

Translate this page into:
Comparison of settling of occlusion in modified and full coverage thermoplastic retainers using T-scan

*Corresponding author: Lokamithra Ragunanthanan, Department of Orthodontics, Meenakshi Ammal Dental College, Chennai, Tamil Nadu, India. lokha_mithra2007@yahoo.co.in
-
Received: ,
Accepted: ,
How to cite this article: Ragunanthanan L, Maheshwari U, Vijayalakshmi D. Comparison of settling of occlusion in modified and full coverage thermoplastic retainers using T-scan. APOS Trends Orthod 2022;12:115-24.
Abstract
Objectives:
The main intent of the study was to evaluate and compare the occlusal bite forces after settling between conventional and modified thermoplastic retainer groups using T-Scan.
Material and Methods:
This study comprised a total of 20 patients, who approached the retention phase after completion of fixed orthodontic therapy. After debonding (T0), occlusal analysis using the T-Scan system was done at centric occlusion. Group I (control) – 10 patients received the conventional thermoplastic retainer and Group II (experimental) – 10 patients received the modified thermoplastic retainer. Patients were instructed to wear the retainer continuously for 6 months except while eating and brushing. T-scan analysis after 6 months (T6) was done to evaluate the changes in occlusal bite forces. The obtained data were evaluated using STATA/IC software version 16.1 at a predetermined probability value of 0.05 which was considered significant.
Results:
The result obtained from this study was suggestive of significant improvement in bite force levels at centric occlusion in the modified thermoplastic group compared with the conventional group. Comparing the right (P < 0.17) and left (P < 0.01) posterior region, there was significant increase on the left side. A significant increase at maximum centric occlusion (P < 0.01) was seen in the region of the first molars. The anterior region did not show any improvement (P < 0.62) after 6 months of retention.
Conclusion:
Partial coverage of thermoplastic retainer significantly improves the occlusal contacts and force levels. The maximum change was seen in the posterior region and the minimum change in the anterior region at centric occlusion.
Keywords
Thermoplastic retainer
Partial coverage retainer
Retention
Occlusal bite force
Settling of occlusion
T-Scan system

INTRODUCTION
Orthodontic treatment of any malocclusion aims at achieving ideal tooth alignment, functional and esthetic occlusion, and stability at the end of active treatment. After orthodontic correction, aligned teeth have an inherent potential to change their position, which may be due to the influence of periodontal and gingival tissues, unstable positions of teeth, and continued skeletal growth pattern. Therefore, retention devices are necessary to maintain the arch form, keep the teeth in their ideal static and functional positions, and minimize relapse.[1,2]
The most important feature of occlusal stability is the presence of occlusal contacts (centric stops) on the functional cusps which affect the health of the stomatognathic system. “Ideally located contacts” and centric occlusion contacts help in vertically directed forces parallel to the long axes of the teeth and minimize the stress distribution on the periodontium.[3] Settling allows relative movements of posterior teeth in the vertical direction and increases the number of occlusal contacts during the retention phase and the choice of retention appliance may affect settling.[2-5] Functional occlusal contacts and intercuspation are the keys to a stable orthodontic treatment.[6]
The most frequently used retention appliance for over a century, is the Hawley retainer introduced by Hawley in 1919.[7] Nevertheless, due to growing esthetic demands, especially among adults, patients want no visibility of wires during the retention phase. To overcome the obstacle, an invisible retainer, is now widely used, which is also referred to as Vacuum-formed retainer, clear overlay retainer, and Essix retainer.[8] These retainers are thin but strong, easy to fabricate, esthetic, comfortable, inexpensive, and easy to clean, and hence have a high level of patient acceptance. Their major disadvantage is the tendency to open the bite due to occlusal coverage.[9]
Previous studies indicate improvement in occlusion and an increase in the number of occlusal contacts during the retention period, with the use of Hawley retainers, tooth positioners, and fixed retention appliances due to settling,[10-15] but not with thermoplastic overlay retainers.[2] To overcome this limitation, a modified thermoplastic retainer (partial coverage thermoplastic retainer) was fabricated without posterior occlusal coverage with the primary objective of improving settling.[16]
There are various non-digital methods for assessing occlusal relations based on the clinician’s subjective interpretation of the marking indicator used, combined with the patient’s verbal “feel” feedback.[17] Commonly used indicators are articulating papers, Shimstock foils, impression waxes, and silicone impressions; but none of these can objectively and accurately quantify the amount of occlusal force (OcFr) or the sequence of contacts that occur during various functional jaw movements.
