

Translate this page into:
Bonded maxillary expander in growing patients with or without unilateral cleft lip and palate: How does it influence transversal and vertical dentoskeletal changes?

*Corresponding author: Fabrizia d’Apuzzo, Multidisciplinary Department of Medical-Surgical and Dental Specialties, University of Campania Luigi Vanvitelli, Naples, Italy. fabriziadapuzzo@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Nucci L, Piccirillo M, d’Apuzzo F, Simeon V, Grassia V, Adel SM. Bonded maxillary expander in growing patients with or without unilateral cleft lip and palate: How does it influence transversal and vertical dentoskeletal changes? APOS Trends Orthod. doi: 10.25259/APOS_280_2024
Abstract
Objectives
Growing patients with unilateral cleft lip and palate (UCLP) usually show maxillary retrusion with constricted upper arch. Thus, orthodontic treatment with maxillary expansion is often needed. This study aimed to evaluate transversal and vertical changes in patients with or without UCLP after maxillary expansion.
Material and Methods
This observational retrospective study included patients aged between 7 and 14 years, with UCLP (test group) or without cleft lip and palate (controls), constricted upper arch and normodivergent growth pattern treated with a bonded maxillary expander. Patients with craniofacial syndromes, previous orthodontic treatment, or incomplete records were excluded. The digital dental casts and lateral radiographs of the head before (T0) and after treatment (T1) were collected and digitized by scanning with the 3ShapeTRIOS®. Statistical analysis was performed with STATA software. The Chi-square test was used for sex data in the two groups, and evaluation of the differences between the two groups was performed with the independent samples. P < 0.05 was considered statistically significant.
Results
The study sample included 51 patients (10.0 ± 2.5 years), 21 patients with UCLP, and 30 patients as the control group. Before treatment, all the transversal values measured on the maxillary arch at the occlusal and gingival level, as well as the length of the arch, presented statistically significant differences between the two groups with P < 0.05. The comparison at T1 did not show significant differences between the two groups for the transversal values, except for the value measured between the second premolars at the gingival level (P < 0.05). The cephalometric values measured in the analysis in the two groups did not show a statistically significant difference, except for the I-SN who showed significant differences both at T0 and T1 due to the presence of previous scars in UCLP patients.
Conclusion
The UCLP group showed an improvement in all transverse diameters after treatment with the bonded maxillary expander without affecting the mandibular divergence and incisor inclination.
Keywords
Unilateral cleft lip and palate
Constricted upper arch
Bonded maxillary expander
Digital dental casts
Cephalometry

INTRODUCTION
The cleft lip and palate (CLP) is the most frequently encountered malformation of the facial region with a multifaceted etiology involving environmental, genetic, and epigenetic factors interacting among them, i.e., smoking, bad habits, air pollution during pregnancy, specific genes, and microRNA mutations.[1-4] Many orofacial structures, including the lips and the palate, derive from the first pharyngeal arches. The pathogenic processes occur between the 4th and 12th week of gestation when the medial nasal and maxillary processes in the primary palate or the palatal units in the secondary palate fail to fusion.[5,6] Oral cleft can be unilateral or bilateral if one or both sides are interested, and patients with CLP show different malformations, including aesthetical defects of the face[7] and of the smile with a higher prevalence of dental anomalies.[8-10] Moreover, these subjects may have difficulty in speaking and uttering a lot of phonetic sounds due to the possible presence of velopharyngeal defects,[11-13] conductive hearing loss due to elevated air conduction,[14] reduced upper airway dimensions and sleeping disorders.[15]
Thus, these malformations need interdisciplinary treatment from birth until adulthood.[8,16,17]
The treatment of children with CLP consists of a first surgery performed at around 4 or 6 months of age for functional reconstruction of the nasolabial area, following the functional cheilorhinoplastic technique of Markus et al.[18] Soft palate surgery is usually performed at 12 months, while hard palate surgery at around 18 months. A secondary alveolar bone graft is usually planned when the patient is 9–12 years old.[19-21]
A significant decrease in vertical and sagittal facial dimensions in surgically treated patients with unilateral CLP (UCLP) was detected during mixed dentition in comparison to noncleft children.[22] Recent research also showed that the occlusion was more affected when the surgery for the hard palate closure was delayed.[21]
