

Translate this page into:
Comparison of mean canine retraction between healed and recently extracted site: A single center, randomized control trial

*Corresponding author: Nazneen Rabia Zubair, Department of Orthodontics, Altamash Institute of Dental Medicine, Karachi, Sindh, Pakistan. nazneenzubair@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Zubair NR, Ehsan AA, Sakrani H. Comparison of mean canine retraction between healed and recently extracted site: A single center, randomized control trial. APOS Trends Orthod 2021;11(2):132-9.
Abstract
Objectives:
The objective of this “2-arm parallel” trial was to compare mean canine retraction into healed and recently extracted site.
Materials and Methods:
One of the sides of the maxillary dental arch of the patients having undergone orthodontic treatment at orthodontic department of a private hospital was randomly allocated to recent extraction side, while the contra-lateral side to healed extraction site. Eligibility criteria included no active local or systemic diseases including long-term medications. The main outcome was canine retraction into the extraction sites. Simple randomization technique was used allocate the right and left sides of the arch to one of the groups with allocation concealment through sequentially numbered, opaque, and sealed envelopes. Blinding was applicable for outcome assessor only. The patients were reviewed after 1 month of retraction. Data were analyzed on an intention to treat basis, using paired t-test was applied to compare the canine retraction between healed and recently extracted site (P ≤ 0.05 statistically significant).
Results:
Thirty-five patients with a mean age of 17.6 years were randomized in a 1:1 ratio for one of the sides of the arch to either recent extraction site or healed extraction site. After a month active retraction in 32 patients, the canine at recent extraction site moved 1.17 ± 0.27 mm in 1 month and 0.75 ± 0.26 mm in 1 month on the healed extraction site (P = 0.00). Two patients were lost to follow-up. No harm was observed.
Conclusion:
The results of the study indicate that the mean canine retraction was faster into the recent extraction site. The mean difference of 0.45 mm between the two sides was found be statistically significant.
Keywords
Mean canine retraction
Recent and delayed extraction sites
Regional acceleratory phenomenon
Extraction space closure

INTRODUCTION
Canine retraction is one of the steps of space closure during orthodontic treatment that involves anterior retraction. This is done not only to relieve crowding, closing space after tooth extraction, reducing large over jet and establishing Class I canine relation but also to achieve optimal occlusal stability and esthetics.[1-3]
The importance of time frame for orthodontic treatment is reflected in the literature as efforts have been made to compare various methods of space closure and prove the superiority of one over the other. For example, there are studies that have determined the efficient technique for retracting canine and compared various methods of achieving it.[4] Samuel et al. compared medium Nickel Titanium (NiTi) light, medium, and heavy NiTi coil spring with elastic modules.[5] Others compared elastomeric auxiliaries with NiTi coil spring and found later to produce much faster rate of retraction[5-7] with the mean difference of 0.20 mm/month (95% CI: 0.12–0.28) as reported by a systematic, review, and meta-analysis.[8] Various studies have also been conducted using segmental arch approach of canine retraction with its advantages particularly highlighted by Burstone in 1962.
Studies have also found that altered alveolar bone resistance and rate of remodeling could affect the rate of tooth movement, degree of tipping or bodily movement of a tooth, and eventually the esthetic results of orthodontic treatment.[9,10] Although, these studied have significantly contributed to the biomechanical aspect of tooth movement, much remains to be known regarding the biological factors that can eventually impact the procedure.
Some researchers have also compared canine retraction using conventional anchorage versus titanium implant anchorage and concluded that the rate of canine retraction was faster with titanium implants (maxilla: 0.93 mm/ month, mandible: 0.83 mm/month with titanium implant vs. maxilla: 0.81 mm/month, mandible: 0.76 mm/month with conventional molar anchorage);[11] while others evaluated the rate of distal movement of maxillary canine with NiTi coil spring with two different bracket systems, clinically, and radiographically.[12]
Häsler et al. compared the rate of canine retraction between healed and recently extracted site in his pilot study and reported that the median distal movement of canine for delayed site was 3.92 (range 1.53–6.09), while for recently extracted site it was 4.60 (range 3.07–7.43).[1] On the contrary, the experimental study conducted in animal by Bauer reported it to be faster into healed extraction site.[13] Although these studies have investigated canine retraction into healed versus recent extraction site, no randomized control trial has been published comparing the difference in the canine retraction between the two sites. Furthermore, the limited studies on humans and the difference between the results of humans and animals highlights the need for further investigation.
