

Translate this page into:
Cervical vertebral anomalies in patients with obstructive sleep apnea
Address for correspondence: Dr. Saugat Ray, Orthodontics and Dentofacial Orthopedics, FDC, Fort, Mumbai, Maharashtra, India. E-mail: saugat.ray@rediffmail.com
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Objective
The aim of this study was to find an association between the patients with obstructive sleep apnea (OSA) and with cervical vertebral anomalies and any further correlation between various anomalies with varying severities of OSA.
Materials and Methods
The sample consisted lateral cephalograms of 70 subjects who were diagnosed with OSA and 70 other orthodontic patients who were selected as a control group. The lateral radiographs of both cases and controls were traced and findings were recorded.
Results
In total, 21.42% of subjects in the OSA group and 8.57% in the control group were affected with cervical vertebrae anomalies. The statistical analysis reveals that the number of subjects affected with cervical vertebrae anomalies in OSA group is highly significant. A number of cases of fusion were higher than posterior arch deficiency in OSA group and equal in the control group. However, in both the groups, the number of cases with two vertebrae fusion was higher. Further, the higher number of two vertebrae fusion cases in OSA group was found to be statistically significant. The findings of one-way ANOVA for OSA cases reveals the number of cases affected with cervical vertebrae anomalies were statistically highly significant (P < 0.01) in severe cases of OSA.
Conclusion
Patients of cervical vertebral anomalies may be at higher risk of developing OSA, and the possibility of the presence of cervical vertebral anomalies may increase with the increase in the severity of OSA. The most common vertebral anomaly was found to be two vertebral fusions.
Keywords
Cervical vertebral anomalies
cervical vertebral morphology
obstructive sleep apnea

INTRODUCTION
Obstructive sleep apnea (OSA) is a common medical condition characterized by loud snoring, arousals, sleep fragmentation, intermittent hypoxemia, and daytime sleepiness.[1] The repetitive blockade of airflow in patients with OSA results in recurrent episodes of hypoxia and frequent arousals, which leads to sleep fragmentation.[2,3] OSA commonly affects the adult population and is more prevalent in males aged 60 years and above.[4-6] The patients affected with this condition are at high risk of developing cardiovascular and other systemic complications which further leads to increased morbidity and mortality.[7-10]
Sonnesen et al.[11] had shown that the patients of OSA do have an increased the prevalence of cervical vertebral anomalies, especially fusion anomalies. The cervical vertebral anomalies had also been shown to be significantly associated with craniosynostosis syndromes and cleft lip and palate cases.[12,13] These associations of OSA with limited cervical vertebral movements due to various anomalies may have diagnostic implications and may provoke the future researchers to understand the pathophysiology of sleep apnea better.
With this background, this study has been designed with an aim and objectives to:
Find an association between patients with OSA and cervical vertebral anomalies.
To evaluate any correlation between various anomalies with varying severities of OSA.
MATERIALS AND METHODS
The study sample consisted lateral cephalograms of 70 subjects (44 males and 26 females) who were diagnosed with OSA based on patients’ symptoms, clinical evaluation, and polysomnography. The mean age of the patients selected for the study was 38.9 ± 3.3. The lateral cephalograms of 70 patients (35 males and 35 females) were also collected as a control group. These were the adult patients who visited for orthodontic treatment in the department. The mean age of the subjects selected in the control group was 36.7 ± 4.2. The inclusion criteria of subjects considered for control group were as follows:
Patients are not having any craniofacial anomalies.
Patients with negative history of any sleep disorder.
Patients without any significant medical or surgical history.
Patients with skeletal class I morphology and average growth pattern.
These lateral cephalograms were collected from Orthodontic Department of a Tertiary Care Government Hospital over a period of 7 years. All lateral cephalograms of these patients were taken by a single professional technician using the standard techniques in such a way that the radiographs included the images of patients’ face down from the supraorbital region involving all the cervical vertebrae.
The lateral radiographs of both cases and controls were traced on an acetate sheet and various cervical anomalies, if any, were recorded.
RESULTS
The lateral cephalograms of total 140 people were traced and analyzed. The entire data are shown in Tables 1 and 2. In total, 21.42% of subjects in the OSA group and 8.57% in the control group were affected with cervical vertebrae anomalies. Z-test was performed, and it was found that the number of subjects affected with cervical vertebrae anomalies in OSA group was highly signifi cant in comparison to control group. The prevalence of fusion group of anomalies was relatively higher than posterior arch defi ciency group in patients affected with OSA. Among fusion group, two vertebrae fusion anomalies were found to be predominantly higher as compared to other variants of fusion anomalies in both experimental and control groups [Table 1].
| Condition type | Experimental group (n = 70) | Control group (n = 70) | P | ||
|---|---|---|---|---|---|
| Affected | P | Affected | P | ||
| Total | 15 | 0.001 (VHS) | 06 | NS (0.13) | 0.03 (S) |
| PAD | 06 | HS (0.013) | 03 | NS (0.83) | 0.12 (NS) |
| Spina bifda | 02 | NS (0.159) | 01 | NS (0.321) | |
| Dehiscence | 04 | NS (0.045) | 02 | NS (0.159) | |
| Fusion | 09 | NS (0.102) | 03 | NS (0.83) | 0.36 (NS) |
| Two vertebrae | 06 | HS (0.013) | 03 | NS (0.83) | |
| Block fusion | 02 | NS (0.159) | — | — | |
| Occipitalization | 01 | NS (0.321) | — | — | |
The signifcance criteria are NS, S <0.05, HS <0.01, VHS <0.001 based on a = 5%, that is, CI of 95%. NS – Nonsignificant; S – Significant; HS – Highly significant; VHS – Very highly significant; CI – Confdence interval; PAD: Posterior arch defciency; OSA: Obstructive sleep apnea
| Condition type | AHI score 5-15 (n = 23) | AHI score 15-30 (n = 19) | AHI score >30 (n = 28) | |||
|---|---|---|---|---|---|---|
| Affected | P | Affected | P | Affected | P | |
| Total | 02 | — | 04 | — | 09 | <0.01 (HS) (0.049) |
| PAD | 01 | 0.00 | 01 | 0.049 | 04 | <0.05 (S) (0.01) |
| Spina bifda | 01 | 0.00 | — | — | 01 | NS (0.150) |
| Dehiscence | — | — | 01 | 0.049 | 03 | NS (0.106) |
| Fusion | 01 | 0.00 | 03 | 0.000 | 05 | <0.001 (VHS) (0.000) |
| Two vertebrae | 01 | 0.00 | 01 | 0.049 | 04 | <0.01 (HS) (0.001) |
| Block fusion | — | — | 01 | 0.049 | 01 | NS (-) |
| Occipitalization | — | — | 01 | 0.049 | — | NS (-) |
The signifcance criteria are NS, S <0.05, HS <0.01, VHS <0.001 based on a=5%, that is, CI of 95%. NS – Nonsignificant; S – Significant; HS – Highly significant; VHS – Very highly significant; CI – Confdence interval; PAD: Posterior arch defciency; OSA: Obstructive sleep apnea; AHI – Apnea-hypopnea index
The OSA group was further divided into mild moderate and severe cases depending upon their apnea-hypopnea index (AHI). The fi ndings were compiled and one-way ANOVA was performed. The total number of all the variants of cervical vertebrae anomalies were found to be highest in patients with AHI scoring >30 as compared to other OSA groups [Table 2]. The prevalence of two vertebrae fusions was found to be highly signifi cant as compared to other variants of fusion anomalies irrespective of AHI scoring of the patients affected with OSA.
The distribution of various cervical vertebrae anomalies in both control and OSA group are shown in Figures 1 and 2. The distribution of various types of anomalies in OSA group is shown in Figure 3.

