

Translate this page into:
Do we know how much force we apply with latex intermaxillary elastics?

*Corresponding author: Elif Dilara Seker, Department of Orthodontics, Bezmialem Vakif University, Istanbul, Turkey. dilaraarsln@hotmail.com
-
Received: ,
Accepted: ,
How to cite this article: Yilmaz BS, Kara M, Seker ED, Yenidünya D. Do we know how much force we apply with latex intermaxillary elastics? APOS Trends Orthod 2021;11:191-7.
Abstract
Objectives:
The aim of our study was to evaluate the variation of the forces provided by different branded elastics and to compare the force diminution that occurs after 24-h of use in wet environment.
Materials and Methods:
Elastics from four different manufacturer (American Orthodontics [AO], USA; Dentaurum [DENT], Germany; Ormco, USA; RMO, USA) with 3/16-inch (4.8 mm) lumen diameter, and two different force degrees (medium/heavy) were included in the study with a total of eight groups of elastics. First force measurements were performed with 50 elastics of each group at various stretching distances; lumen diameter ×2 (9.52 mm), ×3 (14.28 mm), the average canine-first molar length (22.3 mm), and the canine-second molar length (38.7 mm) under room temperature and dry air conditions. In addition, ten the elastics from each group were stretched at 22.3 mm distance in a custom-made plate and kept in 37°C distilled water. Twenty-four hours later, the force measurements were repeated.
Results:
Regardless of the brand and type (medium-heavy), all the tested elastics showed variations in matter of generated forces at different stretching distances. The variation amount increased as the length of elongation increased. The lowest standard deviation values were observed for both medium and heavy DENT elastic groups. When stretched to 3 times of their lumen size, the medium and heavy elastics both produced either lower or higher forces compared to the levels of force indicated by the manufacturers. The closest mean force to the force level stated by the manufacturer was provided with medium AO (3.6 g difference) elastics and heavy RMO counterparts (7.9 g difference). A significant 20–23% reduction of force was observed in all brands, both in medium and heavy elastics after passing 24-h in aqueous environment. No significant difference was observed in matter of force degradation between groups for both medium and heavy elastics (P < 0.05).
Conclusion:
The forces exerted by intermaxillary elastics were not found to be standard and the force stated on the package is not always provided precisely. A significant force loss around 20% was observed with all the elastics after 24-h of use in wet environment at 37°C.
Keywords
Intermaxillary elastics
Orthodontic appliances
Dental materials

INTRODUCTION
The intermaxillary elastics are frequently used for many different purposes in the course of orthodontic treatments. There are produced based on natural (latex) or synthetized bases (latex-free polymers).[1] Although natural elastics can be fabricated using different vegetative extracts, Hevea Brasiliensis is the most commonly used plant in latex production.[2] Synthetic rubber polymers were developed from petrochemicals in the 1920’s and they are preferred in some specific situations such as latex allergies.[3] Although synthetic elastics have been developed, latex elastics remained more popular and are still the most widely used type of elastics in the orthodontic practice since they offer greater flexibility, lower cost, and good energy absorption characteristics providing capability to preserve better their initial dimensions. Nevertheless, physical properties of the latex elastics might be affected negatively by several factors such as saliva, pH changes, light, heat, and thermocycling.[4] The previous studies evaluating the mechanical properties of latex elastics revealed that they show the greatest force decay during the first 24-h of use.[5,6] Therefore, in the clinical practice, patients are advised to change their elastics once at least every 24-h.
| Manufacturer | Elastic Type | The force levels on elastic packs | |
|---|---|---|---|
| Ormco | Medium | 4.5 oz | 128 g |
| Heavy | 6 oz | 170 g | |
| AO | Medium | 4.5 oz | 128 g |
| Heavy | 6.5 oz | 184 g | |
| DENT | Medium | 4.5 oz | 128 g |
| Strong | 6.5 oz | 184 g | |
| RMO | Heavy | 3.5 oz | 99 g |
| Extra Heavy | 5 oz | 142 g | |
AO: American orthodontics, DENT: Dentaurum
The amount of the applied force might be especially important for some specific cases, such as periodontally compromised patients. Therefore, it is necessary that mechanical characteristics of the elastics should be well-understood by orthodontists.
The elastics are classified by the manufacturers based on the amount of force that they provide when extended at 3 times distance of their diameter. However, the force that the elastics produce may differ clinically from the indicated force levels on their packages since the force application points and the stretching distances are unique for each case. Thus, it is advised to screen the amount of generated forces with strain gauges.[7]
To the best of our knowledge, there is no former study evaluating whether the forces generated with different brands of latex elastics are in harmony with the force levels indicated on the packages. The aim of our study was to assess the mean force value produced by latex elastics from different manufacturers at different stretching distances and to compare it with the force levels indicated on elastic packages. In addition, manufacturers update the contents of elastics and aim to eliminate the existing disadvantages. Thus, our second aim was to re-evaluate the force degradation in wet environment following 24-h incubation.