Specific objectives
In this study, we aimed to compare the mean canine retraction between healed and recently extracted site.
Hypothesis
Null hypothesis
There is no difference in canine retraction between healed and recently extracted site.
Alternate hypothesis
There is a difference in canine retraction between healed and recently extracted site.
MATERIALS AND METHODS
Trial design and any changes after trial commencement
This was a parallel-group, randomized, and active-controlled trial with a 1:1 allocation ratio.
IRB approval and trial registration
The approval from the Institutional Review Board was taken before the commencement of the trial. This trial was not registered.
Institute of IRB
This study was conducted at Altamash Institute of Dental Medicine, Karachi, Pakistan.
Approval number
AIDM/EC/06/2019/15.
Participants, eligibility criteria, and settings
Patients who were registered for the orthodontic treatment and required first bicuspid extraction were recruited in the department of orthodontics at a private hospital from September 2019 to May 2020.
The selection criteria were: Patents presented with malocclusion requiring first bicupids extraction with no active local (oral) or systemic diseases and long-term medications. Subjects with history of smoking, age above 30 years or below 15 years or who did not wish to participate were excluded from the study. Written informed consent was obtained from the patients before their recruitment. No changes were made after commencement of the trial.
Intervention
After thorough diagnostic and treatment planning procedure, the bracketing of the dental arches was done, molars were banded, and alignment and leveling was commenced. After going through the sequence of arch wires required for alignment, maxillary first bicuspid was extracted randomly from one of the sides of the maxillary arch (right or left) after reaching 017 × 25 NiTi wire and this side of the arch was considered as healed extraction site. The contra lateral first bicuspid was extracted after 1 month of the previous extraction. This was considered as recent extraction site. After 8 days of the last extraction, molars were stabilized by co-ligating all the posterior teeth and placing omega loop flushed with first molar on both sides of the arch to minimize their mesial movement. All four incisors were also colligated. Canines were ligated individually on both sides and retraction was initiated on 17 × 25 stainless steel wire using NiTi closed coil springs simultaneously on both the sides of the arch. Care was taken to deliver the same amount of retraction force on both sides of the arch by ensuring equal amount of activation of closed coil spring. Distal tipping movement of canine was minimized by rectangular steel as a working wire.
After 1 month of active canine retraction, alginate impression was taken and poured with the plaster. The final recordings were made on the cast using Vernier Caliper with an accuracy of 0.05 mm. The distance in millimeters was measured from the distal surface of canine to the mesial surface of second premolar at the contact point. This was confirmed by the amount of space reduced by distal movement of canine out of the total space present between lateral incisor and second bicuspid. The readings were recorded on the record sheet.
Outcome and any changes after trial commencement
The primary outcome was to find out the mean canine retraction into the healed and recent extraction site.
The patients were advised to report after 1 month of active canine retraction. In case of breakage of the bracket or coil spring, the patent was advised to report immediately to the orthodontic office. If the patients failed to comply, they were considered as loss to follow-up as their non-compliance could eventually affect the accuracy of results. There were no outcome changes after the commencement of the trial.
Sample size calculation
The sample size was determined to be 32 for each group of recent and healed extraction site (total 64) at CI 95% and α – 0.05 with power of 80%, taken from the calculated means for healed site (3.86 ± 1.33) and recent extraction site (4.925 ± 1.28) from their respective median and range from the study by Häsler et al.[1] About 10% (3 for each group, six in total) of the determined sample size was added for each group, taking into account the loss to follow-up.
Interim analysis and stopping guidelines
Not applicable.
Randomization (random number generation, allocation concealment, and implementation)
Randomization was done using simple randomization technique. Allocation concealment was achieved using enveloping technique, that is, opaque, sequentially numbered, and sealed envelopes prepared before trial were used to allocate the sides of the arch to each group. Dental nurse was responsible to open the envelope in sequence to ensure the implementation of randomization process [Figure 1].