A recent advancement includes a digital occlusal analysis system (T-Scan III, Version 7, Tekscan, Inc.S.Boston, MA, USA) that records and displays a real-time dynamic recording of the patient’s closure from initial contact into complete intercuspation (maximum intercuspation [MIP])[18] during which the patient occludes on a compressible, electronically charged, mylar-encased 100 micron-thick high definition recording sensor.
In our study, one of the main objectives was to evaluate and compare the settling efficiency between conventional and modified thermoplastic retainers by measuring occlusal bite force levels using the T-Scan system.
MATERIAL AND METHODS
Null hypothesis
In the present study, the null hypothesis is assumed that there was no change in occlusal bite forces between full coverage and partial coverage thermoplastic retainer.
Subject selection
The subjects enrolled for this study, underwent fixed orthodontic treatment in the Department of Orthodontics and Dentofacial Orthopaedics in Meenakshi Ammal Dental College and Hospital, Chennai. The study included a total of 20 subjects (11 females and 9 males) who approached the final retention stage of treatment following the debonding of the fixed appliance. Patients were well acquainted with the study, and informed consent was acquired from all patients or from their parents, who were chosen for this study.
Inclusion criteria
Both males and females aged 15–30 years
Patients receiving upper and lower thermoplastic retainers
Patients who underwent fixed appliance treatment for a minimum of 15 months
Patients with Class I canine and molar relations.
Exclusion criteria
Patients with missing teeth
History of temperomandibular dysfunction
Prosthetic crowns in posterior teeth
Periodontal disease, and/or muscle dysfunction
Non-compliance regarding retainer wear, attendance at long-term follow-up appointments, or both
Syndromes
Systemic diseases.
For the study power of 95% and an alpha error of 5% calculated using Sampling software G power version 3.1.9.2, a total of 20 samples were required for this study. The selected sample was randomly divided into two groups as follows:
Group 1 – 10 subjects (6 females and 4 males) received the conventional thermoplastic retainer (control group).
Group II – 10 subjects (5 females and 5 males) received the modified thermoplastic retainer (test group).
OcFr measuring device
The T-Scan III (Tekscan, Inc., S. Boston, MA, USA) is an intra-oral occlusal analysis system that records and quantifies the contact force distribution in real-time continuously from initial contact till MIP during closure. Its components include a sensor and support, a handle assembly, the system unit, computer software, and a printer [Figure 1].

- T-Scan connected to a laptop.
The sensor is the key component made of two layers of conductive grid encased within two layers of pressure-sensitive Mylar foil and is available in small and large sizes for easy adaptation to the arch dimension. It sends information regarding the real-time occlusal contact area and force distribution to the accompanying Windows-based software package. This information can be viewed in two and three dimensions [Figure 2] or as a continuous force “movie” of the entire recorded occlusal contact event. The sensor supports also available in small and large sizes is used to hold the sensor and is attached through a latch system to the recording handle which is connected to the computer with a USB interface.

- Two and three-dimensional view of T-Scan result.
Method of analysis
The subjects were asked to sit in an upright position in the dental chair, and either a small or large size sensor was selected depending on the patient’s arch dimension. HD sensors for each patient were calibrated before actual recording to match the recording sensor’s sensitivity level to the OcFr level of the subject by limiting the number of red/ pink high force columns/contacts observed in the graphical display, to a maximum of three during pre-recording test conditions. The sensor was placed intraorally with the central mark of the sensor handle between the central incisors, and multibite recordings at centric occlusion were made by asking the patient to firmly occlude in MIP. To assess the sensitivity of the T-Scan system, the recordings were taken 3 times for each patient. Following occlusal parameters were analyzed from the obtained recordings:
Centric maximum
Left posterior region
Right posterior region
Anterior region.
