

Translate this page into:
Clear aligners for Class III malocclusion and severe open bite camouflage: A case report


*Corresponding author: Dr. Francesca Cremonini, Postgraduate School of Orthodontics, University of Ferrara, Italy. dr.ssafrancescacremonini@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Cremonini F, Guiducci D, Palone M, Lombardo L. Clear aligners for Class III malocclusion and severe open bite camouflage: A case report. APOS Trends Orthod. 2024;14:64-9. doi: 10.25259/APOS_76_2023
Abstract
The aim of the study was to describe a clinical case of a Class III malocclusion and severe open bite approached with clear aligners (CAs) and intermaxillary elastics. A 21-year-old male patient showed to the dental clinic asking for orthodontic treatment. His chief complaint was an unpleasant smile esthetics. The patient showed an oval face with increased length of the lower third of the face, slight mandibular asymmetry, and concave profile. On intraoral evaluation, a bilateral canine and molar Class III with reduced overbite could be seen. Pre-treatment panoramic radiograph showed good root parallelism and presence of all dental elements. Cephalometric values confirmed skeletal Class III (Wits Appraisal = −6.5 mm), increased vertical dimension (FMA = 34.3°), correctly inclined upper incisors and retroclined lower incisors. After discussing the treatment options with the patient, CAs (F22, Sweden and Martina, Due Carrare, Padova, Italy) were chosen to approach this malocclusion together with intermaxillary elastics. After 9 months of active treatment involving 18 sets of aligners, the patient showed correct overbite, bilateral canine e molar Class I, leveled and aligned dental arches, and no signs of radicular or bone resorption. Cephalometric parameters show control of vertical dimension (FMA = 34.4°), upper incisor flaring and lower incisor retroclination, and signs of a dentoalveolar compensation. Careful diagnosis, treatment planning, and clinical management of CAs and intermaxillary elastics led to a successful dentoalveolar compensation featured by good occlusal results, bilateral Class I relationship, and normal overbite which remained stable after 1 year from the end of treatment.
Keywords
Class III
Clear aligners
Open bite
Intermaxillary elastics
Long-term follow-up

INTRODUCTION
Orthodontists face significant challenges when treating Class III malocclusion, specifically in case of adult hype rdivergent. In this last case, careful biomechanical planification is required to obtain good treatment results. As a matter of fact, the use of Class III elastics may produce an extrusion of upper molars and a clockwise rotation of the mandibular plane resulting in a worsening of vertical dimension.[1]
Clear aligners (CAs) represent one option available to camouflage moderate Class III malocclusion maintaining a good vertical control.[2]
The objective of this case report is to describe an adult male patient with Class III malocclusion and anterior open bite (AOB) successfully treated with CAs and intermaxillary elastics.
CASE REPORT
A 21-year-old male patient came to the dental clinic asking for improvement of his smile esthetics. He received a previous orthopedic and orthodontic treatment in another dental clinic.
From extraoral examination an oval face, a slight left chin deviation, increased vertical dimension, centered upper midline, and a straight profile could be observed [Figure 1].