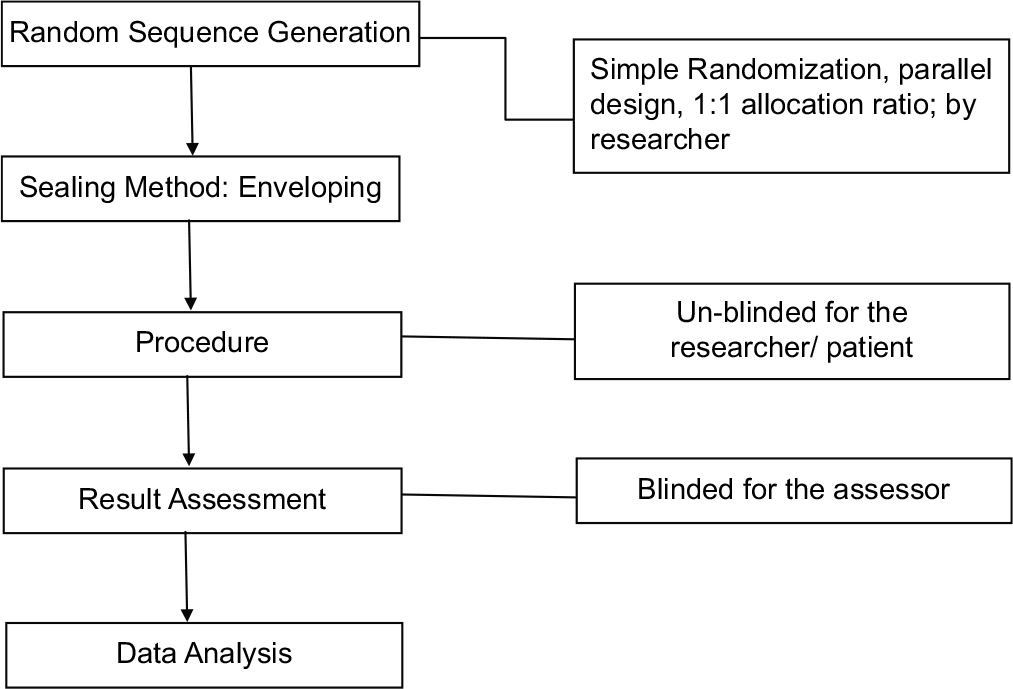
- Randomization process.
Blinding
Although it was not possible to blind the investigator and the patient, the outcome assessor was blinded from the procedure.
Statistical analysis (primary and secondary outcomes, and subgroup analysis)
The data were analyzed using SPSS statistical software version 23. Mean and standard deviation (Median [IQR]) was calculated for age and canine retraction for both sides. Frequency and percentage were computed for gender. Independent t-test was applied to compare the canine retraction between healed and recent extraction site. Effect modifiers such as age and gender were addressed through stratification and post-stratification. Paired t-test was applied. A value of P ≤ 0.05 was taken as statistically significant.