In any case, to improve the growth of the maxilla in width and length, it is necessary to monitor the occlusion and intervene with an early orthodontic treatment.[8] Specifically, the orthopedic treatment of maxillary expansion aims to improve both dentoskeletal occlusions, although not reaching the size of the upper arch as in healthy patients,[23,24] as well as the hearing of the middle ear, breathing, and other oral functions.[14,15,25,26]
Another usual skeletal problem of patients affected by CLP and constricted upper arch is maxillary retrusion due to the cleft and the scars due to the surgical treatment of the hard palate in childhood, often resulting in a Class III malocclusion. In these cases, the early orthopedic treatment should also include therapies aimed at increasing maxillary diameters and controlling mandibular protrusion[27-30] also improving the soft tissues.[31-33]
There are many types of expansion devices and protocols based on different activation modes. The Haas and Hyrax expanders were both efficient for the correction of dentoskeletal crossbite and did not show significant differences in the size increase of the upper dental arch in patients with CLP. [34,35]
Pugliese et al. 2020 used three different devices in patients with full bilateral cleft lip and palate: Hyrax, quad-helix, and differential opening expander. The data showed similar changes in the size of the maxillary dental arch with the three appliances and only with hyrax, the arch morphology was not changed.[36]
There are different activation protocols, i.e., rapid maxillary expansion (RME), slow maxillary expansion, and mixed maxillary expansion.[23,25,37] The expansion of the maxilla was found to be efficient, with no statistically significant differences both in terms of width and perimeter of the upper arch and in the three-dimensional morphology of the palate in patients with bilateral CLP treated with slow or rapid activation.[25,38,39]
The hybrid activation of the expander has shown good results in increasing the transverse tooth and skeletal dimensions, causing fewer dental side effects than magnetic resonance imaging[37,40-42] and in a recent publication carried out at the Orthodontic Program of the University of Campania Luigi Vanvitelli, a sample of patients with CLP were treated in mixed dentition with a McNamara bonded maxillary expander, using hybrid activation.[43] The changes in the upper arch after the treatment were detected on three-dimensional digital models by a laser scanner, demonstrated as an even more effective and reliable method than measurements made directly on the plaster models.[44]
The main purpose of this observational retrospective study is to evaluate changes in the diameters of the upper arch after treatment with a bonded maxillary expander and mixed activation protocol on digital dental models in growing patients with and without UCLP. The secondary objective will be the comparison before and after the treatment of cephalometric variables in the same sample to investigate the sagittal dentoskeletal effects of this type of expansion.
MATERIAL AND METHODS
The sample data were collected from the database of the Orthodontic Program of the University of Campania Luigi Vanvitelli, Naples, Italy, from March 2020 to April 2023. The study was made by the Declaration of Helsinki and approved by the Ethical Committee of the University of Campania Luigi Vanvitelli, Naples, Italy (Prot. N°147). The parents of each child involved in the study signed an informed consent for the use of personal data. The inclusion criteria were patients with non-syndromic UCLP, age range between 7 and 14 years, a constricted upper arch, a cervical vertebral maturation stage between CS1 and CS4, and treatment protocol including a bonded maxillary expander with mixed activation.[37,42,43] Patients with other craniofacial syndromes, with previous orthodontic treatment, or incomplete documentation were excluded. All patients had been previously treated in the Maxillofacial Surgery and Oral Units at the University of Campania Luigi Vanvitelli, Naples, Italy, by the same surgical protocol: A first lip surgery performed between 4 and 6 months, soft palate surgery is usually performed at 12 months while hard palate surgery at around 18 months.
All included patients had undergone an initial orthodontic checkup in mixed dentition [Figure 1] and were treated with a McNamara bonded palatal expander extended from the anteriorly deciduous canines and the first permanent molars,[8,43] an acrylic resin shower in the lower arch, class III elastics and chin cup.[45,46] The expansion protocol envisaged a hybrid activation with a first phase of chairside activation (four laps, two laps after 20–30 min, and a last lap after 10–15 min) and a second phase at home with one lap every 3 days.[40,42] The subjects underwent a follow-up every 2 weeks, and the therapy ended when an overcorrection of about 2 mm was obtained. After the active expansion period, the screw of the appliance was blocked with acrylic composite, and the expander was used as retention for about 8 months [Figure 2].[43] Patients with UCLP were considered the sample group, while subjects without UCLP were as controls.

- Initial intraoral photographs of a patient in mixed dentition with unilateral cleft lip and palate (T0).

- Intraoral photographs and panoramic X-ray after treatment (T1).
