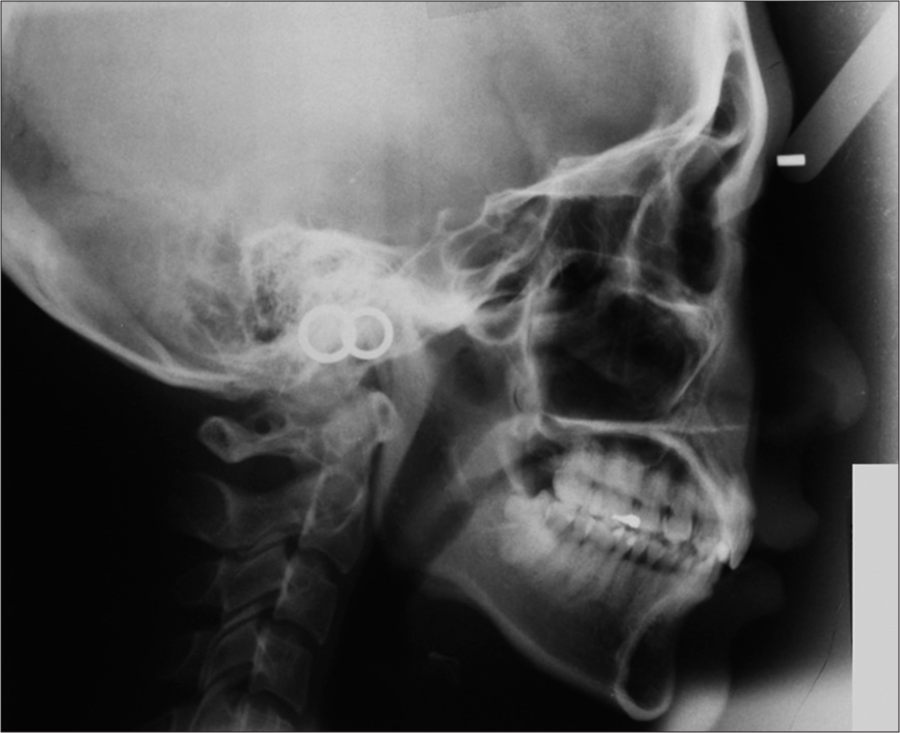
- Pretreatment lateral cephalogram
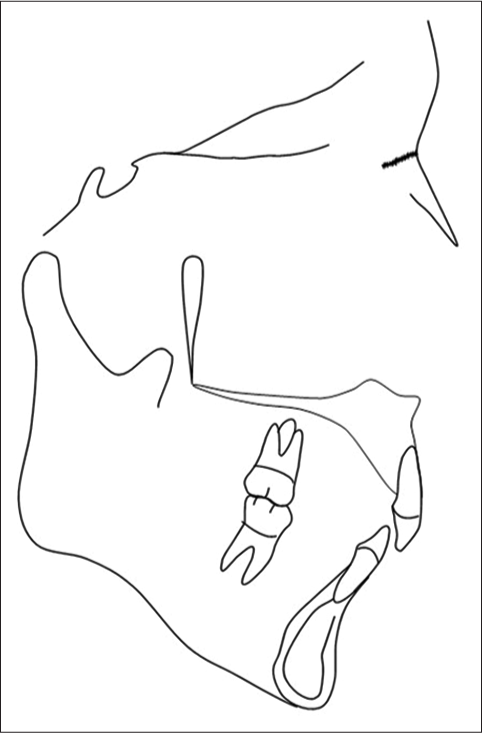
- Tracing of pretreatment lateral cephalogram
| Norm | Pre-tx | Post-tx | Difference | |
|---|---|---|---|---|
| SNA | 82°±3.5 | 85° | 83° | -2° |
| SNB | 79°±3 | 77° | 77° | ±0° |
| ANB | 3°±2 | *8° | *6° | -2° |
| Wits appraisal | -4.5±3 mm | **2 mm | *1 mm | -1 mm |
| Upper incisor to maxillary plane | 118°±6 | **82° | **101° | +19° |
| Lower incisor to mandibular plane | 97°±7 | 92° | 96° | +4° |
| SN to maxillary plane | 8°± 3 | 6° | 6° | ±0° |
| SN to mandibular plane | 34°±4.5 | 33° | 33° | ±0° |
| Lower facial proportion | 55% | 56% | 56% | ±0% |
*Within two standard deviations. **Exceeded two standard deviations
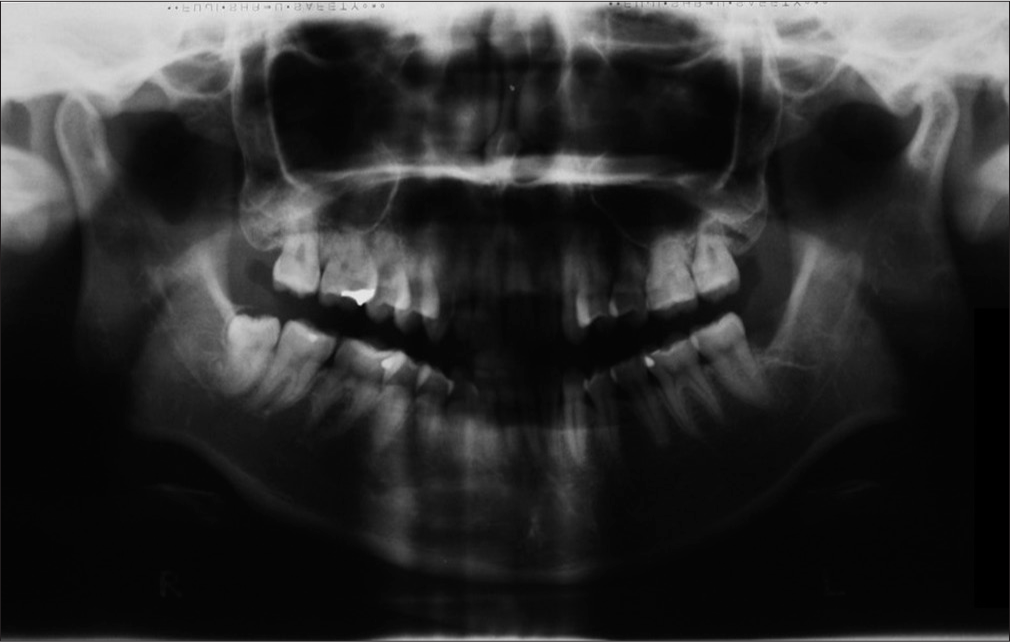
- Pretreatment panoramic radiograph
Temporomandibular joint (TMJ) examination revealed that the patient presented with discrepancy of centric occlusion and centric relation and restricted mouth opening. To eliminate the adverse effect of TMD and reveal the true malocclusion, she was then referred to the second author who is a prosthodontist for the management of TMD.
Temporomandibular disorder management before orthodontic treatment by the second author
At the TMD analysis visit, the patient complained of occasional spontaneous pain, temporomandibular sound of her left TMJ, and limited mouth opening. The patient had no history of head and neck injury. Clinical examination showed that there was pain on palpation of the right and left TMJ. Tenderness to palpation of the left temporalis muscles during mouth opening was recorded. Maximum mouth opening was 28 mm with intensity of left TMJ pain in 6 out of 10 of which 0 and 10 represented no and extreme pain, respectively. Right and left lateral mandibular movements were 7 mm and 11 mm, respectively. The patient experienced pain on the right lateral mandibular movement with intensity in 7 out of 10 on the left TMJ. Locking of the left TMJ was recorded.
