

Translate this page into:
Correlation of clivoaxial angle to skeletal malocclusions: A prescreening for future risk of neurodegenerative disorders
Address for Correspondence: Dr. Navdeep Bhusri, Department of Orthodontics, Postgraduate Clinic, Graduate School, University of the East, CM Recto Avenue, Manila, Philippines. E-mail: nav_bhusri@yahoo.co.in
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Bhusri N, Lim DC. Correlation of clivoaxial angle to skeletal malocclusions: A prescreening for future risk of neurodegenerative disorders. APOS Trends Orthod 2016;6:246-50.
Abstract
Objectives
To find out if there exists any correlation between clivoaxial angle (CXA) and skeletal malocclusions.
Materials
and Methods: Lateral cephalograms of 33 filipino patients equally divided in three types of skeletal malocclusions were traced, and cephalometric parameters CXA, BaSN, ANB, SNMPA, FMA, MMPA, and Y-axis were traced. Data underwent bivariate correlation and curve estimation analysis in SPSS 17.0 statistical software at confidence interval of 95% and 0.05 significance level.
Results
A highly significant (P = 0.003) strong negative correlation was revealed in Class III patients between CXA and BaSN.
Conclusion
Class III patients seem to have higher chances of craniocervical junction anomalies and thus might be at risk of developing neurodegenerative disorders in future.
Keywords
Clivoaxial angle
craniocervical junction
neurodegenerative disorders
skeletal malocclusion

INTRODUCTION
There has been a drastic rise in patients with neurodegenerative and functional disorders in the past decade, and early detection of such conditions is not yet feasible. Upright posture and motion of cervical spine increase the strain in craniocervical junction (CCJ) which is a crucial tollgate for cerebrospinal fluid and blood flow between spinal canal and cranial vault that may lead to faulty hydrodynamics in the craniospinal region and furthering to edema, chronic ischemia, and hydrocephalus.[1-6]
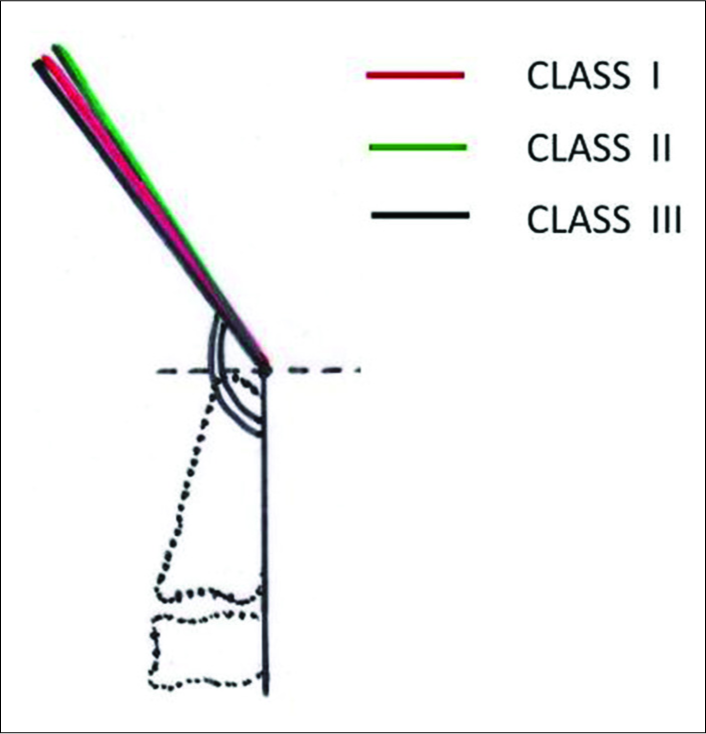
The clivoaxial angle (CXA) or upper cervical angle and cranial base angle, both are important for the function of the brainstem and cord. Just like increase in cranial base angle (BaSN) above than normal (125–143°) which is called platybasia[7,8] as classically described by Chamberlain, a lower than normal (150–165°) CXA compresses[9-14] the brainstem, cord, contents of foramen magnum, and spinal canal [Figures 1-3].[9,15] This not only causes functional Chiari formations[14,16] but also predisposes the individual to biomechanical neuraxial stress which is manifested by myelopathy, bulbar symptoms, and neck pain or headache.[9]
Biomechanics and mechanobiology are closely interrelated, neuronal bundles being the pathological substrate of deformative stress in this case due to kyphotic CXA directly leading to stretch triggered accumulation of neurofilament in axons[17] and thus apoptosis.[18] An abnormal CXA may lead to faulty craniospinal hydrodynamics increasing the chances of neurodegenerative disorders such as Alzheimer’s,[19,20] Parkinson’s,[19] multiple sclerosis,[21,22] obstructive sleep apnea, etc.[23,24]