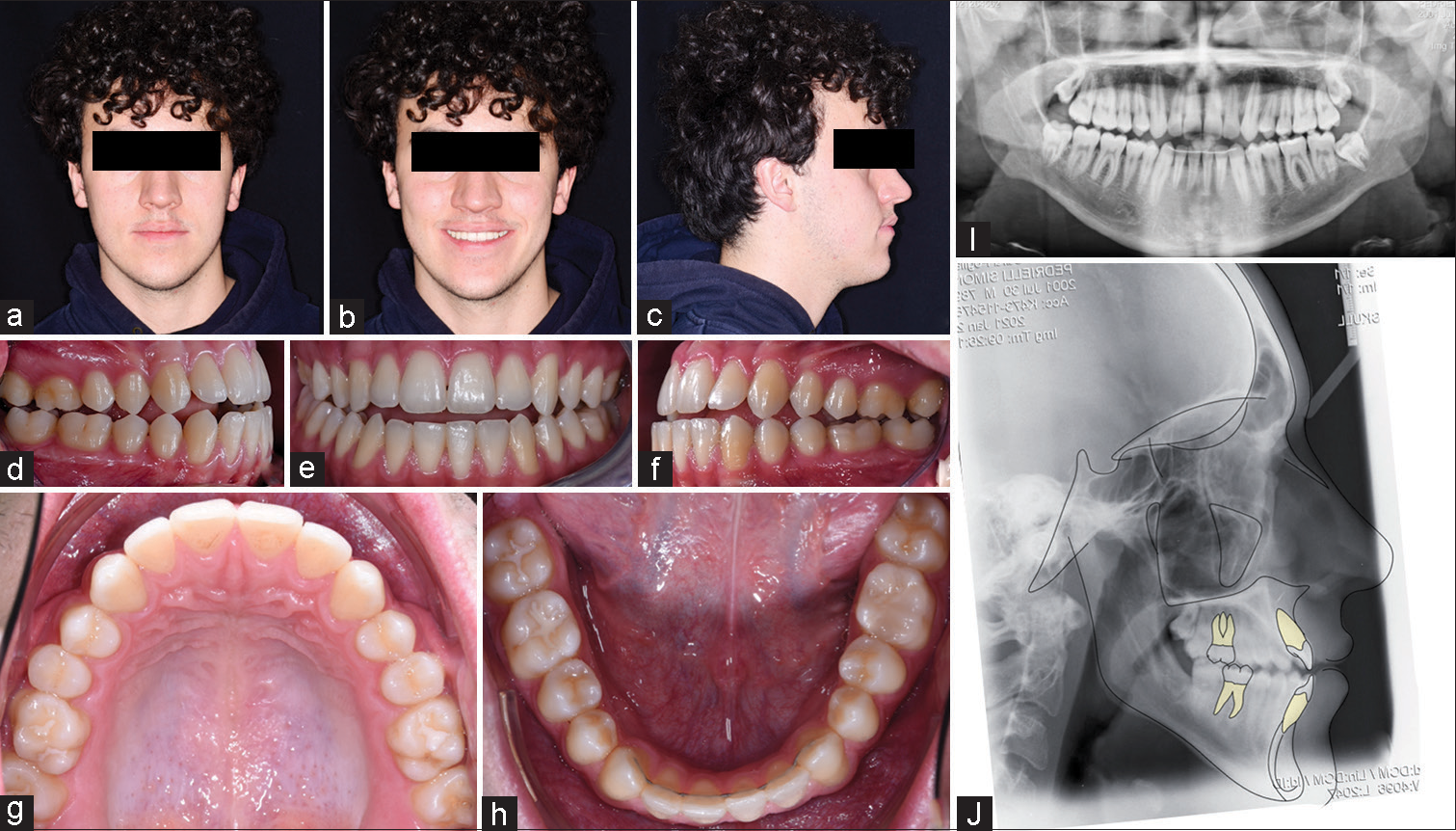
- (a-c) initial extraoral, (d-h) intraoral photos, (i)panoramic X-ray and (j) lateral cephalogram.
Intraoral pictures showed a correct transverse dimension of the maxilla, centered upper and lower midlines, AOB, bilateral molar and canine Class III, and aligned and leveled upper and lower arch [Figure 1].
The initial radiographs showed the presence of all dental elements, good radicular angulation, Skeletal Class III malocclusion (Wits Appraisal = −6.5 mm), increased vertical dimension (Angle between mandibular plane and Frankfurt plane [FMA] = 34.4), correctly positioned upper incisors ( Inclination of upper incisors with respect to palatal plane [U1-PP] = 113.1), and retroclined lower incisors (Lower incisor inclination with respect to mandibular plane [IMPA] = 87.3) [Figure 1 and Table 1].