The initial (T0) and after maxillary expansion (T1) plaster models of each patient were collected and digitized by scanning with the 3ShapeTRIOS® with a manufacturing inaccuracy of <20 microns (www.3shape.com).[44] The digital models were exported in STL format and imported into the Viewbox 4 software (dHal Software, Kifissia, Greece) to carry out the measurements by the expert operators themselves [Figure 3].[43,47] Supplementary Tables 1 and 2 described the reference points and measurements, respectively, used to perform the analysis of digital dental models.
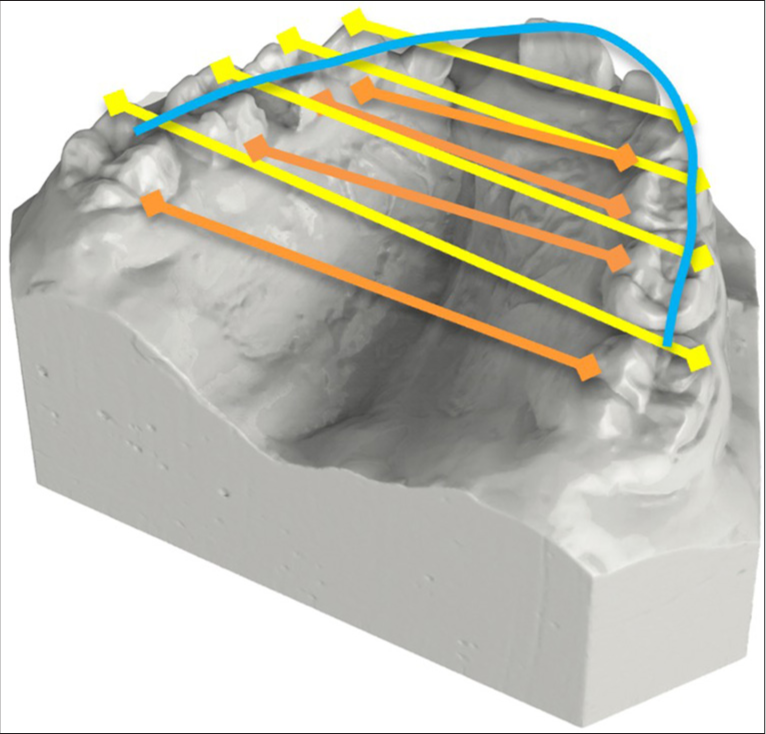
- Digital dental casts of the upper arch with transverse diameters and arch length (yellow: occlusal plane, orange: gingival plane, blue: arch lenght at occlusal plane).
| Variables | Overall | UCLP | Control | P |
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | ||
| Year | 10.0 (2.5) | 10.8 (3.2) | 9.4 (1.8) | 0.061 |
| 3–3 OC | 29.0 (5.8) | 25.6 (7.4) | 31.3 (2.5) | <0.001** |
| 3–3 G | 23.4 (5.2) | 20.5 (6.4) | 25.5 (2.6) | <0.001** |
| 4–4 OC | 35.8 (8.4) | 30.5 (10.7) | 39.5 (2.8) | <0.001** |
| 4–4 G | 24.3 (6.5) | 20.2 (7.9) | 27.1 (3.1) | <0.001** |
| 5–5 OC | 42.3 (4.3) | 39.5 (4.0) | 44.3 (3.3) | <0.001** |
| 5–5 G | 28.3 (4.0) | 26.1 (3.5) | 29.9 (3.6) | <0.001** |
| 6–6 OC | 50.4 (8.3) | 46.8 (11.3) | 52.9 (3.9) | 0.008* |
| 6–6 G | 32.0 (5.9) | 29.8 (7.8) | 33.6 (3.3) | 0.022* |
| AL OC | 86.9 (19.3) | 75.5 (25.9) | 94.8 (4.7) | <0.001** |
UCLP: Unilateral cleft lip and palate, SD: Standard deviation, OC: occlusal plane, G: gingival plane, AL OC: Arch Lenght at the occlusal plane. * and ** mean the level of statistical significance.