The TMD analysis led to the diagnosis of anterior disc displacement without reduction and the associated masticatory dysfunction. Behavioral modifications such as bilateral mastication at the mandibular rest position were encouraged and the need for splint therapy was discussed and agreed by the patient. Silicone impressions with facebow and centric relation records were taken. Maxillary full-coverage stabilization splint with flat occlusal plane was applied which provided stable and uniform occlusal relationship to the opposing dentition [Figure 5]. It required 12–14 h of wear per day and was periodically adjusted every 2–4 weeks to compensate the changes of maxillary and mandibular relationships during the treatment. Balanced occlusion in centric relationship and absence of nonworking side interference on lateral and protrusive movements with the splint in place were emphasized at the end of each review visit. Active splint therapy was finished in 5 months with the maximum mouth opening increased from 28 mm to 34 mm, right lateral mandibular movement increased from 7 mm to 10 mm, and the left mandibular movement maintained at 11 mm. The patient experienced no pain on maximum mouth opening and lateral mandibular movement. No TMJ clicking or locking were recorded. These findings indicated that the internal derangement of left TMJ was resolved. The patient was then advised to continue wearing the splint and was referred back to the first author for orthodontic treatment 4 months after the end of active splint therapy after confirming that there was no further change in the malocclusion and the range of mandibular movement was satisfactory.