MATERIALS AND METHODS
A total of eight groups of latex elastics from four different manufacturers (American Orthodontics [AO], USA, Dentaurum [DENT], Germany, Ormco, USA, RMO, USA) with the same lumen size (3/16 inch/4.8 mm), two different thicknesses (medium-heavy) were included in the study. To enhance the understandability, the terms medium and heavy were used to describe the differences in thickness of elastics for all brands. Original names and strength values are given in [Table 1].
The power analysis revealed that a sample size of 41 elastics for each group would provide more than 95% power to detect significant differences with an effect size of 0.80 and a significance level of α = 0.05.
Fifty specimens from each elastic type were randomly selected and the force levels were measured with a force gauge (GD-30 Dynamometer Gauge Dial 40–350 g, Jonard Tools, New York, USA) by stretching elastics at specific distances: Stretching to 2 times of the lumen size (9.52 mm), stretching to 3 times of the lumen size (14.2 mm), and stretching to the mean distance between upper canine and upper first molar (22.3 mm), stretching to the mean distance between upper canine and upper second molar (38.7 mm).[8] These measurements were performed in dry environment at room temperature (24°C). Each measurement was repeated 3 times by the same operator and the average value was recorded for each elastic specimen and the mean force value was calculated for each group at different distances.
The most common usage of the intermaxillary elastics is between the canines to the first molars and this distance is reported to be 22.3 mm.[8] Ten elastics, which provided a similar force to the mean force level for 22.3 mm stretching distance, were selected. After the force measurements for specimen selection, the elastics were stretched by 22.3 mm with the help of a custom-made set-up [Figure 1]. All specimens were kept submerged in distilled water at 37°C for 24-h in an incubator to evaluate the amount of force degradation after clinical usage simulation. The force measurements of elastics were repeated and recorded after the 24-h incubation period.
Statistical analysis
Statistical analysis was performed with a software (SPSS version 16.0, SPSS, Chicago, Ill). Descriptive statistics were shown as mean, standard deviation, median, minimum, and maximum. The data were tested for normality using Shapiro–Wilk test. Kruskal–Wallis test was used for comparisons among the groups. Mann–Whitney U-test was performed for binary comparisons. Wilcoxon signed-rank tests were used to compare the time-related changes of elastics’ forces. Results for P < 0.05 were considered statistically significant.
| Group | Activation Lengths | |||
|---|---|---|---|---|
| 9.52 mm | 14.28 mm | 22.3 mm | 38.7 mm | |
| n=50 | n=50 | n=50 | n=50 | |
| ORMCO (128 g–4.5 oz) |
||||
| Median | 70 | 125 | 180 | 240 |
| Minimum | 55 | 100 | 130 | 190 |
| Maximum | 80 | 140 | 200 | 275 |
| Mean | 68.6 | 122.8ab | 177.9 | 239a |
| SD | 5.1 | 7.5 | 13.6 | 15.9 |
| AO (128 g–4.5 oz) |
||||
| Median | 75 | 130 | 190 | 250 |
| Minimum | 60 | 115 | 165 | 220 |
| Maximum | 85 | 150 | 235 | 290 |
| Mean | 74 | 131.6a | 192 | 249.9a |
| SD | 4.7 | 7.5 | 13.1 | 14.4 |
| DENT (128 g–4.5 oz) |
||||
| Median | 70 | 120 | 180 | 240 |
| Minimum | 60 | 110 | 160 | 215 |
| Maximum | 85 | 140 | 210 | 270 |
| Mean | 68.8 | 122.3ab | 178.8 | 240.7a |
| SD | 4.6 | 7.9 | 11.1 | 15.7 |
| RMO (99 g–3.5 oz) |
||||
| Median | 70 | 120 | 190 | 340 |
| Minimum | 60 | 105 | 155 | 260 |
| Maximum | 80 | 135 | 215 | 370 |
| Mean | 68.8 | 121.6b | 187.7 | 336.9b |
| SD | 4.2 | 6.1 | 11.3 | 24.2 |
| Mean SD | 4.7 | 7.3 | 11.8 | 17.6 |
| P-value | NS | <0.001 | NS | <0.001 |
AO: American orthodontics, DENT: Dentaurum, SD: Standard deviation, NS: Non-significant, unshared letters indicate significant differences between groups, Kruskal-Wallis and Mann-Whitney U tests were used for comparisons among the groups. a,bUnshared letters indicate significant differences between group

- The latex elastics placed on the mechanism with screws at a standard 22.3 mm distance.