| Variables | UCLP | Non-UCLP | Group difference | |||||
|---|---|---|---|---|---|---|---|---|
| Pre | Post | Difference | Pre | Post | Difference | b (95% CI) | P | |
| mean (SD) | _ | |||||||
| 3–3 OC | 25.6 (7.4) | 30.8 (8.6) | 5.3 (3.0) | 31.3 (2.5) | 35.6 (2.1) | 4.3 (2.5) | 0.94 (−0.84; 2.72) | 0.29 |
| 3–3 G | 20.5 (6.4) | 25.2 (8.0) | 4.7 (3.1) | 25.5(2.6) | 29.8 (2.5) | 4.2 (3.0) | 0.33 (−1.70; 2.37) | 0.75 |
| 4–4 OC | 30.5 (10.7) | 36.4 (12.9) | 5.9 (3.4) | 39.5 (2.8) | 46.1 (3.2) | 6.6 (2.9) | 0.48 (−1.54; 2.50) | 0.64 |
| 4–4 G | 20.2 (7.9) | 25.7 (10.0) | 5.5 (3.3) | 27.1 (3.1) | 33.3 (2.9) | 6.2 (3.1) | −0.19 (−2.34; 1.96) | 0.86 |
| 5–5 OC | 39.5 (4.0) | 46.9 (4.6) | 7.4 (2.1) | 44.3 (3.3) | 51.6 (3.3) | 7.3 (2.6) | −0.62 (−2.27; 1.04) | 0.46 |
| 5–5 G | 26.1 (3.5) | 32.9 (4.5) | 6.8 (2.5) | 29.9 (3.6) | 37.5 (3.0) | 7.6 (2.7) | −1.68 (−3.33; −0.03) | 0.046* |
| 6–6 OC | 46.8 (11.3) | 52.5 (13.1) | 5.8 (3.5) | 52.9 (3.9) | 60.3 (4.0) | 7.4 (3.3) | −1.26 (−3.32; 0.80) | 0.23 |
| 6–6 G | 29.8 (7.8) | 35.6 (9.7) | 5.8 (3.6) | 33.6 (3.3) | 41.1 (3.7) | 7.5 (3.2) | −1.53 (−3.58; 0.52) | 0.14 |
| AL OC | 75.5 (25.9) | 78.5 (26.3) | 2.9 (5.5) | 94.8 (4.7) | 99.7 (6.4) | 4.9 (4.5) | −2.05 (−5.35; 1.25) | 0.22 |
b: Difference between groups, CI: Confidence interval, UCLP: Unilateral cleft lip and palate, SD: Standard deviation, OC: occlusal plane, G: gingival plane, AL OC: Arch Lenght at the occlusal plane. * means level of statistical significance.
The Viewbox software was used to carry out the cephalometric analysis, establishing standard parameters to be adopted for the measurements and eliminating the operator-dependent error of measurement. The collection of cephalometric data was carried out before expansion (T0) and after expansion (T1) in both groups of patients.
The following values were measured: The sella-nasion with mandibular plane angle (SNGoMe), the Frankfort-mandibular plane angle (FMA), the incisor mandibular plane angle (IMPA), the Frankfort-mandibular incisor angle (FMIA), and the maxillary incisor with sella-nasion angle (I^SN).
Data analysis
Continuous variables were reported as means and standard deviations if the data distribution was normal or as medians and interquartile ranges if the data showed a skewed distribution. The Shapiro–Wilk test was used to evaluate normality assumption. Analysis of continuous variables and comparison between groups (two categorical variables) was performed using Student’s t-test.
Linear regression models were performed to evaluate the association between T1 evaluation (as dependent variable) and groups, adjusting for information at baseline (diff at T1 = groups + diff at baseline). Beta coefficients and 95% confidence intervals (β) have been calculated for all models.
P < 0.05 was considered statistically significant. All analyses were performed using statistical software STATA v18 (StataCorp. 2023. College Station, TX: StataCorp LLC).
RESULTS
The total study sample included 51 patients (mean age: 10.0 ± 2.5 years). Of these, 21 patients from the UCLP group, including 11 females and 10 males, and 30 patients from the control group, including 19 females and 11 males. The initial mean age of the UCLP group was 10.8 ± 3.2 years, while the mean initial age of the control group was 9.4 ± 1.8 years with a P = 0.061, therefore, with a non-significant difference between the two groups at T0. The total phase of expansion treatment (T0 - T1) lasted 1.8 ± 0.8 years in the UCLP group and 1.1 ± 0.34 years in the control group.
Before treatment (T0), all the transversal values measured on the maxillary arch at the occlusal and gingival level, as well as the length of the arch, presented statistically significant differences between the two groups with P < 0.05 [Table 1], in particular in the anterolateral areas.