- Occlusal splint which was used in this report
Change of occlusion after splint therapy
The patient returned to the first author with the occlusal splint and the centric relation was registered. Molar relationship changed from half unit to full unit Class II; the overjet increased from 2 to 4.5 mm. The incomplete overbite was accentuated [Figure 6]. The occlusal interferences were located at upper first premolar and upper second molar regions [Figure 7].

- Occlusion of digital model (DDP-Ortho, Ortolab Sp. z o.o.) (a) before and (b) after splint therapy

- Occlusal contacts (a) before and (b) after splint therapy. Blue color indicates definite inter-occlusal contacts which were located at 17–47, 24–33 only after splint therapy
Treatment objectives
The digital model (DDP-Ortho, Ortolab Sp. z o.o.) after splint therapy was superimposed on the pretreatment lateral cephalogram and the lower model was rotated around the condyle with 2 mm of the upper and lower first molars’ vertical overlap to simulate the occlusion after 2 mm of the upper first molar intrusion [Figure 8 and Table 2]. The lateral cephalogram and digital model composite were transferred to the digital occlusogram software (True3D Occlusogram, IOSS GmbH)[7] for the construction of visual treatment objective (VTO) [Figure 9].[8] It served as a template to guide the tooth movement and assisted treatment planning by the construction of the digital occlusogram which will be explained in the next paragraph.

- Superimposition of digital model to the pretreatment lateral cephalogram with the lower model rotated around the condyle to simulate the occlusal change after 2 mm upper first molar intrusion
Upper incisors and extra-oral features
|
Occlusal plane
|
Occlusion
|
Condylar position
|

- Visual treatment objectives on digital occlusogram software (True3D Occlusogram, IOSS GmbH). Pretreatment upper and lower incisor positions after counterclockwise rotation of mandible by 2 mm intrusion of upper molars were indicated by red lines. Objective positions were indicated by green lines. Upper incisor required 3 mm intrusion and 10° uprighting which were measured at the incisal edge. Lower incisor required 3 mm proclination
Treatment alternatives
The patient declined combined surgical orthodontic treatment with surgical mandibular advancement and accepted orthodontic camouflage with skeletal anchorage. Biological limit [Table 3] was the most important consideration when formulating the VTO to confirm whether orthodontic camouflage was a feasible alternative to surgery. Since the overjet correction was produced by a combination of retraction of upper incisors, proclination of lower incisors, forward movement of the lower incisors, and the chin in response to counterclockwise rotation of mandible due to upper molar intrusion, dental movement should be planned with caution to avoid moving the teeth away from the dentoalveolar process. Violation of the biological limit might cause root resorption and gingival recession which indicates alternative measures such as modification of the treatment objectives and/ or rejecting orthodontic camouflage as a feasible option during treatment planning. On the other hand, planning and execution of mechanical tooth movement [Table 3] were also important as they allowed orthodontic tooth movement to achieve the objectives.[9] It was assisted using digital occlusogram [Figure 10] which revealed the space requirement and anchorage demand based on the VTO.
| Biological limit |
|---|
Alveolar process
|
Attached gingivae
|
| Mechanical tooth movement |
|---|
|
Space analysis and extraction plan
|
Anchorage analysis for extraction
|

- Digital occlusogram. Lines in red indicated objective arch form. Dots in green and red indicated contact points of incisors, canines, second premolars and molars. Dots in blue indicated mesial contacts of first molars. Upper first premolars were planned to be extracted. Quadrant 1 and 2 – first molars were allowed to move forward 3 mm, upper canines required 4 mm and 4.5 mm retraction on quadrants 1 and 2, respectively, which indicated moderate-to-maximum anchorage requirement. Quadrant 3 – lower left first molar has to protract 2 mm. Quadrant 4 – Lower right first molar has to retract 1.5 mm
Treatment progress
Leveling and alignment by straight wire mechanics
The patient was treated with 0.022” slot straight wire appliance (SmartClip™ SL3 Self-Ligating Bracket, 3M Oral care) in MBT™ prescription. The archwires were changed progressively from 0.014”, tandem 0.014” and 0.016”, 0.021” × 0.025” heat-activated NiTi to 0.019” × 0.025” stainless steel.
Alignment of 46 by segmented arch mechanics
Four-six was left out from banding at the initial stage. It was aligned separately with a 0.018” stainless steel wire activated in geometry V configuration[10] while the rest of the teeth were splinted by 0.019” × 0.025” stainless steel wire which served as an anchorage unit [Figures 11-13].