| Normal values | Pre-treatment values | Post-treatment values | |
|---|---|---|---|
| Horizontal skeletal | |||
| SNA (°) | 82±3.5 | 81.7 | 79.5 |
| SNB (°) | 80±3.0 | 80.6 | 79.4 |
| ANB (°) | 2.0±2.4 | 1.1 | 0.1 |
| Maxillary skeletal (A-Na Perp) (mm) | 1.0±3.1 | −1.4 | 0.2 |
| Mandibular skeletal (Pg-Na Perp) (mm) | −2.0±5.3 | −2.0 | 2.9 |
| Wits appraisal (mm) | −1±1 | −6.5 | −5.0 |
| Vertical skeletal | |||
| FMA (MP-FH) (°) | 26±5.0 | 34.3 | 34.4 |
| MP-SN (°) | 33±6.0 | 41.3 | 45.0 |
| Palatal-mandibular angle (°) | 28±6.0 | 37.1 | 39.0 |
| Palatal-occlusal plane (°) | 10±4.0 | 13.4 | 10.8 |
| Mandibular plane to occlusal plane (°) | 18.6±5.0 | 23.7 | 28.5 |
| Mx occlusal plane (MxOP-Na Perp) (°) | 95±1.4 | 100.5 | 95.9 |
| Anterior dental | |||
| U-Incisor protrusion (U1-Apo) (mm) | 6±2.2 | 5.2 | 6.6 |
| L1-protrusion ([L1-Apo] (mm) | 1±2.3 | 5.4 | 4.3 |
| U1-palatal plane (U1-PP) (°) | 110±5.0 | 113.1 | 117.0 |
| U1-occlusal plane (°) | 59±7.0 | 53.5 | 52.1 |
| L1-occlusal plane (°) | 72±5.0 | 68.9 | 72.5 |
| IMPA (°) | 95±7.0 | 87.3 | 79.1 |
SNA: Angle between Sella-Nasion-A point, SNB: Angle between Sella-Nasion-B point, ANB: Angle between A point-Nasions-B point, MP-FH: Angle between mandibular plane and Frankfurt Plane, MP-SN: Angle between mandibular plane and Sella Nasion line, IMPA: Lower incisor inclination with respect to mandibular plane, FMA: Angle between mandibular plane and Frankfurt plane, U1-PP: Inclination of upper incisors with respect to palatal plane
Treatment objectives
The objectives of the treatment were to obtain a bilateral Class I dental occlusion and a normalization of overjet and overbite, with the improvement of smile esthetics.
Treatment alternatives