RESULTS
Participant flow
The sides of the maxillary dental arch of 35 patients with mean age 17.6 ± 3.7 years were randomized in a 1:1 ratio to be equally allocated to either healed or recent extraction site. Two of them were lost to follow-up. The recruitment process commenced in September 2019 and ended in May 2020 [Figure 2].
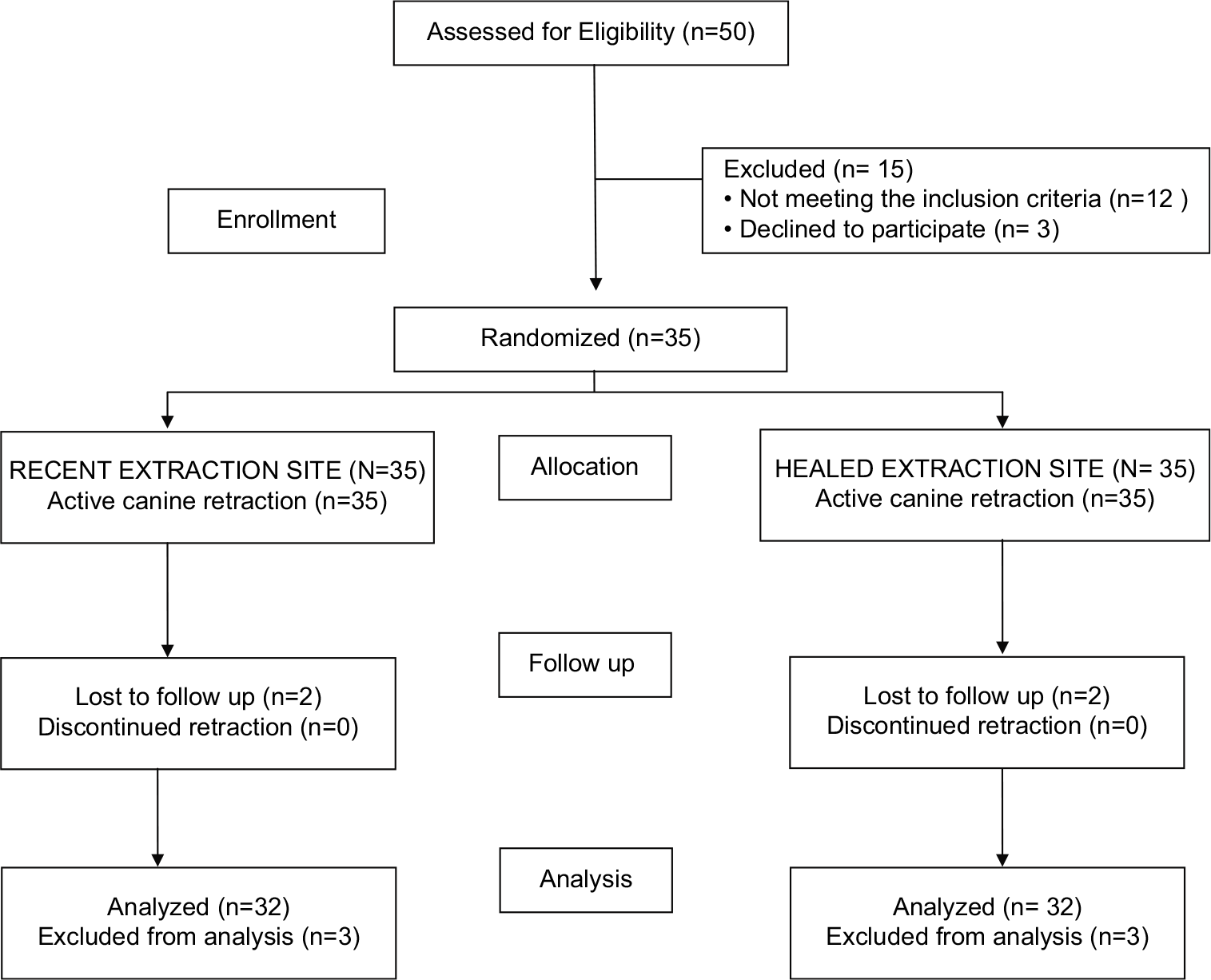
- Consort patient flow diagram.
Baseline data
Majority of the participants were females, that is, 75% (n = 24), while males were found to be 25% (n = 8). The mean age of the participants was 17.6 years ± 3.7 and IQR 12–27 years [Figure 3 and Table 1].
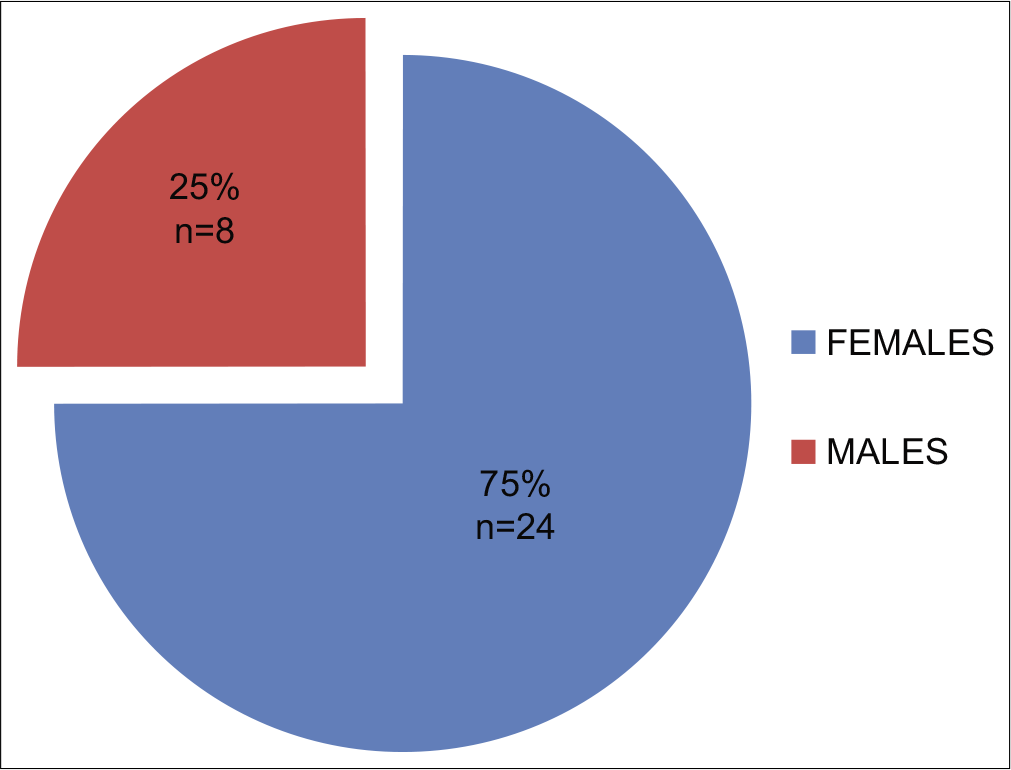
- Demographics: Gender distribution of the participants.