- Aligning 46 (dotted circle) with asymmetric V bend in geometry V by stainless steel 0.018” archwire. Other teeth in the arch were splinted together by stainless steel 0.019” × 0.025” archwire as anchorage

- (a) Force system of aligning 46 and 47 with straight wire in geometry II (b) Force system of aligning 46 with asymmetric V bend in geometry V while other teeth in the arch were splinted together as anchorage. The V bend was located between half and one-third of inter-bracket distance which was closer to 44. Well-defined active and anchorage units prevented 47 from displacement which might aggravate occlusal interferences

- (a) 46 (dotted circle) was aligned, lingual arch was installed (b) torquing arch (ART®, Atlanta Orthodontics) was installed for lingual root torque of upper incisors (c and d) retraction and intrusion of upper anterior segment and retraction of lower right dentition
Surgical placement of orthodontic miniscrews
When all the teeth were aligned with 0.019” × 0.025” stainless steel archwires, orthodontic miniscrews (ORLUSTM, Ortholution Co., Ltd.) were inserted at 16, 26, and 46 mesial buccal regions and 36 distal buccal region 7 mm from the archwire at the mucogingival junction (1O16107); 16 and 26 distal palatal regions 9 mm from the gingival margin (1O18208) and between upper and lower central incisors (1O14107) at the base of maxillary frenum insertion after frenectomy by diode laser (Ezlase™, Biolase) under local anesthesia.
Intrusion of upper dentition, retraction of upper incisors with lingual root torque, and space closure
Powerchains were applied from the miniscrews of 16 and 26 distal palatal regions to the lingual sheaths at 16 and 26 and lingual cleats at 17 and 27 for posterior intrusion. The lingual sheaths carried the transpalatal arch made by 0.036” stainless steel that counteracted the moments of the intrusion force which produced palatal crown torque at 16 and 26. Powerchain was applied from the miniscrew between upper central incisors to the archwire to intrude and procline the upper anterior teeth. To provide sufficient moment to move the root of upper incisors to the objective position, a torquing arch (ART®, Atlanta Orthodontics) was inserted. Proclination of incisors was prevented by retracting the upper incisors with powerchains which were applied from the miniscrews at 16 and 26 mesiobuccal regions to the crimpable extensions (DISCOpender 6.5X, BioMaterials Korea) located between the lateral incisors and canines [Figures 13 and 14].

- Appliance setup and force system for (a) retraction and intrusion of upper anterior segment (b-d) intrusion of upper posterior segment. The tendency for palatal tipping of 16 and 26 was prevented by the transpalatal arch. The tendency for palatal tipping of 17, 27 and 15, 25 was prevented by the moment of intrusion force produced by the buccal archwire which moved apically as it was connected to 16 and 26 during intrusion
Correction of lower midline by mesialization of lower molars on the left and distalization of lower molars on the right side
Distalization on the lower right dentition was done briefly by retracting the lower right anterior segment with powerchain from the discopender located between 42 and 43 to the miniscrew at 46 mesial buccal region. On the other hand, mesialization of the lower left dentition was done by activating a loop which was made by 0.017” × 0.025” β-titanium with a ligature wire connecting to the miniscrew at 36 distal buccal region [Figures 13, 15 and 16].

- (a) Transpalatal with hooks soldered at 15 and 25 region. Intrusion of 16, 26, 17, and 27 (b) Lower midline shift was corrected by the previous protraction of lower left and retraction of lower right dentition. (c and d) Upper incisor inclination was corrected

- Appliance setup and force system to (a) retract the dentition on the right and (b) protract the dentition on the left. The passive form of the protraction loop was drawn by the dotted line. The lines of force appliance which were indicated by the orientation of the powerchains were located very close to the centers of resistance of the dentition (blue dots). They reduced the tendency for the change of occlusal planes which might cause canting. (c and d) Spatial relationship changed between the miniscrew and 37 – the beta titanium loop was deactivated comparing panoramic radiographs taken (c) immediately after activation of the loop and (d) 6 months after. New bone (white arrows) had formed distal of 36 after 6 months of mesialization
Space closure with reciprocal anchorage
At the later stage of treatment, space closure was done by reciprocal anchorage between the posterior and anterior segments which allowed mesial drift of upper molars [Figure 17].

- (a) Retraction of 23 with a DISCOpender 468, BioMaterials Korea bonded on the palatal surface to reduce the friction during retraction (b) spaces appeared distal to 11 and 21 for composite buildup (c and d) 13 and 23 were retracted against 17 and 27 to open space distal to 12 and 22, close extraction spaces, and put buccal occlusion into Class I
Consultation of the second author at the finishing stage
The case was finished with 0.017” × 0.025” β-titanium with step down at 13 and 23 to provide optimum canine guidance. It was suggested by the second author who reviewed the patient regularly.
Treatment result
Total orthodontic treatment time was 36 months. The treatment result met the objectives. Molar relationship was finished into full unit Class II, canine relationship in Class I, and overjet changed from 4.5 mm at centric relation after splint therapy to 2.5 mm [Figure 18]. Upper incisor angulation changed from 82° to 101°. SNA and ANB reduced from 85° to 83° and 8° to 6°, respectively [Table 1]. Cephalometric superimposition revealed root uprighting of upper incisors, intrusion of upper dentition, and counterclockwise rotation of the mandible [Figures 19-22]. There was minimal amount of root resorption of upper incisors, and the right idiopathic condylar resorption lesion remained stable [Figure 23].