- Normal craniocervical junction in the neutral position. The clivo-axial angle varies from 150° to 165°. There is minimal or zero deformative strain in the neutral state

- Normal craniocervical junction in flexion. The neuraxis stretches by approximately 10% of its total length with flexion of the craniocervical junction creating a strain ε = 0.1

- Pathological craniocervical junction with an abnormal clivo-axial angle in flexion. On full flexion at the craniocervical junction, the increase in the tangent arc creates a deformative strain approaching ε = 0.2. In vivo and in vitro models demonstrate loss of function with strains of 0.2
The aim of this study was to find if there exists any correlation between CXA and other craniofacial cephalometric parameters in different types of skeletal malocclusions.
MATERIALS AND METHODS
The study was a retrospective cephalometric study. Lateral cephalograms of 33 Filipino subjects, divided equally into three groups of Class I, II, and III malocclusions were obtained randomly from the pretreatment records of the orthodontic patients at Postgraduate Orthodontics Clinic, CM Recto Avenue, University of the East, Manila, Philippines.
These were traced by the author on cephalometric tracing sheets (Masel, Australia) using a 0.3 mm mechanical pencil (Staedtler, Germany) and the cephalometric parameters CXA, cranial base angle (BaSN), maxillomandibular angle (ANB), mandibular plane angle (SNMPA), Frankfort-mandibular plane angle (FMA), maxillomandibular plane angle (MMPA), and growth axis angle (Y-axis) were measured using cephalometric protractor (Ortho Organizers, US). Three X-rays from each group were randomly selected and retraced 1 week after the initial data recording by the author for error quantification.
The data recorded were subjected to descriptive statistics [Table 1], bivariate correlation [Table 2], and regression/ curve estimation analysis [Figures 5-7] using statistical software SPSS 17.0, IBM Corp., (SPSS Statistics for Windows, Version 17.0. Chicago (US), SPSS Inc.) at 95% confidence interval and 0.05 significance level.
| N=11 | Descriptive statistics | |||||
|---|---|---|---|---|---|---|
| Class I | Class II | Class III | ||||
| Mean | SD | Mean | SD | Mean | SD | |
| CXA | 154.05 | 6.38 | 155.18 | 7.4 | 155.54 | 8.63 |
| BaSN | 135 | 3.54 | 131.18 | 3.12 | 129.09 | 6.28 |
| ANB | 2 | 1 | 5 | 0.74 | -3.54 | 2.25 |
| SNMPA | 36.68 | 4.16 | 39.68 | 4.21 | 32.73 | 5.23 |
| MMPA | 28.36 | 3.77 | 32.32 | 4.83 | 28.18 | 4.47 |
| FMA | 27.86 | 4.85 | 32.73 | 4.49 | 26.36 | 3.52 |
| Y-Axis | 57.73 | 4.12 | 59.82 | 4.35 | 56.18 | 2.56 |
| Bivariate correlations | |||||||
|---|---|---|---|---|---|---|---|
| N=11 | CXA | BaSN | ANB | SNMPA | MMPA | Y-Axis | |
| CLASS I | CXA | 1 | |||||
| r | -0.541 | 0.102 | -0.195 | 0.008 | -0.030 | ||
| P | 0.086 | 0.766 | 0.565 | 0.982 | 0.931 | ||
| CXA | 1 | ||||||
| CLASS II | r | -0.257 | 0.374 | 0.206 | 0.299 | 0.501 | |
| P | 0.446 | 0.258 | 0.544 | 0.372 | 0.117 | ||
| CXA | 1 | ||||||
| CLASS III | r | -0.803 | 0.377 | -0.003 | 0.301 | 0.438 | |
| P | 0.003* | 0.253 | 0.993 | 0.369 | 0.177 | ||
- Minimum observed clivo-axial angle for Class I, II, and III were 145°, 146°, and 144°, respectively with standard deviation from normal increasing from Class I to III