| Age in years | Mean | Standard deviation | Median | IQR |
|---|---|---|---|---|
| 17.6 | 3.7 | 16.0 | 12–27 |
Numbers analyzed for outcome estimation and precision, subgroup analysis
The mean canine retraction of 32 patients for the healed extraction site was found to be 0.75 ± 0.26 mm in 1 month, while for the recent extraction site it was found to be 1.17 ± 0.27 mm in 1 month. The amount of retraction was, therefore, higher for the recent extraction site [Figure 4]. The primary analysis was carried out on an intention-to-treat basis.
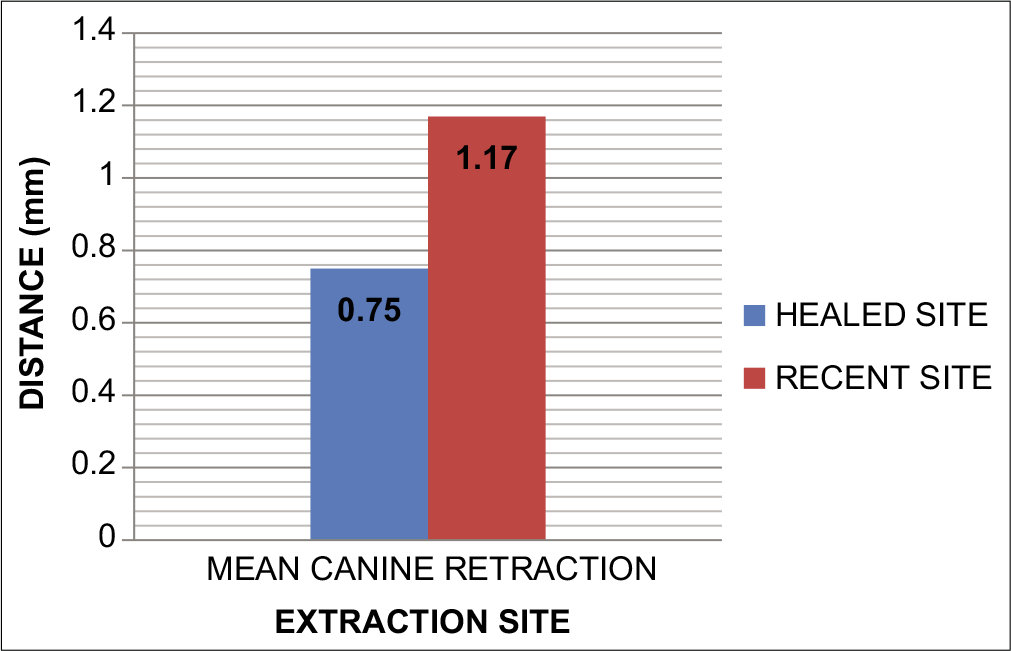
- Mean canine retraction for healed and recent extraction site.
The difference in the mean canine retraction between the healed and recently extracted site was found to be 0.45 mm in 1 month and this was statistically significant with (P = 0.00) [Table 2].
| Healed extraction site | Recent extraction site | Mean difference (mm) |
P-value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean canine retraction (mm) |
SD | Median | IQR | Mean canine retraction (mm) |
SD | Median | IQR | ||
| 0.759 | 0.26 | 0.750 | 0.25–1.15 | 1.17 | 0.27 | 1.25 | 0.75–1.65 | 0.45 | 0.00* |
When the stratification for age and gender was done, it was found that for gender, the mean canine retraction was higher for males compared to females for both recent and healed extraction site. The results were statistically significant with P = 0.00 (P ≤ 0.05), [Table 3].