- Obstructive sleep apnea group

- Control group
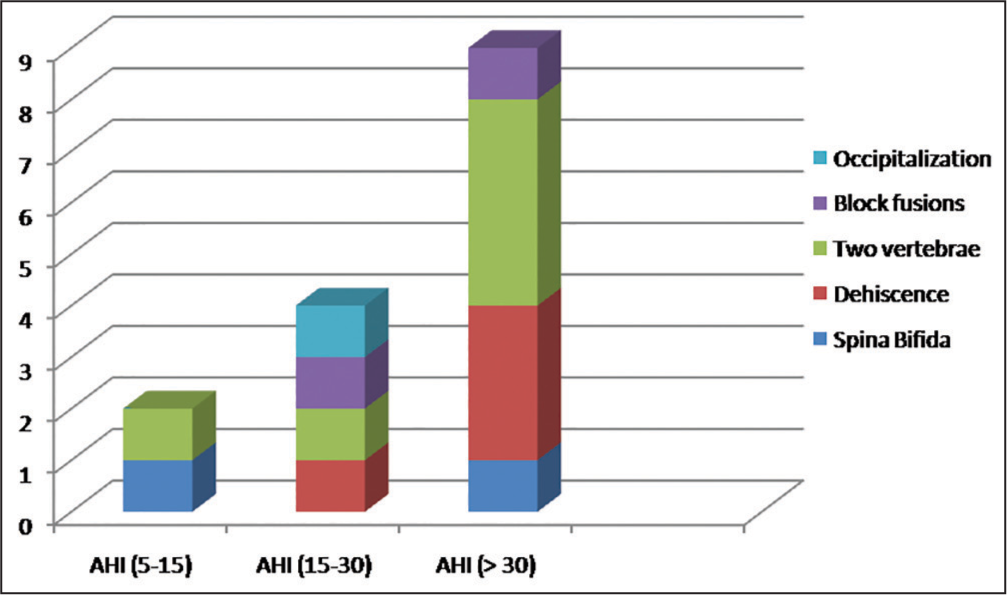
- Distribution of cervical vertebral anomalies in obstructive sleep apnea group
DISCUSSION
The obesity and associated soft tissue enlargement of the upper respiratory tract may contribute as a potential threat for the development of OSA, but nevertheless the role of skeletal abnormalities of cranio maxillofacial region can be ruled out. Sakakibara et al. advocated the bony structure discrepancies may be the dominant contributing factors for OSA, especially in nonobese patients.[14] The present study focused primarily on the association of various anomalies, especially pertaining to cervical vertebrae with OSA. Although the previous studies had shown a higher prevalence of cervical vertebrae anomalies in patients with OSA but the sample size of the control group was low as compared to the study group.[11] In the present study, the samples for the control group were carefully selected with age group almost similar as a study group and the sample size equal to OSA group. The age and gender differences between the individuals in both the groups were found to be statistically nonsignificant.
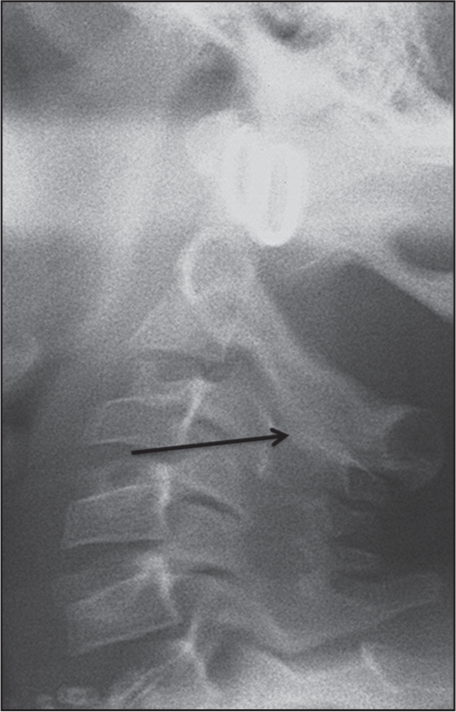
Although the cervical anomalies were located in both the groups but the prevalence was signifi cantly higher in OSA group. The cases of two vertebrae fusions [Figure 4] in both experimental and control groups were mostly located in C2, C3, C4, and C5 regions. The prevalence of two vertebrae fusions was higher in caudal regions with 83% of cases in OSA group involved C4 and C5. Two cases of block fusions [Figure 5] involved C2, C3, and C4. One case of occipitalization was the partial assimilation of the anterior arch of an atlas with the anterior rim of foramen magnum [Figure 6]. Two cases of spina bifi da in OSA group involved atlas and C3, but the one located in control group involved C2 [Figure 7]. All the cases of dehiscence [Figure 8] were seen in either C2 or C3 vertebrae with C3 being more prevalent in 67% of cases.