- Class I regression curve

- Class II regression curve
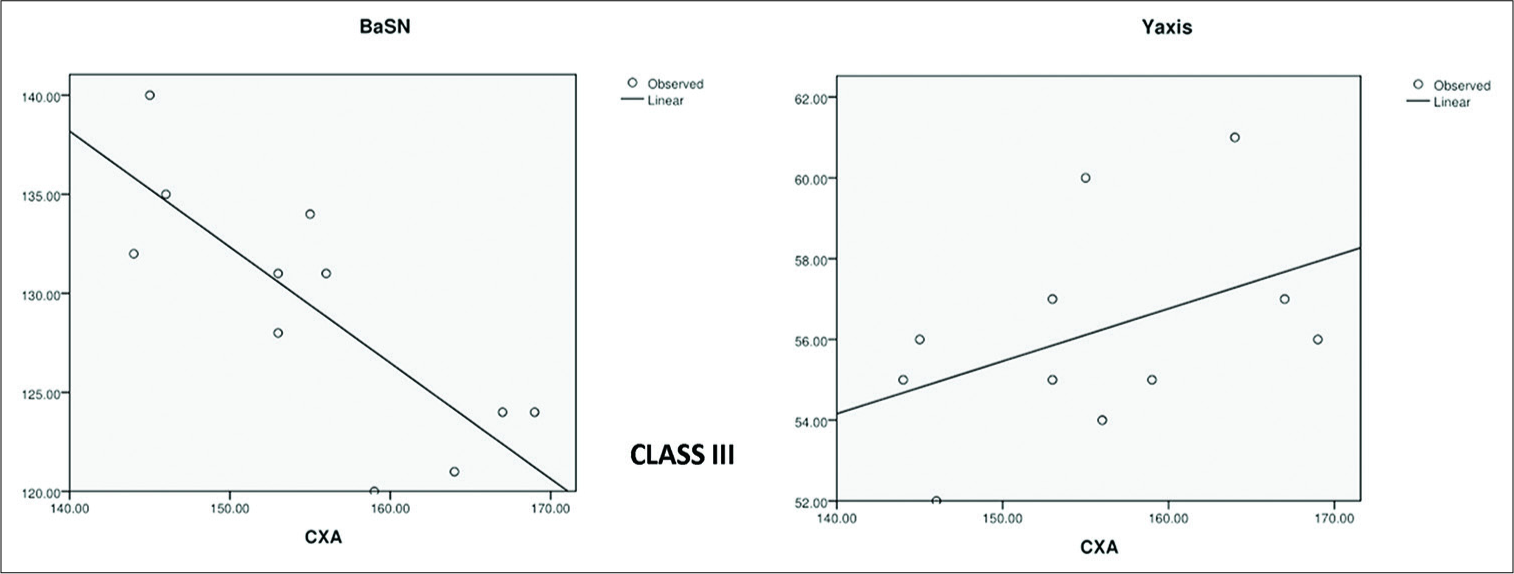
- Class III regression curve
RESULTS
Minimum observed clivo-axial angle for Class I, II, and III were 145°, 146°, and 144°, respectively with standard deviation from normal increasing from Class I to III [Figure 4]. In Class I skeletal malocclusion group, Pearson’s correlation coefficient “r” for CXA showed strong negative relationship to BaSN (−0.541), weak negative relationship to FMA (−0.266), negligible or no correlation for SNMPA (−0.195), MMPA (+0.008), Y-axis (−0.030), and ANB (+0.102).
In Class II group, value of “r” for CXA was found to have strong positive relationship for FMA (+0.537) and Y-axis (+0.501), a moderate positive relation to ANB (+0.374), weak positive relationship to SNMPA (+0.206), MMPA (+0.299), and a weak negative relation to BaSN (−0.257).
In skeletal Class III malocclusions, Pearson’s “r” for CXA showed a very strong negative correlation toBaSN (−0.803) which was highly significant (P < 0.05) at P = 0.003, Y-axis (+0.438) showed a strong positive relationship, MMPA (+0.301) and ANB (+0.377) gave moderate positive correlations, FMA (+0.285) had a weak relation to CXA, and SNMPA (−0.003) showed negligible or no correlation.
DISCUSSION
Looking into human evolution, the development of an upright posture caused a curvature in neurovascular bundles at the cranial base level, and this might further worsen when kinking/kyphosis ensues due to certain craniofacial patterns which cause a further change in head posture.
Cranial base growth and skeletal jaw relations are closely dependent on each other thus prescreening such patients early in age would enable us to help susceptible patients to be referred to other medical specialists so as to correct their posture and/or treat them in a more effective manner.
CONCLUSION
Class I and III patients had evident inverse correlation between CXA and cranial base angle but the latter seem to have more statistically significant dependence. In Class II group, on the other hand, CXA was more related to Frankfurt mandibular plane and growth axis angles.
Class III group indicatively seem to be at more risk of developing future neurodegenerative disorders as compared to Class I and II skeletal malocclusion since the standard deviation for both CXA and cranial base angle (BaSN) in Class III group is large, which is enough to cause unwanted biomechanical strain on neural bundles passing through CCJ, although more evidence is required to establish such statement.
Since we orthodontists deal with cephalometrics on a regular basis, our profession can play a vital role in prescreening such cases having abnormal craniocervical abnormalities not limited just to CXA.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- The role of the craniocervical junction in craniospinal hydrodynamics and neurodegenerative conditions. Neurol Res Int. 2015;2015:794829.
- [Google Scholar]