| Gender | Canine retraction on healed side | Canine retraction on recent side | t | P-value |
|---|---|---|---|---|
| Male | ||||
| Mean | 0.8750 | 1.3250 | 9.82 | 0.00* |
| n | 8 | 8 | ||
| SD | 0.21044 | 0.29520 | ||
| Female | ||||
| Mean | 0.7208 | 1.1250 | 5.54 | 0.00* |
| n | 24 | 24 | ||
| SD | 0.27816 | 0.24891 |
For the age and canine retraction, it was found that the mean canine retraction was higher in the younger age groups, that is, from 15 to 22 years of age compared to the patients in 23–30 years of age group; therefore, it varied with age for both the recent and healed extraction site. The results were statistically significant for both the sites (P ≤ 0.05), [Table 4].
| Age groups (years) |
Canine retraction groups | Mean | Standard deviation |
P-value |
|---|---|---|---|---|
| 15–22 | Recent site | 1.20 | 0.26 | 0.00 |
| Healed site | 0.78 | 0.24 | ||
| 23–30 | Recent site | 1.09 | 0.28 | 0.02 |
| Healed site | 0.68 | 0.33 |
Harm
No serious harm was observed.
DISCUSSION
The trial attempted to compare the mean canine retraction between healed and recent extraction site by randomizing 70 extraction sites (35 patients) of the maxillary dental arch to be equally allocated for either the recent or healed extraction group. It was noted that the canine moved faster into the recent extraction site compared to the side of the dental arch where the socket was allowed to heal before retraction. The difference 0.45 mm in 1 month was found to be statistically significant with P = 0.00. The results of our study are comparable to the pilot study available in the literature that has compared canine retraction between the two extraction sites, with the median difference between the two sites of 0.75 mm, range 1.18–2.67. This difference was also found to be statistically significant with the mean canine retraction of 3.7 mm on the recent and 1.8 mm for the healed extraction site.[1] Another study conducted in 1970 conducted the oxytetracycline microflorescent comparison of orthodontic retraction between healed and recently extracted sites, concluded, and recommended that to minimize the duration of orthodontic treatment, retraction should be commenced early after orthodontic extraction. The author also concluded that the rate of tooth movement was higher for the recent extraction site.[14]
It is believed among the orthodontists that initiating early traction of tooth following extraction is more advantageous compared to a period of delay in retraction after extraction. Starting the retraction into the premolar extraction site distally, as early as 2 weeks post-extraction, results in more rapid tooth movement,[15] since there is only a thin inter-dental septum that acts as a separation between thin connective tissue and the tooth, thus it should move rapidly.[16] In our study, the retraction was initiated after 1 week of extraction for recent extraction site.
Although the clinical studies are very limited, the abundance of histological studies can be referred to to understand the characteristics of bone at and around and healing of the extraction sites along with the possible reasons for rapid retraction into the recent extraction site.
It was suggested by some authors that orthodontic tooth movement occurs because of the elastic nature of bone and its bending capacity.[17-19] However, this concept has been gradually disregarded when findings of the histological investigations were considered.[20-27] The previous studies have highlighted that the nature and character of bone are not the same for recently extracted and healed extraction site and that it varies according to the amount of healing that has taken place.[28-32] Furthermore, in the extraction site, the contraction of the transeptal fibers result in distal of teeth, as suggested by others.[32-40]
A study on histological and histochemical investigation of human alveolar socket healing in undisturbed extraction wounds found out that healing of the extraction site is a rapid process such that the bony trabeculae fills in the two-third of the alveolar socket, starting from its base, by 1.25 months (38 days) following extraction.[28] This process of rapid bone formation reached maximum at approximately 100 days following extraction and this was reflected as increased radio-opacity on the radiograph. At this point, the bone at the extraction site was indistinguishable from the normal bone elsewhere or surrounding adjacent alveolar process due to the similarity in the radio-density.[28]
Another histological study, investigating the advantages of early tooth movement following extraction versus delayed tooth movement, concluded that at the site of delayed tooth movement, the density of alveolar bone was low and the type of bone there was mature lamellar bone. Furthermore, pronounced atrophy of the alveolar process with the apposition of periosteal bone in the direction of tooth movement was found there with increased tendency toward invagination of gingiva. On the contrary, the bone density surrounding the site of the early tooth movement was higher with an immature bundle bone. The alveolar process there was broader with a reduced tendency toward invagination of gingiva.[41] These histological findings therefore indicate that orthodontic traction should be commenced at an early stage following extraction of teeth.