Following occlusal analysis, the sensor wafer was washed with clean water, dried using cotton, stored in a plastic pouch, and was used again for occlusal recording after 6 months. The patients in each group were delivered with their respective type of thermoplastic retainer and were instructed to wear them full time except while eating and brushing for 6 months. Instructions regarding retainer maintenance and hygiene were also reinforced to the patients. After 6 months of retainer wear, occlusal recordings using T-Scan were taken again for comparison of retainer efficiency (T6).
Retainer fabrication
The thermoplastic retainers were fabricated using copolyester Essix sheets of 1 mm thickness. The modified retainer was designed by eliminating the occlusal and half of the lingual and facial surfaces [Figure 3]. They were given to the patient the same day as the fixed appliance was debonded after occlusal analysis.

- Modified thermoplastic retainer by eliminating occlusal surface of the posterior teeth.
Statistical analysis
The collected data were analyzed with STATA/IC software version 16.1 (STATA CORP., TEXAS). Means and standard deviation (s.d.) of force percentage values at centric occlusion were calculated from the three recordings done on each subject. Reproducibility of T-Scan variables was assessed by a coefficient of variation [CV = (s.d. of force%/n)*100].
To test for the normality of the distribution of all variables, the Shapiro-Wilk test was used. As there was skewing in collected data, a non-parametric test was used for hypothesis testing.
Intra-group analysis to check for the significance of T-Scan variables between T0 and T6 in conventional and modified thermoplastic retainer groups was done using a one-sided sign test. The inter-group comparison was done using the Mann-Whitney U test.
RESULTS
The CV of bite force% values calculated using three consecutive recordings was 0.7500 (SE 0.0797; 95% CI [0.5831–0.9169]) suggestive of high reproducibility of T-Scan [Table 1].
| Interrater agreement | |||||
|---|---|---|---|---|---|
| Coef. | Std. Err. | t | P>│t│ | [95% Conf. Interval] | |
| Percentage Agreement | 0.7500 | 0.0797 | 9.40 | 0.000 | 0.5831 0.9169 |
| Cohen/Conger’s Kappa | 0.7359 | 0.0819 | 8.99 | 0.000 | 0.5645 0.9073 |
Number of subjects = 20
Ratings per subject = 3
Number of rating categories = 23
Occlusal settling patterns assessed using the T-Scan III system between the two groups before and after 6 months of retention are depicted in [Figures 4 and 5].

- Occlusal pattern seen in conventional retainer group (a) at T0 and (b) at T6 depicting no significant improvement in the occlusal bite force levels.

- Occlusal pattern seen in modified retainer group (a) at T0 and (b) at T6 depicting significant improvement and even distribution of occlusal bite forces among the posterior teeth.
[Tables 2 and 3] depicts the intra-group analysis of the conventional and modified thermoplastic retainer groups respectively. Bite force values in the modified group in posterior left, posterior right, and at centric maximum were (29.66 ± 21.84% [median = 37.45, IQR = 5.8–48.5]), (39.63 ± 16.77% [median = 37.7, IQR = 20.5–52.5]), and (71.17 ± 18.32% [median = 70, IQR = 66.7–100]) at T0, and (40.51 ± 11.93% [median = 42.5, IQR = 30.4–45.2]), (50.34% ± 10.29% [median = 51.7, IQR = 40.4–53.4]), and (91.46% ± 13.74% [100, 50–100]) at T6 respectively. There was a significant increase in bite force levels in the modified group at T6 in centric occlusion with P < 0.05.