Due to the complexity of the malocclusion, the ideal treatment plan would have been a combined surgical-orthodontic approach. As the patient refused it, a camouflage treatment was then considered, as dentoalveolar values were favorable for dental compensation. Fixed multi-bracket appliance or CAs could have been used to improve the malocclusion. As a good control of vertical dimension was required, with just crown tipping movements needed and the demand of the patient to use an aesthetic appliance, CAs were chosen.
Treatment progress
Digital set up was performed to improve the overbite, and to obtain a Class I molar and canine relationship. Therefore, teeth movement was planned resembling the effects of Class III elastics: Upper incisor slight extrusion and proclination, lower incisor retroclination, distal tipping of lower teeth for Class III correction, and slight upper molar intrusion.
Grip points with a beveled form were needed and bonded on upper and lower teeth both for stabilization and extrusion movements [Figure 2].
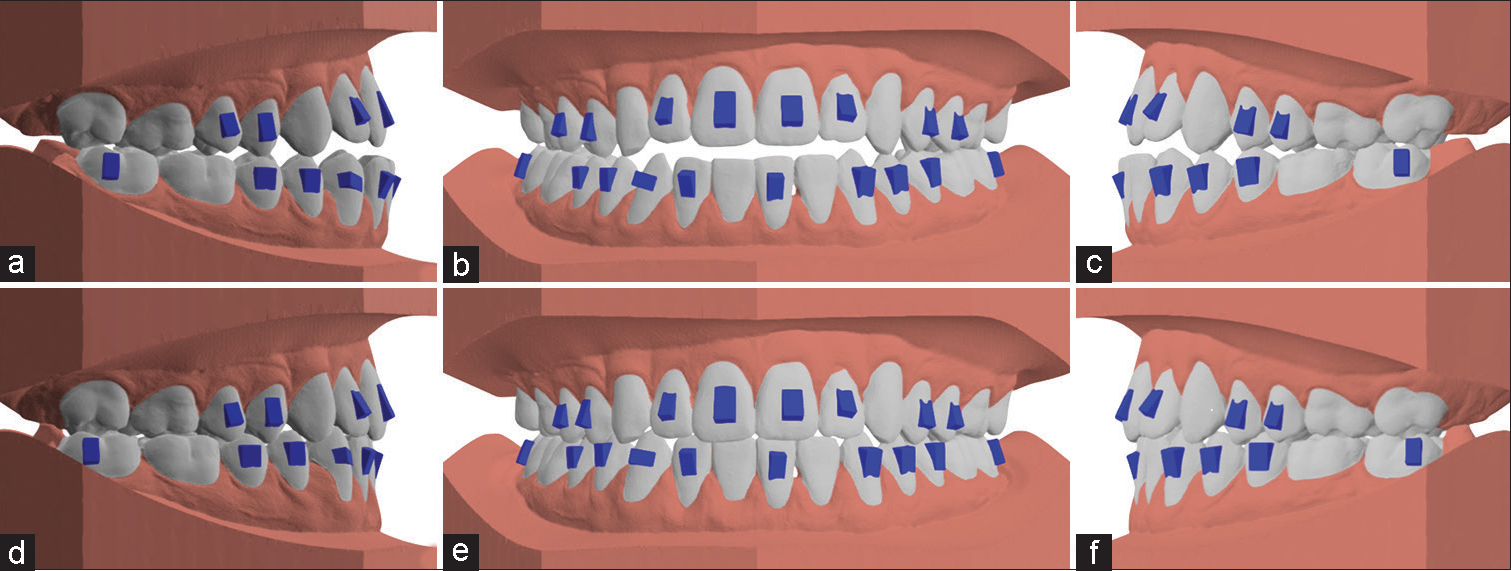
- Digital planification with grip point. (a-c) pre-treatment models, (d-f) programmed post-treatment.
Eighteen aligners (F22, Sweden and Martina, Due Carrare, Padova, Italy) for upper and lower dental arches were planned.
Six ounces, 3/16 of diameter Class III elastics were delivered to solve the sagittal relationship. The patient was instructed to wear both CAs and elastics applied from cuts made on CAs for 22 h a day.
The patient was asked to change set of aligner every 14 days and the check-up appointments were planned every month. [Figure 3] shows treatment progress.
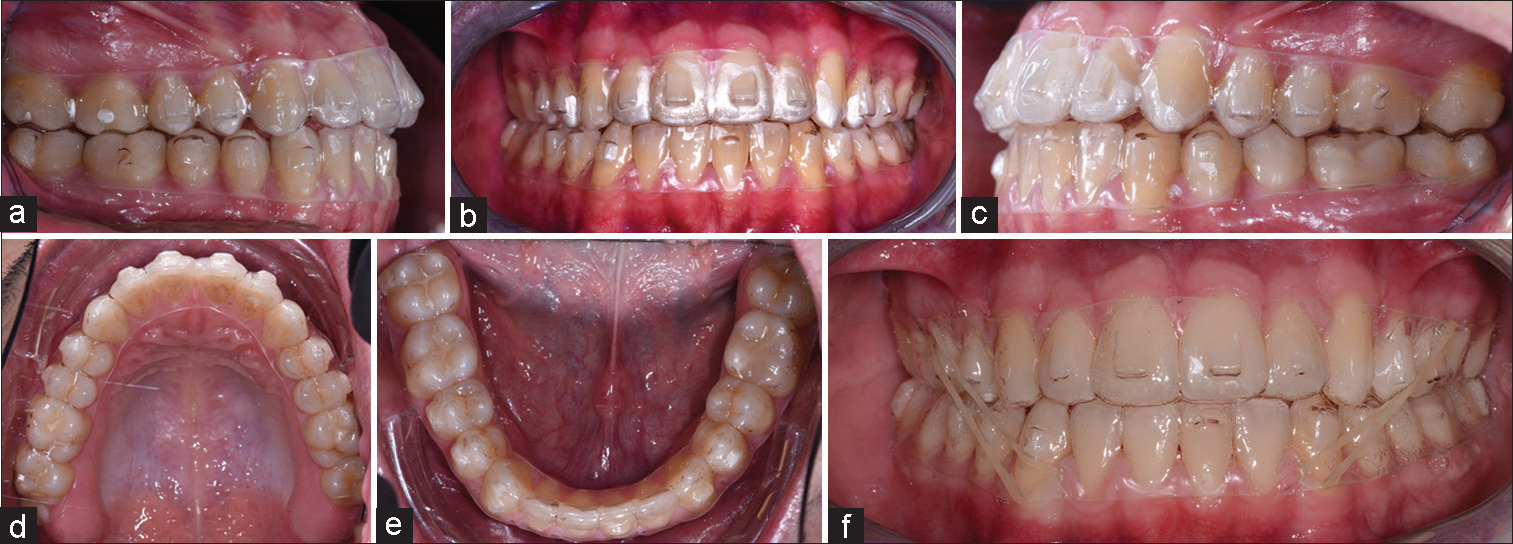
- Treatment progress with clear aligners. (a) intra-oral right lateral view with clear aligners, (b) intra-oral frontal view with clear aligners, (c) intra-oral left lateral view with clear aligners, (d) upper occlusal view with clear aligners, (e) lower occlusal view with clear aligners, (f) intra-oral frontal view with clear aligners and class III elastics.