In our study, even though the time difference between recent and healed extraction site was only 1 month, the canine retraction was significantly different for both the sites. In our opinion, the possible reason could be attributed to the histological changes, which could be the immature and less calcified bone surrounding the socket, seen on the periapical radiograph as reduced bone density compared to that of healed extraction site, where most of the trabecular bone forms by only 38 days following extraction, as highlighted by the previous studies.[28,41] Although the phenomenon of regional acceleration could also be a factor for rapid tooth movement, as it usually peaks at 1–2 months,[42] since its impact would be on the tooth movement for both recent as well as healed extraction site, therefore, its influence could be less likely for the significant difference between the retraction for the two sites.
Had the time difference for the two sites been set longer, like 3 months, the results might still be expected to be significant in our opinion; however, this needs to be confirmed by conducting another trial.
To avoid unnecessary delays during orthodontic treatment, our recommendation would be, therefore to commence orthodontic tooth movement early following extraction to minimize the overall duration of treatment. This could be for cases that require active canine retraction following extraction once alignment and leveling is done, as well as for cases that require early extractions due to crowding or any other reason, where the advantage of early tooth movement could be taken for other purposes, such as alignment and leveling or relief of crowding.
Furthermore, we would recommend that the commencement of tooth movement could be as early as within 1–2 weeks following extraction, when the histological changes are favorable.[15] The greater the delay in commencing tooth movement, the greater the time required for space closure, as two-third of the socket is filled with trabecular bone by 38 days following extraction.[28]
The advantage of this study is the randomized allocation of the sides of the dental arch to the two groups of extraction site resulting in low risk of selection bias.
Limitations
Although it was not possible to blind the patients and the operator during intervention, the outcome assessment was blinded to minimize the risk of observation and detection biases. Furthermore, since the study design was prospective randomized control trial, it allowed better comparison and evaluation of the mean retraction rate. The limitations of our study might be unequal gender distribution of the participants. This could be because the females usually seem to be more concerned about their appearance and therefore seek orthodontic treatment more frequently compared to males. In addition, the canine retraction was measured for a shorter period of time, that is, 1 month for each patient. This was done to avoid any potential confounding factors such as breakage of the wire, bracket or the NiTi closed coil spring, and arise of any potential bias.
Generalizability
Since this research was conducted in a single center, the generalizability of these results might be limited.
CONCLUSION
Based on the results of this randomized control trial, it is evident that the canine retraction into the recent extraction site is faster compared to the healed extraction site. The difference in the mean retraction rate between the two sites is statistically significant. Therefore, the null hypothesis was rejected. The commencement of tooth movement early following extraction would therefore help minimize unnecessary delays in the treatment and reduce patient burn out.
Declaration of patient consent
Institutional Review Board permission obtained for the study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- A clinical comparison of the rate of maxillary canine retraction into healed and recent extraction sites a pilot study. Eur J Orthod. 1997;19:711-9.
- [CrossRef] [PubMed] [Google Scholar]
- Canine retraction and anchorage loss: Self-ligating versus conventional brackets in a randomized split-mouth study. Angle Orthod. 2014;84:846-52.
- [CrossRef] [PubMed] [Google Scholar]
- Role of insulin-like growth factors (IGFs), their receptors and genetic regulation in the chondrogenesis and growth of the mandibular condylar cartilage. J Cell Physiol. 2012;227:1796-804.
- [CrossRef] [PubMed] [Google Scholar]
- Canine retraction: A systematic review of different methods used. J Orthod Sci. 2015;4:1.
- [CrossRef] [PubMed] [Google Scholar]
- A clinical study of space closure with nickel-titanium closed coil springs and an elastic module. Am J Orthod Dentofac Orthop. 1998;114:73-9.
- [CrossRef] [Google Scholar]
- Canine retraction with rare earth magnets: An investigation into the validity of the constant force hypothesis. Am J Orthod Dentofac Orthop. 1996;109:489-95.
- [CrossRef] [Google Scholar]
- A randomized clinical trial to compare three methods of orthodontic space closure. J Orthod. 2002;29:31-6.
- [CrossRef] [PubMed] [Google Scholar]
- Effectiveness of nickel-titanium springs vs elastomeric chains in orthodontic space closure: A systematic review and meta-analysis. Orthod Craniofac Res. 2018;21:12-9.
- [CrossRef] [PubMed] [Google Scholar]
- The effect of low level laser therapy on the rate of tooth movement and pain perception during canine retraction. Oral Health Dent Manag. 2014;13:183-8.