- Posttreatment extra- and intra-oral photographs

- Posttreatment lateral cephalogram

- Tracing of posttreatment lateral cephalogram

- Cephalometric superimposition of cephalograms on SN before splint therapy and orthodontics (blue) and after orthodontics (red). Condyle moved distally and caudally to centric relation which masked the effect of counterclockwise rotation of mandible due to upper molar intrusion

- Cephalometry superimposition on SN immediately after miniscrew placement (blue) and after orthodontics (red). The counterclockwise rotation of mandible around the condyle at centric relation in response to upper molar intrusion was revealed

- Posttreatment panoramic radiograph
Retention plan, composite buildups of 12 and 22, and postorthodontic occlusion equilibrium
A pair of vacuum-form suck-down retainers (Essix C+, Dentsply) was prescribed. The patient was instructed to wear them full time for the first 6 months and then continue with nighttime wear. Fixed retainers were bond on the upper and lower anterior teeth. Small composite occlusal platforms were incorporated into the fixed retainers at the upper incisors which lacked of prominent cingulum and marginal ridges to achieve solid and board interincisal contacts [Figure 24]. Composite buildups on 12 and 22 [Figures 25-27] and occlusion equilibrium were performed after debond by the second author.

- Fixed retainers on the upper arch with occlusal platforms built on upper incisors indicated by arrows

- Intraoral frontal view (a) before orthodontic treatment and (b) after orthodontic treatment and composite buildups

- Frontal view during smile (a) before orthodontic treatment and (b) after orthodontic treatment and composite buildups