| T scan parameters | T0 | T6 | P value (Median of t6-t10 > 0) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Median (%) | Minimum (%) | Maximum (%) | IQR (%) | Median (%) | Minimum (%) | Maximum (%) | IQR (%) | ||
| Centric occlusion Anterior region | 6.05 | 4.6 | 23.4 | 5.7-13.3 | 19.55 | 6.2 | 24.2 | 18.7-20.1 | 0.0547 |
| Posterior right region | 42.6 | 35.9 | 56.7 | 38.7-46.5 | 46.55 | 38.9 | 52.7 | 43.7-46.9 | 0.3770 |
| Posterior left region | 46.3 | 19.9 | 56.4 | 44.8-53.7 | 39.15 | 27.8 | 46.2 | 32.2-45.5 | 0.9648 |
| Maximum force | 50 | 33.3 | 57.9 | 36.6-54 | 49.8 | 28.8 | 100 | 33.3-54 | 0.9375 |
IQR: Interquartile range
| T scan parameters | T0 | T6 | P value (Median of t6-t10 > 0) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Median (%) | Minimum (%) | Maximum (%) | IQR (%) | Median (%) | Minimum (%) | Maximum (%) | IQR (%) | ||
| Centric occlusion Anterior region | 16.6 | 1.8 | 30.5 | 5.8-24.5 | 6.8 | 3.9 | 27.7 | 4.7-21.2 | 0.6230 |
| Posterior right region | 37.45 | 4.4 | 60 | 5.8-48.5 | 42.5 | 24.4 | 58.8 | 30.4-45.2 | 0.1719 |
| Posterior left region | 37.7 | 19.6 | 65.1 | 20.5-52.5 | 51.7 | 35.4 | 70.7 | 40.4-53.4 | 0.0107* |
| Maximum force | 70 | 45 | 100 | 66.7-100 | 100 | 60 | 100 | 50-100 | 0.0195* |
IQR: Interquartile range
Intergroup analysis shown in [Table 4] revealed a significant improvement in the posterior left region, and centric maximum, (P < 0.05) with the modified thermoplastic retainer group [Figures 6 and 7]. Clinical intra-oral photograhs before and after retainer use are depicted in Figures 8 and 9.
| T scan parameters | (T6-T0) Modified thermoplastic retainer | (T6-T0) Conventional thermoplastic retainer | P-value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Median | Minimum | Maximum | IQR | Median | Minimum | Maximum | IQR | ||
| Centric occlusion | |||||||||
| Anterior region | 5.75 | –9.5 | 15.3 | 1.2–10.7 | 13.3 | –10 | 14.3 | 1.6–14 | 0.2899 |
| Posterior right region | 11.35 | –5.3 | 28.4 | –2.6–21 | 0.2 | –4 | 10.1 | –1.9–4.7 | 0.1986 |
| Posterior left region | 6.5 | –10 | 31.3 | 5.1–16.9 | –1.5 | –21.5 | 8.3 | –18.2–0 | 0.0101* |
| Maximum force | 28.95 | –20 | 40 | 10–30 | –1.25 | –7.9 | 50 | –4.9–0 | 0.0366* |
DISCUSSION
Occlusion achieved at the end of orthodontic treatment is one of the important factors related to the health of the temperomandibular joint and masticatory muscles[19] and is directly related to the stability of orthodontic treatment.[3] Occlusal stability is important not only for static occlusion but also for functional occlusion. Changes in occlusal contacts can be seen immediately after removal of the fixed appliance due to post-treatment settling, or over years after retention.[13-15] Evaluation of occlusion after orthodontic treatment is not a routine procedure, however, assessing the location and number of contacts after treatment are helpful predictors of occlusal stability to avoid relapse in the future.[13]
An occlusal contact or area can be defined by its shape, size, and position, irrespective of whether it makes an occlusal or near-occlusal contact with opposite teeth.[17] Traditional methods for evaluating occlusal contacts include measurement using millimeter ruler, articulating paper or occlusal wax, silicone impressions, and mapping with an occlusal sketch, photographs, or study models.[20] Gazit and Liberman, 1989,[21] used photocclusion technique, and Durbin and Sadowsky,1986,[10] used polyether rubber impression material to evaluate occlusal contact changes and showed an increase by 56% in 1 year and 1.26% in 3 months, respectively. However, their sensitivity and reliability are susceptible to inaccurate results due to the thickness, strength, physical properties, and elasticity of the materials used in the oral environment.[22] Saraçoğlu and Özpinar,[23] suggested that using articulating paper showed that the sensitivity of the paper is often affected by saliva, due to which shows false-positive results, and it does not measure the force with which teeth occlude.
Examining changes in OcFr is one of the methods for assessing occlusal and jaw function and is related to craniofacial morphology.[24] To date, there are no studies evaluating bite force after active orthodontic treatment. This study was undertaken to evaluate the changes in occlusal bite forces during the retention phase using the T-Scan system.