- [Google Scholar]
- Load system of segmented T-loops for canine retraction. Am J Orthod Dentofac Orthop. 2013;144:548-56.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of rate of canine retraction with conventional molar anchorage and titanium implant anchorage. Am J Orthod Dentofac Orthop. 2008;134:30-5.
- [CrossRef] [PubMed] [Google Scholar]
- A clinical and radiographic study to evaluate the rate of retraction of maxillary canine using nickel-titanium closed coil spring with two different bracket systems. APOS Trends Orthod. 2014;4:169-77.
- [CrossRef] [Google Scholar]
- The Rate of Orthodontic Retraction into Extraction wound Undergoing Various Stages of Healing: A Radiographic Study [MS Thesis] USA: St Louis University, School of Dentistry; 1969.
- [Google Scholar]
- Oxytetracycline microfluorescent comparison of orthodontic retraction into recent and healed extraction sites. Am J Orthod. 1970;58:215-39.
- [CrossRef] [Google Scholar]
- Oxytetracycline microfluorescent comparison of orthodontic retraction into recent and healed extraction sites. Am J Orthod. 1970;58:215-39.
- [CrossRef] [Google Scholar]
- Treatment of Malocclusion of the Teeth (7th ed). Ch. 6. Philadelphia, PA: SS White Dental Manufacturing Co; 1907.
- [Google Scholar]
- An Inquiry into Physiological and Pathological Changes in Animal Tissues in Regulating Teeth. . 1876;18
- [Google Scholar]
- Irregularities of Teeth and their Treatment Philadelphia, PA: Blakiston, Son, and Co.; 1888.
- [Google Scholar]
- Some histologic facts useful in orthodontic practice. Am J Orthodont Oral Surg. 1942;28:167-72.
- [CrossRef] [Google Scholar]
- Die Vernnderungen der gemebebei ubermassiger beanspruchung der zahne, cited by C. F. Bodecker. Int J Orthodont. 1932;18:895-917.
- [CrossRef] [Google Scholar]
- Tissue changes particularly of the bone incident to tooth movement. Am J Orthod. 1912;3:57-67.
- [Google Scholar]
- Human tissue response to orthodontic intervention of short and long duration. Am J Orthodont Oral Surg. 1942;28:263-301.
- [CrossRef] [Google Scholar]
- Tissue changes incident to orthodontic tooth movement. Int J Orthodont. 1932;18:331-52.
- [CrossRef] [Google Scholar]
- Histological and histochemical investigation of human alveolar socket healing in undisturbed extraction wounds. J Am Dent A. 1960;61:33-44.
- [CrossRef] [PubMed] [Google Scholar]
- Synopsis of Oral Pathology (2nd ed). St. Louis: The CV Mosby Company; 1965. p. :89-94.
- [Google Scholar]
- A histologic study of repair in the maxillary bone following surgery. J Am Dent Assoc. 1929;16:1987-97.
- [CrossRef] [Google Scholar]
- Orthodontics and transeptal fibers: A histological interpretation of repair phenomena following the removal of first premolars with retraction of the anterior segment. Am J Orthodont. 1945;31:1-20.
- [CrossRef] [Google Scholar]
- A study of the periodontal membrane from the orthodontist's standpoint. Am Soc Orthodont 1912:144-61.
- [Google Scholar]
- Tissue behavior during orthodontic tooth movement. Am J Orthodont. 1960;46:881-900.
- [CrossRef] [Google Scholar]
- Clinical and histologic observations on tooth movement during and after orthodontic treatment. Am J Orthodont. 1967;53:721-45.
- [CrossRef] [Google Scholar]
- Orban's oral histology and embryology (6th ed). St. Louis: The CP Mosby Company; 1962.
- [Google Scholar]
- Orthodontic relapses analyzed in a study of connective tissue fibres. Am J Orthodont. 1959;45:93-109.
- [CrossRef] [Google Scholar]
- The normal movement of the remaining teeth subsequent to extraction (as translated by Milo Hellman) Am Orthodont. 1910;1:56-8.
- [Google Scholar]
- Orthodontic retraction into recent and healed extraction sites. A histologic study. J Orofac Orthop. 1997;58:90-9.
- [Google Scholar]
- The biology of fracture healing, an overview for clinicians, Part II. Clin Orthop Relat Res. 1989;248:294-309.
- [CrossRef] [Google Scholar]