- Three-quarter profile during (a) before orthodontic treatment and (b) after orthodontic treatment and composite buildups
Discussion
Importance of temporomandibular disorder management before orthodontic treatment
Orthodontics cannot cure temporomandibular disorder
The current evidences failed to establish a cause–effect relationship between occlusion (which included defective occlusal contacts and orthodontics) and TMD. Furthermore, orthodontic treatment could not cure or prevent TMD in any circumstances.[11] Therefore, the British Orthodontic Society[12] had given practical advices about the need of proper assessment of TMD and the importance of explaining to patients explicitly that orthodontic treatment only treats malocclusion but not TMD. TMD patients who seek or were receiving orthodontic treatment should be informed about the nature of TMD that the development and alleviations of signs and symptoms are seemingly random and options for management included appropriate referral to other specialties.
Stabilization splint is a valid option to manage temporomandibular disorder
Even though the causal relationship between defective contacts and TMD could not be established due to the lack of well-conducted randomized controlled trials, stabilization splint which is commonly used to eliminate unwanted occlusal interferences is, however, found to be useful in the improvement of signs and symptoms of TMD.[13]
Splint therapy is commonly used to reduce postural activity of masticatory muscles, alter the condyle–fossa relationship, eliminate TMJ pain and sounds, resolve restricted range of mandibular movement and internal derangement.[14] In addition, occlusal splint can protect teeth and associated structures from bruxism. Diagnostic information provided by occlusal splint for full-mouth prosthodontic rehabilitation cannot be ignored.[14-16] A study has shown that nocturnal occlusal splint is more effective to alleviate myogeneous pain, while patients with arthrogeneous pain can benefit from full-time application.[17]
The placebo effect of splint therapy was reported in various studies.[15,18] These clinical trials showed similar improvement of TMD when comparing patients with occlusal coverage splints to those with nonoccluding splints which is the placebo. It was shown that any kind of intraoral appliance can produce an effect on the masticatory muscle. For instance, nonoccluding splint therapy increases the awareness of jaw habits and tongue functioning position of TMD patients.[19] Change of palatal thickness of the splint can affect the improvement in myofascial pain dysfunction syndrome.[20] Nevertheless, other studies had shown better results in the elimination of signs and symptoms of TMD in patients with occlusal coverage splints than those with the placebo.[21,22]
Importance of preorthodontic splint therapy on orthodontic treatment planning
In general, most clinical studies had shown that splint therapy takes 10 weeks–12 months which concurred with the treatment time in our report.[15] Although wearing the splint 12 h a day up to a year can be a challenge to the patient, it is a good way to evaluate patient’s compliance for the subsequent orthodontic treatment.
Partial daily wear of occlusal splint is mostly recommended to reduce the risks of irreversible occlusal change from full-time wear of splint.[23,24] On the other hand, periodic adjustments of the splint to remove unwanted nonworking side interferences during laterotrusion and to provide balanced occlusion in centric relations are required to compensate the change in relationship between maxilla and mandible during treatment.[15] The result of periodic splint adjustments would improve mandibular movement, induce morphological alterations and remodeling in the joint structures, change the centric relation and hence the occlusion.[25] The resulting stable jaw relationship and change of occlusion affect the future orthodontic analysis and planning.
By revealing the true malocclusion, the clinicians can then evaluate and confirm any needs of orthognathic surgery for those patients. Furthermore, it can affect anchorage planning, extraction pattern, and position of miniscrew placement in orthodontic camouflage. The resulting stable jaw relationship after splint therapy will allow stable orthodontic treatment result. Therefore, there is medicolegal implication for inadequate preorthodontic TMD assessment and management as it may lead to incorrect treatment planning and hence adverse treatment results.
Psychosocial factors in temporomandibular disorder and orthodontic risk management
TMD has a significant negative impact on oral health-related quality of life such as its association with physical pain and psychologic discomfort.[26] For instance, patients with TMD had higher prevalence of psychological disorders such as anxiety or depression than the general population. Particularly, patients with disc displacement without reduction and limited mouth opening had higher psychosocial distress than the populations with disc displacement with reduction.[27] On the other hand, a study had illustrated that depression increases the risk of TMD, especially in female populations, and is associated with body dysmorphic disorder and obsessive-compulsive disorder.[28] Therefore, integration of mental health screening using questionnaires would be essential to clarify the nature of TMD.[29] Failure to identify the mental health problem could be detrimental to the management of TMD. This, in turn, could complicate the management of orthodontic patients in many ways such as treatment expectation, cooperation, compliance, and satisfaction of treatment outcome.
Proper referral for the management of TMD and its related conditions prior to orthodontic treatment is important for orthodontic risk management and achieving good standard of care.
Design and material of splint for the management of temporomandibular disorder