At present, computer-aided determination of occlusal parameters using pressure-sensitive films is used. Varga et al., 2017[25] developed the prototype of the T Scan system, and in the past 25 years has undergone multiple revisions of hardware, sensor, and software to come up with the latest version of the T-Scam III system. In the present study, T Scan III is preferred because it gives both two-dimensional and three-dimensional force values, force percentage per tooth/arch or half/quadrants, and consistently measures OcFrs in a highly repeatable fashion when compared to the highly subjective method of “judging” paper mark size appearance characteristics.[26]
It allows fast and accurate analysis and registration of the occlusal-articulation system, and better visualization of the dental arches making them much more superior than other methods[27], and is an ideal tool for chair-side assessment of occlusion.[18] The measured T-Scan forces are displayed as relative values instead of absolute values since the change in muscular forces would affect the force values between different intercuspations resulting in highly variable results.
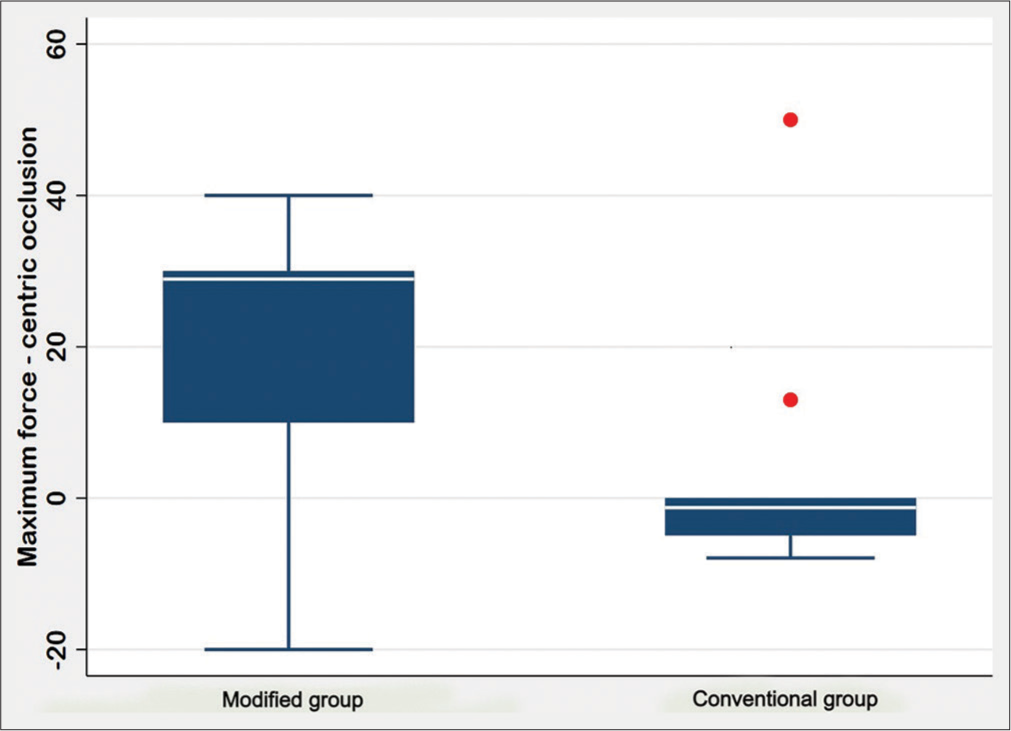
- Box-and-whisker plot for improvement in bite force at centric maximum.