- Two vertebrae fusion
- Block fusion

- Occipitalization

- Spina bifida

- Dehiscence
The incidental fi nding of cervical vertebrae anomalies in orthodontic patients during their pretreatment evaluation of lateral cephalogram may indicate the requirements of a thorough evaluation of the upper respiratory tract even in the absence of any relevant medical history. The present study not only proves the association of the two conditions but also provokes for further research in sleep disorders for better understanding of the pathophysiology of OSA.
CONCLUSION
Keeping in view of the results derived from this study, it can be concluded that:
Patients of cervical vertebral anomalies may be at higher risk of developing OSA.
The possibility of the presence of cervical vertebral anomalies increases with the increase in severity of OSA.
The most common vertebral anomaly was found to be two vertebral fusions.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Pathophysiology of sleep apnoea In: Sullivan CE, Saunders NA, eds. Sleep and Breathing (2nd ed). New York: Marcel Decker; 1994. p. :405-88.
- [Google Scholar]
- Complications and consequences of obstructive sleep apnea. Curr Opin Pulm Med. 2000;6:485-9.
- [Google Scholar]
- Epidemiology of obstructive sleep apnea: A population health perspective. Am J Respir Crit Care Med. 2002;165:1217-39.
- [Google Scholar]
- Predictors and prevalence of obstructive sleep apnoea and snoring in 1001 middle aged men. Thorax. 1991;46:85-90.
- [Google Scholar]
- Sleep and aging: 1. Sleep disorders commonly found in older people. CMAJ. 2007;176:1299-304.
- [Google Scholar]
- Increased incidence of cardiovascular disease in middle-aged men with obstructive sleep apnea: A 7-year follow-up. Am J Respir Crit Care Med. 2002;166:159-65.
- [Google Scholar]
- Hemostatic alterations in patients with obstructive sleep apnea and the implications for cardiovascular disease. Chest. 2003;124:1956-67.
- [Google Scholar]
- Obstructive sleep apnea: Implications for cardiac and vascular disease. JAMA. 2003;290:1906-14.
- [Google Scholar]
- Case control study of cerebrovascular damage defined by magnetic resonance imaging in patients with OSA and normal matched control subjects. Sleep. 2001;24:715-20.
- [Google Scholar]
- Cervical column morphology in adult patients with obstructive sleep apnoea. Eur J Orthod. 2008;30:521-6.
- [Google Scholar]
- Cervical spine anomalies in the craniosynostosis syndromes. Cleft Palate J. 1987;24:328-33.
- [Google Scholar]
- Cervical vertebral anomalies in cleft lip and palate. Cleft Palate J. 1986;23:206-14.
- [Google Scholar]
- Cephalometric abnormalities in non-obese and obese patients with obstructive sleep apnoea. Eur Respir J. 1999;13:403-10.
- [Google Scholar]