There are various designs of occlusal splints which are prescribed for eliminating signs and symptoms of masticatory dysfunction. Stabilization splint is the most common one which is an inter-occlusal device providing even occlusal contact to the opposing dentition. Another popular device is anterior repositioning splint which supports only anterior teeth occluding in protruded mandibular position. Compared to stabilization splint, anterior repositioning splint produces faster relief of signs and symptoms of internal derangement by recapturing the disc into the condylar fossa. However, it is recommended only for short-term usage as unwanted posterior openbite can occur over time. Stabilization splint demonstrated excellent response in clinical studies with complete recovery of internal derangement in many subjects.[16,30] Additionally, it seems to be more effective than anterior repositioning splint in internal derangement patients specifically with anterior disc displacement without reduction in long term.[31] As such, stabilization splint was prescribed to the patient in this case report. Other splint designs such as pivot splint, hydrostatic splint, and anterior and posterior bite planes had been described in the literatures. However, studies for those splint designs are minimal and long-term studies are required.[14,23]
Clinical reports had published the use of adhesive posterior bite blocks to maintain the splint-induced malocclusion during fixed orthodontic treatment.[32,33] However, it was not considered for our patient as the true malocclusion and the acquired mandibular position were stable over 4-month observation period before the orthodontic treatment.
Hard splints are mostly prescribed for TMD patients. They are either chemically cured or heat processed. It is adjustable with greater longevity and durability than soft splint.[23] On the other hand, soft splints are made from resilient material which has better comfort. However, they are difficult to repair and adjust. Additionally, soft splints cannot create even and stable contact to the opposing dentition.
Dual-laminated stabilization splint is a third variation to hard and soft splints which is considered to be a member of hard acrylic resin group.[23] It carries adjustable hard acrylic resin on the occlusal surface with a soft resilient inner layer which provides good fitting and optimal comfort to the supporting teeth. Therefore, dual-laminated design will become an important trend for the management of TMD.
Specific considerations in orthodontic mechanics in patients with previous temporomandibular disorder
Single tooth with large displacement: Clear differentiation between active and anchorage unit to prevent skewing of arch form which creates new interferences
Alignment of 46 which was rotated distolingually posed a challenge to the anchorage of 47. If a piece of straight wire runs between 46 and 47, the bracket wire interaction could result in geometry 2 relationship. The resulting mesial lingual rotation and lingual crown tipping of 47 may introduce new occlusal interference. This is the reason why 46 was left out at the initial stage of leveling and alignment. Splinting the rest of the teeth together with 0.019” × 0.025” served as an anchorage unit during the alignment of 46 which reduced the possible side effect of creating new interference. Four-six was aligned separately with an overlay 0.018” stainless wire activated in geometry V. It produced a force system which tipped the crown buccally and derotated it in a distobuccal direction which was consistent with the treatment objective [Figures 12 and 13].
Intrusion of upper dentition eliminated posterior interference, reduced overjet, and provided more bone volume for uprighting upper incisors
Due to the occlusal interferences located at the second molar region after extraction of upper first premolars, intrusion of upper molars was required. It produced counterclockwise rotation of the mandible which reduced the overjet and made the orthodontic camouflage feasible as it prevented excessive proclination of lower incisors and retraction of upper incisors. Furthermore, intrusion of upper incisors put the roots in the wider part of the funnel-shaped dentoalveolar process. It allowed more root uprighting to take place without moving the root away from the palatal cortex which violated the biological limit [Figures 14, 15 and 22].
Mesialization of lower left and distalization of lower right dentition corrected lower midline instead of using intermaxillary elastics
Inter-maxillary elastics is commonly used to correct midline deviation with the side effect of canting of the occlusal plane. To correct a lower midline shift to the left, the force system extrudes the upper right and lower left molars and incisors which rotates the upper and lower occlusal planes in counterclockwise direction (Roll) with inter-occlusal contacts maintained. In this case, since the upper dentition was being retracted and intruded by miniscrew anchorage, the extrusion of upper molars was prevented. On the right side, it can induce posterior openbite as the upper molar extrusion is not allowed to maintain inter-occlusal contact in response to the counterclockwise rotation (Roll) of lower occlusal plane. On the left side, the extrusion of lower molars is allowed as it is not hindered by the skeletal anchorage. It prevents counterclockwise (Pitch) rotation of mandible to take place. Therefore, mesialization of the lower left and distalization of the lower right dentition with miniscrew anchorage were used with the lines of force appliance applied as close to the center of resistance as possible to prevent canting from happening [Figure 16].
Limitation of orthodontic tooth movement: Occlusal adjustment and postorthodontic restoration may be required
Since occlusal interferences may induce a recurrence of TMD, good occlusion in terms of proper canine guidance, evenly distributed posterior and anterior inter-occlusal loadings are important to aim for which are easily overlooked by the orthodontist and difficult to be achieved by orthodontic treatment solely. For instance, lack of well-defined anatomical features such as worn cusp tips, poorly restored dental restorations with defective marginal ridges and anatomical occlusal grooves, and morphological anomalies such as talon cusps could prevent the achievement of excellent occlusion details. Furthermore, specific tooth movements which are requested by the prosthodontist to optimize the occlusion can induce new interferences at the anchorage unit at the finishing stage which is undesirable. Therefore, postorthodontic occlusal equilibrium and restorations may be indicated. In this case, since the upper lateral incisors were peg shaped and the central incisors were thin due to erosion and lack of anatomically well-defined cingulum and marginal ridges, the teeth were aligned into the best positions in relation to the alveolar bone and lip support while minimal intervention with composite resin buildups on peg-shaped lateral incisors and distal surfaces of central incisors were undertaken. Furthermore, the solid inter-occlusal contacts of upper incisors were achieved by the composite bite platforms which were incorporated into the fixed retainers. It was then followed with occlusal equilibrium performed by the second author [Figures 24].