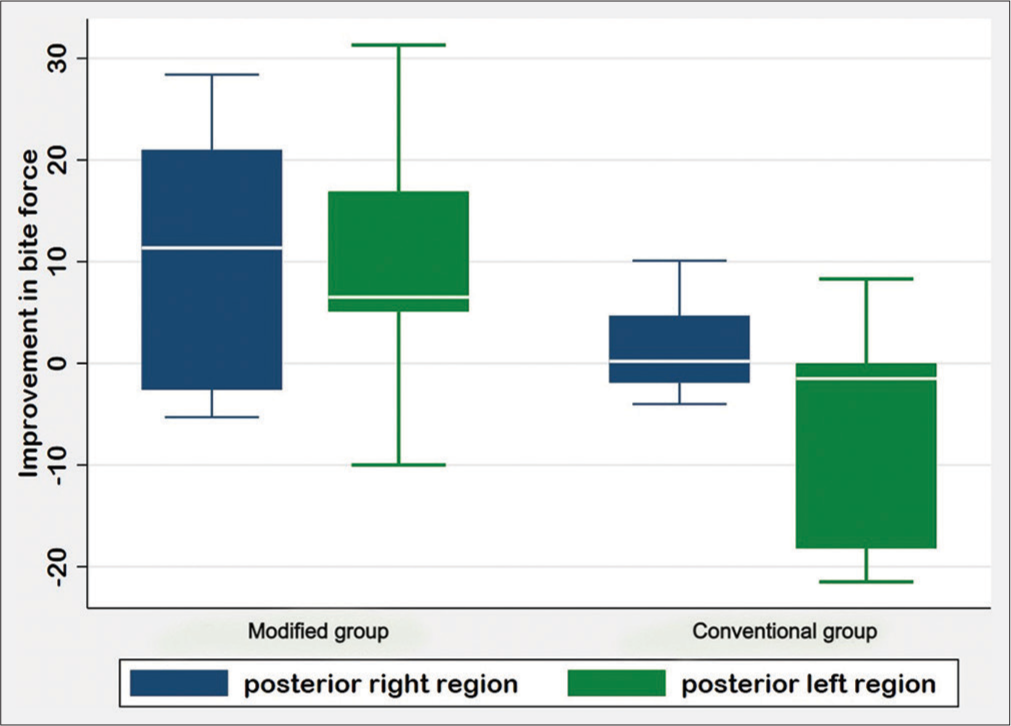
- Box-and-whisker plot for improvement in bite force at centric occlusion.
The ideal retainer should achieve three-dimensional control of teeth while allowing settling in horizontal and vertical directions within safe margins and preventing the tendency of relapse.[2] Duration of retainer wear is based on the patient’s age, growth pattern, type, the severity of malocclusion, habits, and other etiologic factors, mechanics used, and the clinical experience of the orthodontist. The most frequently used retainers are Hawley, vacuum formed and fixed bonded retainers. Thermoplastic retainers first introduced by Ponitz,[8] are preferred more by practitioners due to their ease of fabrication chairside, minimal or no adjustment on delivery, and better acceptability by patients as an esthetic retention device. The disadvantage of plasticized retainer is the occlusal coverage which interferes in occlusion leading to posterior open bite, TMJ pain, and non-settling of occlusion. Muscle recovery is longer due to uncertainty in biting while wearing the thermoplastic retainer.[28] However, improvement in posterior occlusion can be seen in post retention phase after the withdrawal of the retainer.[29] The present study showed no improvement in occlusal contacts, and hence no increase in bite force level after 6 months of retention with conventional full-coverage thermoplastic retainer following Dincer and Aslan, 2009[29] and Sauget et al.,1997.[2]
OcFr is used for the assessment of jaw functions and is related to craniofacial morphology.[24] Sultana et al., 2002[4] evaluated OcFr and occlusal area (OcAr) using pressure-sensitive sheets and showed a significant increase in OcFr and OcAr after 1 year of retention with upper wrap-around and lower bonded retainer (P < 0.0001). This is due to the improved interdigitation of the teeth after debonding and the teeth are allowed to settle during the retention phase with begg retainer. Hence, we evaluated occlusal settling and the changes in OcFrs with thermoplastic clear retainers by eliminating the occlusal coverage in the posterior teeth region.
Modification in thermoplastic retainer by providing a relief in the occlusal surfaces of premolars and canine to aid in settling was first proposed by Theroux in 2003.[30] Following the study by Aslan,[27] the modified group in the current study showed a significant improvement in bite force at centric occlusion after 6 months of retention (P < 0.05). The molars which are discluded during active orthodontic treatment, settle after the removal of orthodontic bands due to remodeling of gingival and periodontal fibers, and continuous vertical eruption over the life of the tooth.[31] Hence, the bite force values at maximum centric occlusion in the present study were significantly increased in the molar region, especially first molars, in the modified group (P < 0.01).
Wearing retainers for at least 1 year after active orthodontic treatment, as suggested by many authors, is the most accepted retention protocol for removable appliances.[32] Reitan,[31] suggested that the reorganization of periodontal fibers occurs over 3–4 months while the remodeling of the gingival fibers takes 4–6 months after active orthodontic treatment; the supracrestal elastic fibers remain stretched for more than 232 days. Hence, a retention period of 6 months should be an ideal period for settling occlusion and varies depending on the malocclusion and treatment mechanics.