Treatment results
Total treatment time was nine months. Post-treatment extraoral photos show oval face, slight left chin deviation, good incisal exposure when smiling and straight profile [Figure 4].
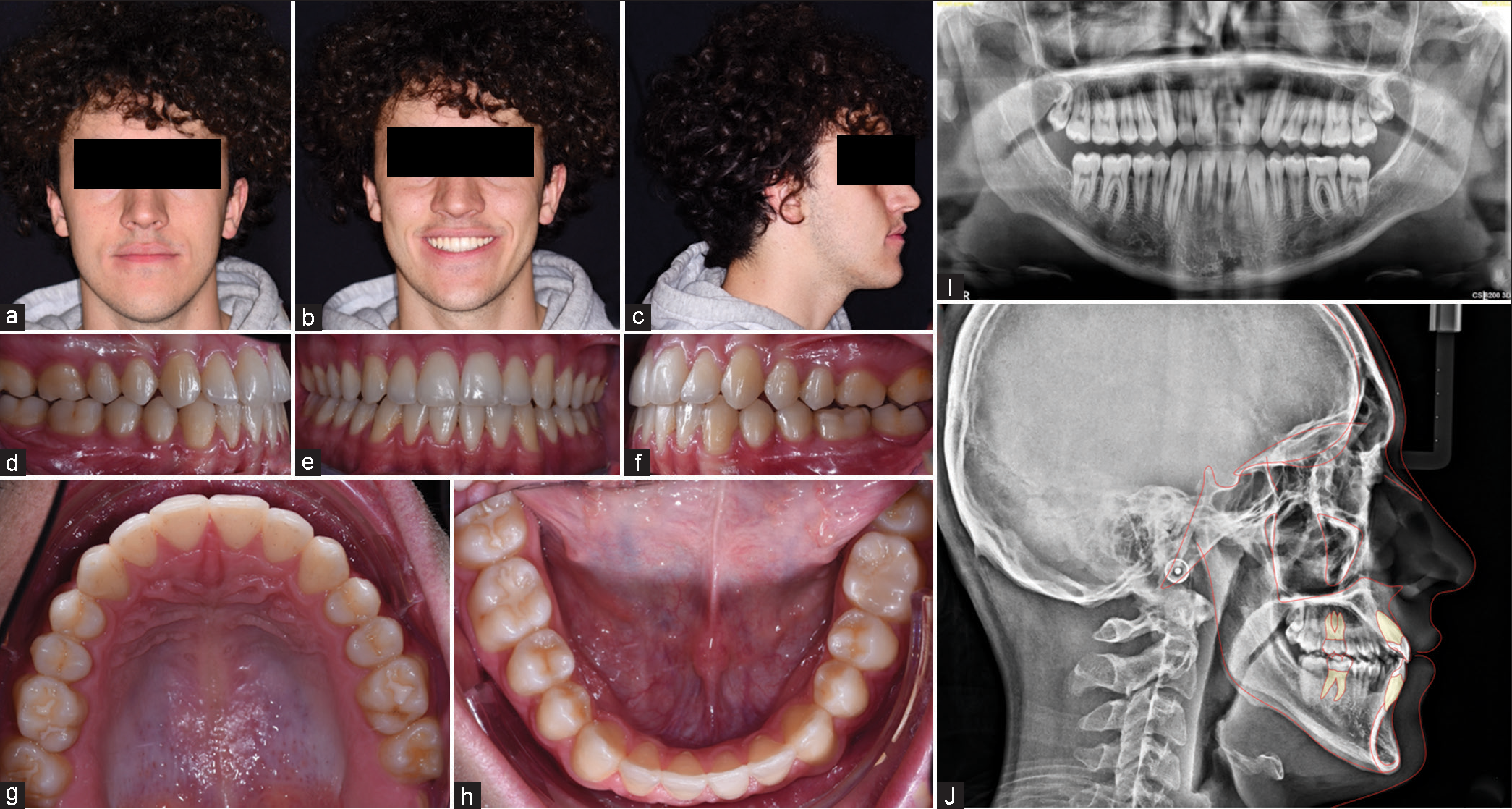
- Final extraoral (a-c), intraoral photos (d-h), panoramic X-ray (i), lateral cephalogram (j).