- The beaten copper cranium: A correlation between intracranial pressure, cranial radiographs, and computed tomographic scans in children with craniosynostosis. Neurosurgery. 1996;39:691-9.
- [Google Scholar]
- Intracranial pressure monitoring in children with single suture and complex craniosynostosis: A review. Childs Nerv Syst. 2005;21:913-21.
- [Google Scholar]
- Hydrocephalus with cerebral aqueductal dysgenesis and craniofacial anomalies. Acta Neuropathol. 1984;63:170-3.
- [Google Scholar]
- A comparative cephalometric study of the cranial base in craniofacial anomalies: Part I: Tensor analysis. Cleft Palate J. 1985;22:75-87.
- [Google Scholar]
- Skull base and calvarial deformities: Association with intracranial changes in craniofacial syndromes. AJNR Am J Neuroradiol. 1996;17:619-30.
- [Google Scholar]
- Basilar impression (Platybasia): A bizarre developmental anomaly of the occipital bone and upper cervical spine with striking and misleading neurologic manifestations. Yale J Biol Med. 1939;11:487-96.
- [Google Scholar]
- Deformative stress associated with an abnormal clivo-axial angle: A finite element analysis. Surg Neurol Int. 2010;1.pii:30.
- [Google Scholar]
- Angular craniometry in craniocervical junction malformation. Neurosurg Rev. 2013;36:603-10.
- [Google Scholar]
- Inclination of the odontoid process in the pediatric Chiari I malformation. J Neurosurg. 2003;98(1 Suppl):43-9.
- [Google Scholar]
- Estimation of odontoid process posterior inclination, odontoid height, and pB-C2 line in the adult population. J Neurosurg Spine. 2014;20:172-7.
- [Google Scholar]
- Posterior odontoid process angulation in pediatric Chiari I malformation: An MRI morphometric external validation study. J Neurosurg Pediatr. 2015;16:138-45.
- [Google Scholar]
- Malformations of the craniocervical junction (Chiari type I and syringomyelia: Classification, diagnosis and treatment) BMC Musculoskelet Disord. 2009;10(Suppl 1):S1.
- [Google Scholar]
- Mechanical breaking of microtubules in axons during dynamic stretch injury underlies delayed elasticity, microtubule disassembly, and axon degeneration. FASEB J. 2010;24:1401-10.
- [Google Scholar]
- Vulnerability of central neurons to secondary insults after in vitro mechanical stretch. J Neurosci. 2004;24:8106-23.
- [Google Scholar]
- Craniocervical syndrome: Its potential role in Alzheimer’s, Parkinson’s and other diseases of the brain: Part I: Cranial hydrodynamics and the sutures. Dyn Chiropr. 2001;19:23.
- [Google Scholar]
- Blood-brain-barriers in aging and in Alzheimer’s disease. Mol Neurodegener. 2013;8:38.
- [Google Scholar]
- The craniocervical spine and multiple sclerosis, part 1 of 2. Dyn Chiropr. 2003;21:5-9.
- [Google Scholar]
- The possible role of cranio-cervical trauma and abnormal CSF hydrodynamics in the genesis of multiple sclerosis. Physiol Chem Phys Med NMR. 2011;41:1-17.
- [Google Scholar]
- Cervical vertebral anomalies in patients with obstructive sleep apnea. APOS Trends Orthod. 2015;5:262-6.
- [Google Scholar]
- The cranial base in obstructive sleep apnea. J Oral Maxillofac Surg. 1995;53:1150-4.
- [Google Scholar]