On evaluating OcFrs in different regions at centric occlusion, there was no significant increase in the anterior, posterior right, and posterior left region in the conventional group, and in the anterior region in the modified group. The complete occlusal and incisal coverage in the conventional group and partial incisal coverage in the modified group inhibits the freedom of physiologic movement of teeth, and hence there is reduced vertical settling of occlusion. Finishing orthodontic treatment with a proper cusp fossa relation in the posteriors, and lower incisal edge directly below the center of the cingulum plateau of the maxillary incisor helps in achieving a stable static and functional occlusion.[33]

- Visual examination of no significant changes in occlusion with conventional retainer wear at T0 and T6.

- Visual examination of settling in occlusion with modified retainer wear at T0 and T6.
Neurophysiologists state that a relationship exists between the dominance of certain body functions and brain laterality.[34] Barcellos et al., 2012[35] and Martinez-Gomis et al., 2009[36] have reported that the chewing side preference is related to lateralities such as handedness, footedness, eyedness, and earedness. Although bilateral balanced mastication is effective for efficient deglutition,[37] Ferrario, 2000[38] reported that healthy individuals prefer one side for chewing and generate higher muscular activity on the preferred side. In the present study, although there was an improvement in the left and right posterior regions after 6 months in the modified group, the significant increase in the left posterior region (P = 0.001) could be attributed to the preferential unilateral chewing pattern due to dominance of hemispheric laterality.[39]
The increase in occlusal contacts and OcFrs in the current study for a retention period of 6 months was seen with the modified thermoplastic retainer. This was due to the partial coverage of the retainer which led to the substantial improvement in the vertical settling of occlusion.
CONCLUSION
Improvement in vertical settling, and hence, OcFrs can be seen with partial coverage thermoplastic retainers compared with full coverage retainers
An increase in bite force levels was more pronounced in the posterior region and least evident in the anterior region
Bite force levels at maximum centric occlusion improved in the posterior teeth, especially near the first molar region
The left posterior dentition showed more OcFr values compared to the right posterior dentition at centric occlusion.
Ethical approval
The study proposal was submitted, and approval was obtained from the Institutional Review Board of Meenakshi Ammal Dental College, Maduravoyal, Chennai 600095, India before the commencement of the study. Protocol number-MADC/ IRB-XXIII/2018/373.
Declaration of patient consent
Institutional Review Board (IRB) permission was obtained for the study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- C of vacuum-formed and H retainers: A systematic review. Am J Orthod Dentofacial Orthop. 2014;145:720-7.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of occlusal contacts with the use of Hawley and clear overlay retainers. Angle Orthod. 1997;67:223-30.
- [Google Scholar]
- Evaluation, Diagnosis, and Treatment of Occlusal Problems (2nd ed). St. Louis: CV Mosby; 1989. p. 28-33, 41-5, 590-1
- [Google Scholar]
- Changes in occlusal force and occlusal contact area after active orthodontic treatment: A pilot study using pressure-sensitive sheets. J Oral Rehabil. 2002;29:484-91.
- [CrossRef] [PubMed] [Google Scholar]
- Retention procedures for stabilizing tooth position after treatment with orthodontic braces. Cochrane Database Syst Rev. 2016;2016:CD002283.
- [CrossRef] [PubMed] [Google Scholar]
- Considerations of dentofacial growth in long-term retention and stability: Is active retention needed? Am J Orthod Dentofac Orthop. 1992;101:297-302.
- [CrossRef] [Google Scholar]
- Changes in tooth contacts following orthodontic treatment. Am J Orthod Dentofac Orthop. 1986;90:375-82.
- [CrossRef] [Google Scholar]
- Occlusal contact changes after the active phase of orthodontic treatment. Am J Orthod Dentofac Orthop. 1992;102:22-8.
- [CrossRef] [Google Scholar]
- Changes in occlusal force and occlusal, Using contact area after active orthodontic treatment: A pilot study, 491 pressure-sensitive sheets. J Oral Rehabil. 2002;29:484.
- [CrossRef] [PubMed] [Google Scholar]
- The investigation of occlusal contacts during the retention period. Angle Orthod. 2003;73:640-6.