Conclusion
Temporomandibular joint examination by an orthodontist revealed signs and symptoms which led to the referral to a prosthodontist. Preorthodontic splint therapy alleviated signs and symptoms of TMD and revealed the true malocclusion which facilitated orthodontic treatment planning. With the guidance of digital visual treatment objective (VTO) and occlusogram, orthodontic camouflage with miniscrew anchorage with specific considerations in mechanics for patients with previous TMD, composite buildups, and occlusal equilibrium were performed to achieve the planned objectives with good result.
Acknowledgment
We would like to thank Dr. Edmond, H. N. Pow, Clinical Associate Professor in Prosthodontics for his advice on the manuscript.
Declaration of patient consent
The authors certify that they have obtained the appropriate patient consent form. In the form the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that her name and initials will not be published and due efforts will be made to conceal her identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Prevalence of mandibular dysfunction and relation between malocclusion and mandibular dysfunction in a group of women in Sweden. Eur J Orthod. 1983;5:115-23.
- [CrossRef] [PubMed] [Google Scholar]
- Association between malocclusion and temporomandibular disorders in orthodontic patients before treatment. J Orofac Pain. 1993;7:156-62.
- [Google Scholar]
- The effect of maxillary first premolar extraction and incisor retraction on mandibular position: Testing the central dogma of “functional orthodontics”. Am J Orthod Dentofacial Orthop. 1992;101:4-12.
- [Google Scholar]
- TMD in relation to malocclusion and orthodontic treatment. Angle Orthod. 2007;77:542-8.
- [CrossRef] [Google Scholar]
- Orthodontics. Part 7: Fact and fantasy in orthodontics. Br Dent J. 2004;196:143-8.
- [CrossRef] [PubMed] [Google Scholar]
- Perception of the relationship between TMD and orthodontic treatment among orthodontists. Dental Press J Orthod. 2015;20:45-51.
- [CrossRef] [PubMed] [Google Scholar]
- The “3-D occlusogram” software. Am J Orthod Dentofacial Orthop. 1999;116:363-8.
- [CrossRef] [Google Scholar]
- Bioprogressive Therapy. Denver, Colo: Rocky Mountain/Orthodontics; 1979.
- Biomechanics in Orthodontics. Wollerau, Switzerland: International Orthodontic School and Services; 2014.
- Orthodontics for treating temporomandibular joint (TMJ) disorders. Cochrane Database Syst Rev. :CD006541.
- [Google Scholar]
- Temporomandibular Disorders (TMDs) and Orthodontic Patient.
- Evaluation of different occlusal splints and counselling in the management of myofascial pain dysfunction. J Oral Rehabil. 2009;36:79-85.
- [CrossRef] [PubMed] [Google Scholar]
- Occlusal appliance therapy in patients with temporomandibular disorders. A double-blind controlled study in a short-term perspective. Acta Odontol Scand. 1998;56:122-8.
- [Google Scholar]
- Use and effectiveness of splint appliance therapy: Review of literature. Cranio. 1997;15:159-66.
- [CrossRef] [Google Scholar]
- A comparison of the success of 24-hour occlusal splint therapy versus nocturnal occlusal splint therapy in reducing craniomandibular disorders. J Cranio Disord Winter. 1992;6:64-70.
- [Google Scholar]
- Conventional and nonoccluding splint therapy compared for patients with myofascial pain dysfunction syndrome. Gen Dent. 1987;35:502-6.
- [Google Scholar]
- Splint therapy for the myofascial pain – Dysfunction (MPD) syndrome: A comparative study. J Am Dent Assoc. 1972;84:624-8.
- [Google Scholar]
- Effect of a thick palatal appliance on muscular symptoms in craniomandibular disorders: A preliminary study. Cranio. 2001;19:42-7.
- [Google Scholar]
- The treatment of painful temporomandibular joint clicking with oral splints: A randomized clinical trial. J Am Dent Assoc. 2006;137:1108-14.
- [Google Scholar]
- Efficiency of occlusal appliance therapy in secondary otalgia and temporomandibular disorders. Acta Odontol Scand. 2002;60:248-54.
- [Google Scholar]
- Oral appliances in the management of temporomandibular disorders. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;107:212-23.
- [CrossRef] [PubMed] [Google Scholar]
- Side effects of stabilization occlusal splints: A report of three cases and literature review. Cranio. 2010;28:128-35.
- [Google Scholar]
- Treatment outcome of appliance therapy in temporomandibular disorder patients with myofascial pain after 6 and 12 months. Acta Odontol Scand. 2004;62:343-9.
- [CrossRef] [PubMed] [Google Scholar]
- Oral health-related quality of life in patients with temporomandibular disorders. J Oral Facial Pain Headache. 2015;29:231-41.
- [CrossRef] [PubMed] [Google Scholar]
- Can a 10-minute questionnaire identify significant psychological issues in patients with temporomandibular joint disease? J Oral Maxillofac Surg 2017
- [Google Scholar]
- Associations in the longitudinal course of body dysmorphic disorder with major depression, obsessive-compulsive disorder, and social phobia. J Psychiatr Res. 2006;40:360-9.
- [Google Scholar]
- Integration of mental health screening in the management of patients with temporomandibular disorders. Br J Oral Maxillofac Surg. 2017;55:594-99.
- [Google Scholar]
- A short-term evaluation of the effectiveness of stabilization-type occlusal splint therapy for specific symptoms of temporomandibular joint dysfunction syndrome. J Prosthet Dent. 1989;61:610-3.
- [CrossRef] [Google Scholar]
- Conservative therapy in patients with anterior disc displacement without reduction using 2 common splints: A randomized clinical trial. J Oral Maxillofac Surg. 2005;63:1295-303.
- [Google Scholar]
- Treatment of a mandibular functional shift in an adolescent boy with temporomandibular disorder and crossbites. Am J Orthod Dentofacial Orthop. 2015;148:660-73.
- [Google Scholar]
- An adult case of TMJ osteoarthrosis treated with splint therapy and the subsequent orthodontic occlusal reconstruction: Adaptive change of the condyle during the treatment. Am J Orthod Dentofacial Orthop. 2000;118:566-71.
- [Google Scholar]