Intraorally, the patient shows bilateral molar and canine Class I relationship, correct overjet and overbite, and alignment of upper and lower arches [Figure 4].
Post-treatment radiographs show no signs of radicular or bone resorption, maintenance of skeletal Class III, control of vertical dimension (FMA = 34.4), upper incisors proclination (U1-PP = 117), and lower incisors retroclination (IMPA = 79.1). Lower third molars were extracted during the orthodontic therapy [Figure 4].
Superimposition of pre- and post-treatment lateral cephalograms on the cranial base revealed stability of skeletal structures. Superimpositions on maxillary and mandibular stable structures revealed upper incisor extrusion and proclination, lower incisor extrusion and retroclination, upper molar and lower molar, respectively, mesial and distal tipping, due to Class III elastics use.[3,4] [Figure 5].
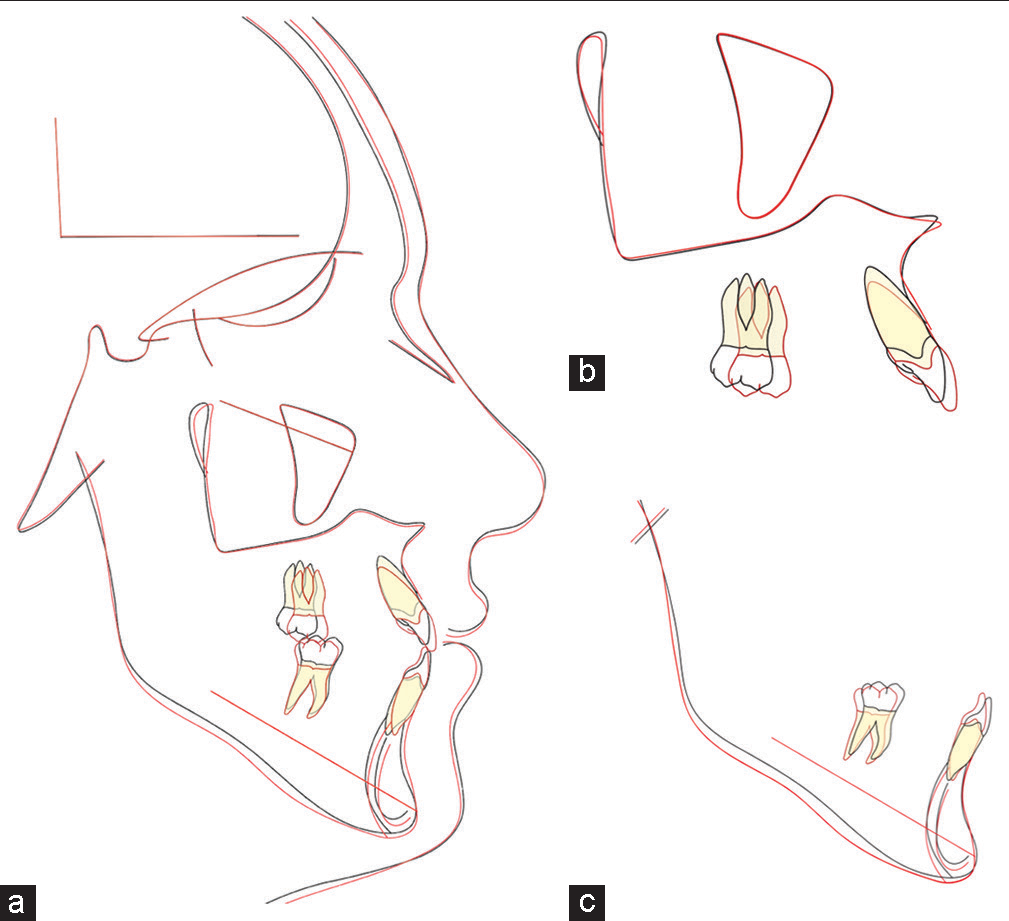
- (a) superimposition on cranial base, (b) on maxillary stable structures, (c) on mandibular stable structures.