- [Google Scholar]
- Occlusal contacts with different retention procedures in the 1-year follow-up period. Am J Orthod Dentofac Orthop. 2007;131:357-62.
- [CrossRef] [PubMed] [Google Scholar]
- Occlusal contact changes with removable and bonded retainers in a 1-year retention period. Angle Orthod. 2009;79:867-72.
- [CrossRef] [PubMed] [Google Scholar]
- Computerized occlusal analysis as an alternative occlusal indicator. Cranio. 2016;34:52-7.
- [CrossRef] [PubMed] [Google Scholar]
- Force finishing and centering to balance a removable complete denture prosthesis using the T-scan III computerized occlusal analysis system. J Indian Prosthodont Soc. 2013;13:184-8.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of the effects of modified and full-coverage thermoplastic retainers on occlusal contacts. Orthodontics (Chic). 2013;14:e198-208.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of Post-orthodontic Occlusal Contacts with Wraparound and Clear Overlay Retainers. Amsterdam, Netherlands: Elsevier; 2017.
- [CrossRef] [Google Scholar]
- Occlusal contacts following orthodontic treatment measured by a photoocclusion technique. Angle Orthod. 1985;55:316-20.
- [Google Scholar]
- Limitations of traditional non-digital Computerized indicators when compared to TS, occlusal analysis In: Kerstein RB, ed. Handbook of Technology, Research: Computerized Occlusal Analysis IGI. Vol 1. Hershey, PA: Applications in Dental Medicine; 2015. p. :36-65.
- [CrossRef] [Google Scholar]
- In vivo and in vitro evaluation of occlusal indicator sensitivity. J Prosthet Dent. 2002;88:522-6.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of excursive occlusal force parameters in post-orthodontic and non-orthodontic subjects using T-Scan® III. Cranio. 2018;36:11-8.
- [CrossRef] [PubMed] [Google Scholar]
- Changes of bite force and occlusal contacts in the retention phase of orthodontic treatment: A controlled clinical trial. Am J Orthod Dentofac Orthop. 2017;152:767-77.
- [CrossRef] [PubMed] [Google Scholar]
- Relationship between articulation paper mark size and percentage of force measured with computerized occlusal analysis. J Adv Prosthodont. 2012;4:7-12.
- [CrossRef] [PubMed] [Google Scholar]
- Influence of anthropometry, TMD, and sex on molar bite force in adolescents with and without orthodontic needs. J Orofac Orthop. 2017;78:487-93.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of maximum voluntary bite force in adults with a normal assessment of maximum voluntary bite force in adults with normal occlusion and different types of malocclusions. J Contemp Dent Pract. 2012;13:534-8.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of thermoplastic retainers on occlusal contacts. Eur J Orthod. 2010;32:6-10.
- [CrossRef] [PubMed] [Google Scholar]
- Tissue rearrangement during retention of orthodontically rotated teeth. Angle Orthod. 1959;29:105-13.
- [Google Scholar]
- A possible biomechanical role of occlusal cusp-fossa contact relationships. J Oral Rehabil. 2013;40:69-79.
- [CrossRef] [PubMed] [Google Scholar]
- Hand Funct Child Found Remediat (2nd ed). Philadelphia, PA: Elsevier Health Science; 2006. p. :181.
- [Google Scholar]
- Absence or weak correlation between chewing side preference and lateralities in primary, mixed, and permanent dentition. Arch Oral Biol. 2012;57:1086-92.
- [CrossRef] [PubMed] [Google Scholar]
- Relationship between chewing side preference and handedness and lateral asymmetry of peripheral factors. Arch Oral Biol. 2009;54:101-7.
- [CrossRef] [PubMed] [Google Scholar]
- The determination of optimal human jaw movements based on their association with chewing performance. Arch Oral Biol. 1994;39:333-43.
- [CrossRef] [Google Scholar]
- An electromyographic investigation of masticatory muscles symmetry in normo-occlusion subjects. J Oral Rehabil. 2000;27:33-40.
- [CrossRef] [PubMed] [Google Scholar]
- Chewing side preference as a type of hemispheric laterality. J Oral Rehabil. 2004;31:412-6.
- [CrossRef] [PubMed] [Google Scholar]