The comparison between T0 and T1 did not show statistically significant differences between the two groups at the diameters of the arches, both at the level of the cusp tips and at the gingival level, except for the value measured between the second premolars at the gingival level (P < 0.05) [Table 2].
The cephalometric values measured before and after treatment in the two groups did not show any statical significance, except for the I-SN value that showed significant differences both at T0 and T1 due to the previous scar tissue both at T0 and T1 in patients with UCLP [Table 3].
| Variables | UCLP | Non-UCLP | P |
|---|---|---|---|
| mean (SD) | mean (SD) | ||
| SNGoMe | 37.6 (3.7) | 35.1 (4.7) | 0.046 |
| FMA | 26.6 (4.0) | 24.3 (5.0) | 0.082 |
| IMPA | 87.4 (4.0) | 86.8 (7.1) | 0.72 |
| FMIA | 66.3 (5.6) | 68.9 (7.2) | 0.18 |
| I-SN | 91.2 (9.8) | 108.6 (7.3) | <0.001 |
UCLP: Unilateral cleft lip and palate, SD: Standard deviation, SNGoMe: The sella-nasion with mandibular plane angle, FMA: the Frankfort-mandibular plane angle, IMPA: the incisor mandibular plane angle, FMIA: the Frankfort-mandibular incisor angle, I^SN: the maxillary incisor with sella-nasion angle.
DISCUSSION
Several studies in the literature have highlighted the maxillary morphogenetic varieties, in mixed or permanent dentition, in patients with cleft lip and palate compared to control groups before different types of orthopedic/orthodontic treatment.[47,48] In particular, the distances between the upper canines were found to be significantly reduced in some studies both at the coronal and gingival level; thus, the expansion of the upper jaw in patients with cleft lip and palate is often requested treatment in subjects during the maxillary growth phase.[22,49,50]
The expansion of the maxilla produces various positive effects in patients with UCLP, including not only the improvement of occlusion with an increase in the transverse diameters and the correction of the cross-bite, where present[21,51] but also the resolution of other breathing, hearing, and language issues often associated with the UCLP, thanks to the enlargement of the nasal airways, the improvement of hearing in the middle ear,[14,15,26] and of speech by facilitating movements of the tongue in the increased oral cavity space.[13,48,52] Furthermore, the improvement in facial esthetics that results from the enlargement of the middle third of the face should not be underestimated.[52]
Most patients with CLP have a diagnosis of constricted and retruded maxilla due to scar residues, resulting from previous surgery to close the lip and palate, that negatively affect the growth of the maxilla concerning the mandible. Therefore, the orthopedic/orthodontic treatment before the pubertal peak is indicated to reduce the discrepancies between the mandible and maxilla.[53] Many studies have evaluated dental and alveolar changes in patients with uni or bilateral cleft lip and palate using different devices and expansion protocols. In the study of Ayub et al., the RME produced similar effects in both groups, except arch length and palate depth which were less developed in patients with CLP.[23]
In our study, patients with constricted and retruded maxillary arch with and without UCLP were included to compare the post-maxillary expansion data, all presenting similar maxillary retrusion and contraction associated with mandibular protrusion. Other authors in previous studies have used other types of maxillary expansion with different types of expanders and activation protocols.[23,25,35,36] In this study, a bonded maxillary expander (McNamara type) with hybrid activation of the expansion screw was used for the 1st time in association with early therapy for class III malocclusion, which also includes lower Splint, Class III intermaxillary elastics and Chincup, protocol defined with the acronym of SEC III modified due to the presence of the expansion screw in the upper splint[45,46] to treat transverse, sagittal, and vertical problems simultaneously. Hoefert et al. also included class III patients treated with Delaire expansion and facial mask, and this showed clear improvements in facial esthetics with an improvement in soft tissues in a three-dimensional analysis.[33] Our results showed improvements in all transversal dimensions of the upper arch and the total arch length. The bonded expander eliminates possible interference with the lower arch thanks to the presence of smooth acrylic splints that cover the occlusal surface. This implies that the expander bonded together with the hybrid activation protocol should be adopted in UCLP as a procedure between the slow and rapid protocol to obtain an efficient maxillary expansion.[43] This also leads to avoiding buccal tipping of premolars and molars, ensuring adequate activation.[25,38]
This study, of course, showed some limitations such as the retrospective nature of the study design and short-term collected results. The stability of orthodontic–orthopedic treatment over time can be threatened by the presence of scar residues due to primary surgery, the lack of palatal support bone, abnormal muscle forces, and highly representative orthodontic tooth movements. In recent years, several studies have been performed on the stability of the transverse dimension after treatment in patients with CLP. Li and Lin have demonstrated how the use of retention spans to maintain the results obtained in long-term re-evaluations.[54] Patients with CLP, 1 year after the expansion and implant-prosthetic treatment in adulthood, had less stability and less volume and surface of the palate than healthy patients.[55]
A new perspective for diagnosis, treatment planning, and monitoring could be the use of intraoral scanners during clinical routines in offices and hospitals in assessing dentofacial and nasolabial morphology in cleft patients; also useful to better communicate with the affected patients and their families.[56] Therefore, future aims could be the evaluation of the airway volumes and the influence of tongue position and movement before and after treatment in a wide sample, as performed in previous studies using a different oral appliance in patients with CLP.[57,58]
Moreover, it could be relevant to evaluate the long-term stability during adulthood of the treatments performed in mixed dentition with the palatal expander in comparison to matched control groups without CLP.