At the end of treatment, grip points were removed; thermoformed removable retainers were delivered to the patient who was asked to wear them every night together with Class III elastics. After four months from the end of treatment, Class III elastics were suspended and the patient was asked to wear only removable retainers every night.
The intraoral photos after one year from the end of treatment show stability of open bite closure [Figure 6].

- One-year follow-up intraoral pictures. (a) intra-oral right lateral view, (b) intra-oral frontal, (c) intra-oral left lateral view, (d) upper occlusal view, (e) lower occlusal view.
DISCUSSION
This case report demonstrates a successful compensatory treatment of Skeletal and Dental Class III relationship featured by increased vertical dimension and AOB using CAs.
The decision of employing this treatment method was justified by the need of a dentoalveolar compensation, of a good vertical control, and no requested radicular movements.
Indeed, mainly tipping movements, which are reported as the most predictable, were planned to correct AOB and Class III.[5]
As extrusion movements are documented to be more difficult to obtain with CAs with a, grip points were planned to be used.[6,7]
To avoid a clockwise mandibular rotation, it is crucial to have a good vertical control. CAs have been proven to be effective in controlling vertical dimension for two reasons: Molar intrusion and incisor movement. From literature, it emerges that AOB is mainly corrected by the second mechanism as molars undergo little movements.[8,9] Harris and colleagues have demonstrated that upper incisors retrocline of 10.91 ± 6.95 and extrude of 1.45 ± 0.89 mm while upper molar intrude of 0.47 ± 0.59 mm.
Post-treatment cephalometric tracing reported a good control of vertical dimension despite the use of Class III elastics thanks to the correct digital planification.
For what concerns long-term stability, Gu and colleagues demonstrated that patient with AOB treated using CAs had their overbite corrected and after 9 months, the result was stable although the initial negative overbite was not excessive (−2.23 ± 1.86 mm).[10]
Unfortunately, even in this clinical case, the follow-up period was not long (one year) but the age of the patient, the end of growth, the lack of tongue thrusting habit make foresee a good stability.
CONCLUSION
In this clinical case, the successful dentoalveolar compensation was accomplished by upper incisors proclination and extrusion and lower incisor retroclination. Careful diagnosis, treatment planning, and clinical management were fundamental for the successful treatment.
Ethical approval
The research/study complied with the Helsinki Declaration of 1964.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
Dr. Luca Lombardo is on the editorial board of the journal.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Efficiency, effectiveness and treatment stability of clear aligners: A systematic review and meta-analysis. Orthod Craniofac Res. 2017;20:127-33.
- [CrossRef] [PubMed] [Google Scholar]
- Prediction of mandibular growth rotation. Am J Orthod. 1969;55:585-99.
- [CrossRef] [PubMed] [Google Scholar]
- Growth of the maxilla in three dimensions as revealed radiographically by the implant method. Br J Orthod. 1977;4:53-64.
- [CrossRef] [PubMed] [Google Scholar]
- Predictability of orthodontic movement with orthodontic aligners: A retrospective study. Prog Orthod. 2017;18:35.
- [CrossRef] [PubMed] [Google Scholar]
- Effectiveness of clear aligner therapy for orthodontic treatment: A systematic review. Orthod Craniofac Res. 2020;23:133-42.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical effectiveness of clear aligner treatment compared to fixed appliance treatment: An overview of systematic reviews. Clin Oral Investig. 2022;26:2353-70.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of open bite closure using clear aligners: A retrospective study. Prog Orthod. 2020;21:23.
- [CrossRef] [PubMed] [Google Scholar]
- Management of overbite with the invisalign appliance. Am J Orthod Dentofacial Orthop. 2017;151:691-9.e2.
- [CrossRef] [PubMed] [Google Scholar]
- Anterior openbite malocclusion in adults. Angle Orthod. 2022;92:27-35.
- [CrossRef] [PubMed] [Google Scholar]