CONCLUSION
The results of this study showed that growing subjects with UCLP show an improvement in all transverse diameters and the length of the upper arch after treatment with a bonded expander and hybrid activation measured on digital dental models. No statistically significant differences were revealed in the mandibular divergence before and after treatment in both groups. The comparison of treatment outcomes in the two groups did not show relevant differences except for upper central incisor inclination, which resulted in more retroclined in patients with UCLP due to previous surgery for treating the cleft during the 1st year of age.
Ethical approval
The research/study approved by the Institutional Review Board at the University of Campania Luigi Vanvitelli, number Protocol N° 147, dated 2021.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- The complex genetics of cleft lip and palate. Eur J Orthod. 2004;26:7-16.
- [CrossRef] [PubMed] [Google Scholar]
- Salivary microRNAs as new molecular markers in cleft lip and palate: A new frontier in molecular medicine. Oncotarget. 2018;9:18929-38.
- [CrossRef] [PubMed] [Google Scholar]
- Maternal exposure to ambient air pollutant and risk of oral clefts in Wuhan, China. Environ Pollut. 2018;238:624-30.
- [CrossRef] [PubMed] [Google Scholar]
- Rare genetic variants in SEC24D modify orofacial cleft phenotypes. medRxiv [Preprint]; 2023
- [CrossRef] [Google Scholar]
- Diagnostic accuracy of fetal MRI to detect cleft palate: A meta-analysis. Eur J Pediatr. 2020;179:29-38.
- [CrossRef] [PubMed] [Google Scholar]
- Delaire's cheilorhinoplasty: Unilateral cleft aesthetic outcome scored according to the EUROCLEFT guidelines. Int J Pediatr Otorhinolaryngol. 2006;70:463-8.
- [CrossRef] [PubMed] [Google Scholar]
- Interdisciplinary approach for a patient with unilateral cleft lip and palate. Am J Orthod Dentofacial Orthop. 2018;153:883-94.
- [CrossRef] [PubMed] [Google Scholar]
- Dental anomalies in different types of cleft lip and palate: Is there any relation? J Craniofac Surg. 2018;29:1316-21.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of dental anomalies in the patient with cleft lip and palate visiting a tertiary care hospital. JNMA J Nepal Med Assoc. 2020;58:591-6.
- [CrossRef] [PubMed] [Google Scholar]
- Association between velopharyngeal function and dental-consonant misarticulations in children with cleft lip/palate. Br J Plast Surg. 2001;54:290-3.
- [CrossRef] [PubMed] [Google Scholar]
- Psychological effects of speech disorders in an adult patient with untreated cleft palate. Niger J Med. 2007;16:381-3.
- [CrossRef] [PubMed] [Google Scholar]
- Speech outcome in unilateral complete cleft lip and palate patients: A descriptive study. Eur J Paediatr Dent. 2014;15:293-6.
- [Google Scholar]
- Effects of maxillary expansion on hearing and voicefunction in non-cleft lip palate and cleft lip palatepatients with transverse maxillary deficiency: Amulticentric randomized controlled trial. Braz J Otorhinolaryngol. 2021;87:315-25.
- [CrossRef] [PubMed] [Google Scholar]
- Three-dimensional nasal septum and maxillary changes following rapid maxillary expansion in patients with cleft lip and palate. Angle Orthod. 2020;90:672-9.
- [CrossRef] [PubMed] [Google Scholar]
- Cleft lip and palate patients: Diagnosis and treatment In: Almasri MA, ed. Designing strategies for cleft lip and palate care. London: InTech; 2016. p. :23-42.
- [CrossRef] [Google Scholar]
- Speech outcomes after palatal closure in 3-7-year-old children. Braz J Otorhinolaryngol. 2022;88:594-601.
- [CrossRef] [PubMed] [Google Scholar]
- Primary closure of cleft palate: A functional approach. Br J Oral Maxillofac Surg. 1993;31:71-7.
- [CrossRef] [PubMed] [Google Scholar]
- Secondary alveolar bone grafting using autologous versus alloplastic material in the treatment of cleft lip and palate patients: Systematic review and meta-analysis. Prog Orthod. 2019;20:6.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of rapid maxillary expansion in unilateral cleft lip and palate patients after secondary alveolar bone grafting: Review and case report. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;114:e25-30.
- [CrossRef] [PubMed] [Google Scholar]
- Do infant cleft dimensions have an influence on occlusal relations? A subgroup analysis within an RCT of primary surgery in patients with unilateral cleft lip and palate. Cleft Palate Craniofac J. 2020;57:378-88.
- [CrossRef] [PubMed] [Google Scholar]
- Facial profile and maxillary arch dimensions in unilateral cleft lip and palate children in the mixed dentition stage. Eur J Dent. 2017;11:76-82.
- [CrossRef] [PubMed] [Google Scholar]
- Analysis of the maxillary dental arch after rapid maxillary expansion in patients with unilateral complete cleft lip and palate. Am J Orthod Dentofacial Orthop. 2016;149:705-15.
- [CrossRef] [PubMed] [Google Scholar]
- Relapse tendency in maxillary arch width in unilateral cleft lip and palate patients with different maxillary arch forms. Cleft Palate Craniofac J. 2008;45:278-83.
- [CrossRef] [PubMed] [Google Scholar]
- Slow versus rapid maxillary expansion in bilateral cleft lip and palate: A CBCT randomized clinical trial. Clin Oral Investig. 2017;21:1789-99.
- [CrossRef] [PubMed] [Google Scholar]
- Rapid maxillary expansion effects of nasal airway in children with cleft lip and palate using computational fluid dynamics. Orthod Craniofac Res. 2019;22:201-7.
- [CrossRef] [PubMed] [Google Scholar]
- Rapid maxillary expansion treatment in patients with cleft lip and palate: A survey on clinical experience in the European cleft centers. J Clin Med. 2023;12:3159.
- [CrossRef] [PubMed] [Google Scholar]
- Craniofacial growth analysis of individuals with and without cleft lip and palate in Colombia. Cleft Palate Craniofac J. 2022;59:577-88.
- [CrossRef] [PubMed] [Google Scholar]
- Retrognathic maxilla in individuals born with oral clefts is due to intrinsic factors and not only due to early surgical treatment. Angle Orthod. 2021;91:243-7.
- [CrossRef] [PubMed] [Google Scholar]
- Biomechanics of maxillary expansion and protraction in Class III patients. Am J Orthod Dentofacial Orthop. 2002;121:582-3.
- [CrossRef] [PubMed] [Google Scholar]
- A prospective study of the short-term treatment effects of the acrylic-splint rapid maxillary expander combined with the lower Schwarz appliance. Angle Orthod. 2005;75:7-14.
- [Google Scholar]
- 3D soft tissue changes in facial morphology in patients with cleft lip and palate and class III malocclusion under therapy with rapid maxillary expansion and delaire facemask. J Orofac Orthop. 2010;71:136-51.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of rapid maxillary expansion in cleft patients resulting from the use of two different expanders. Dental Press J Orthod. 2016;21:82-90.
- [CrossRef] [PubMed] [Google Scholar]
- Transverse effect of Haas and Hyrax appliances on the upper dental arch in patients with unilateral complete cleft lip and palate: A comparative study. In: Dental Press J Orthod. Vol 19. 2014. p. :39-45.
- [CrossRef] [PubMed] [Google Scholar]
- Dental arch size and shape after maxillary expansion in bilateral complete cleft palate: A comparison of three expander designs. Angle Orthod. 2020;90:233-8.
- [CrossRef] [PubMed] [Google Scholar]
- Upper and lower arch changes after Mixed Palatal Expansion protocol. Eur J Paediatr Dent. 2014;15:375-80.
- [Google Scholar]
- Analysis of the dentoalveolar effects of slow and rapid maxillary expansion in complete bilateral cleft lip and palate patients: A randomized clinical trial. Clin Oral Investig. 2016;20:1837-47.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of maxillary expansion on the maxillary arch width in patients with bilateral cleft palate: A review. Children (Basel). 2023;10:762.
- [CrossRef] [PubMed] [Google Scholar]
- Dento-skeletal effects of mixed palatal expansion evaluated by postero-anterior cephalometric analysis. Eur J Paediatr Dent. 2014;15:59-62.
- [Google Scholar]
- Comparison between rapid and mixed maxillary expansion through an assessment of dento-skeletal effects on posteroanterior cephalometry. Prog Orthod. 2014;15:46.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison between rapid and mixed maxillary expansion through an assessment of arch changes on dental casts. Prog Orthod. 2015;16:20.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of upper arch changes in patients with unilateral cleft lip and palate after maxillary expansion using digital dental cast. Stoma Edu J. 2020;7:184-90.
- [CrossRef] [Google Scholar]
- Intra-arch dimensional measurement validity of laser-scanned digital dental models compared with the riginal plaster models: A systematic review. Orthod Craniofac Res. 2015;18:65-76.
- [CrossRef] [PubMed] [Google Scholar]
- Paediatric orthodontics part 4: SEC III protocol in Class III malocclusion. Eur J Paediatr Dent. 2019;4:330-4.
- [Google Scholar]
- Modified SEC III protocol: Vertical control related to patients' compliance with the Chincup. Eur J Orthod. 2021;43:80-5.
- [CrossRef] [PubMed] [Google Scholar]
- Three-dimensional evaluation of the maxillary arch and palate in unilateral cleft lip and palate subjects using digital dental casts. Eur J Orthod. 2017;39:641-5.
- [CrossRef] [PubMed] [Google Scholar]
- Three-dimensional morphology of the palate in subjects with unilateral complete cleft lip and palate at the stage of permanent dentition. Cleft Palate Craniofac J. 2004;41:416-23.
- [CrossRef] [PubMed] [Google Scholar]
- Maxillary anterior tooth size and arch dimensions in unilateral cleft lip and palate. Cleft Palate Craniofac J. 2008;45:639-46.
- [CrossRef] [PubMed] [Google Scholar]
- Early assessment of dental arch development in repaired unilateral cleft lip and unilateral cleft lip and palate versus controls. Cleft Palate Craniofacial J. 2005;42:385-91.
- [CrossRef] [PubMed] [Google Scholar]
- Biomechanical effects of rapid palatal expansion on the craniofacial skeleton with cleft palate: A three-dimensional finite element analysis. Cleft Palate Craniofac J. 2007;44:149-54.
- [CrossRef] [PubMed] [Google Scholar]
- Speech assessment in cleft palate patients: A descriptive study. Int J Pediatr Otorhinolaryngol. 2009;73:641-4.
- [CrossRef] [PubMed] [Google Scholar]
- 3D comparison of dental arch stability in patients with and without cleft lip and palate after orthodontic/rehabilitative treatment. J Appl Oral Sci. 2019;27:e20180434.
- [CrossRef] [PubMed] [Google Scholar]
- Dental arch width stability after quadhelix and edgewise treatment in complete unilateral cleft lip and palate. Angle Orthod. 2007;77:1067-72.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of dental arch stability after orthodontic treatment and oral rehabilitation in complete unilateral cleft lip and palate and non-clefts patients using 3D stereophotogrammetry. BMC Oral Health. 2020;20:154.
- [CrossRef] [PubMed] [Google Scholar]
- Exploring the potential applications of intraoral scanners in the treatment of cleft lip and palate deformity-A scoping review of literature. J World Fed Orthod. 2024;13:265-78.
- [CrossRef] [PubMed] [Google Scholar]
- Three-dimensional assessment of airway volumes in patients with unilateral cleft lip and palate. Prog Orthod. 2021;22:35.
- [CrossRef] [PubMed] [Google Scholar]
- The effect of tongue appliance on the nasomaxillary complex in growing cleft lip and palate patients. J Indian Soc Pedod Prev Dent. 2006;24:136-9.
- [CrossRef] [PubMed] [Google Scholar]