RESULTS
[Tables 2 and 3] show the mean force levels at different stretching distances of different elastic groups. The lowest standard deviation values were observed for both medium and heavy DENT elastic groups. The forces provided by the elastics showed greater variability since the standard deviations increased in harmony with the increasing the stretching distances.
Statistical analysis revealed significant differences between the medium elastics’ groups at the stretching distances of 14.28 mm and 38.7 mm (P < 0.001). On the other hand, no statistical difference was observed in the stretching distances of 9.52 mm and 22.3 mm (P > 0.05, Table 1). The comparison between groups of heavy elastics showed statistically significant differences for all stretching distances (P < 0.001, Table 2).
The force levels indicated by the manufacturers on the package are known to be the force amounts provided when the elastics are extended at 3 times of the lumen size (14.28 mm for 3/16-inch elastics).[7] [Figures 2 and 3] present the mean force values recorded when the elastics were stretched at 3 times distance of the lumen size and the force levels indicated on the packages for medium and heavy elastics. The medium elastic group that provided the closest mean force to the force level stated by the manufacturer (3.6 g difference) was fabricated by AO. On the other hand, the closest force levels to the one indicated on the package were provided by the Dentarum samples among the heavy elastics (18 g difference).
Statistically significant changes after 24-h stretching in 37°C distilled water was observed between the force levels recorded before and after incubation for both medium and heavy elastics (P < 0.05, Table 4). On the other hand, no significant differences were observed in force degradation among groups for both medium and heavy elastics (P < 0.05, Table 5). The percentage of force loss in medium and heavy elastics over time ranged from 20% to 23%. The force measurements performed with medium elastics in the wet media revealed a smaller standard deviation compared to the one recorded with the heavy elastics [Tables 4 and 5].
DISCUSSION
Even though in vitro conditions may not perfectly simulate the oral conditions, these investigations may still provide a better understanding for many clinical applications as well as intermaxillary elastics usage.[9] In the present study, latex elastics (medium and heavy) from four different manufacturers with the same lumen size (3/16 inch/4.8 mm) were evaluated in both dry and wet environments.
| Group | Activation lengths | |||
|---|---|---|---|---|
| 9.52 mm | 14.28 mm | 22.3 mm | 38.7 mm | |
| n=50 | n=50 | n=50 | n=50 | |
| ORMCO (170 g–6 oz) | ||||
| Median | 110 | 195 | 280 | 360 |
| Minimum | 95 | 170 | 250 | 320 |
| Maximum | 120 | 225 | 325 | 420 |
| Mean | 107.7b | 193bc | 281.7bc | 363.4b x |
| SD | 6.4 | 12.2 | 16.3 | 24 |
| AO (184 g–6.5 oz) | ||||
| Median | 110 | 205 | 300 | 400 |
| Minimum | 90 | 170 | 245 | 330 |
| Maximum | 125 | 230 | 340 | 450 |
| Mean | 111.4b | 205.5b | 300.1b | 397.6 β |
| SD | 7.7 | 13.9 | 23 | 30.5 |
| DENT (184 g–6.5 oz) | ||||
| Median | 90 | 165 | 250 | 340 |
| Minimum | 75 | 115 | 215 | 295 |
| Maximum | 105 | 200 | 300 | 410 |
| Mean | 90.7ac | 165.2ac | 252.3ac | 340.7ac |
| SD | 5.9 | 13 | 15.7 | 20.3 |
| RMO (142 g–5 oz) | ||||
| Median | 85 | 150 | 235 | 385 |
| Minimum | 65 | 110 | 190 | 300 |
| Maximum | 100 | 185 | 275 | 460 |
| Mean | 83a | 149.8a | 234.3a | 383.4a |
| SD | 8.3 | 15.2 | 19.5 | 35.8 |
| Mean SD | 7.1 | 13.6 | 18.6 | 27.6 |
| P-value | <0.001 | <0.001 | <0.001 | <0.001 |
AO: American orthodontics, DENT: Dentaurum, SD: Standard deviation, NS: Non-significant, unshared letters indicate significant differences between groups, Kruskal-Wallis and Mann-Whitney U tests were used for comparisons among the groups. a,b,cUnshared letters indicate significant differences between group
| Group | Immediately after stretching | After a 24-h period of stretching | P-value | Force degradation (%) |
|---|---|---|---|---|
| n=10 | n=10 | |||
| ORMCO-H (128 g–4.5 oz) | ||||
| Median | 175 | 132.5 | 0.004* | 22.92% |
| Minimum | 170 | 125 | ||
| Maximum | 180 | 145 | ||
| Mean | 174.5 | 134.5 | ||
| SD | 4.3 | 6.4 | ||
| AO-H (128 g–4.5 oz) | ||||
| Median | 185 | 147.5 | 0.004* | 20.1% |
| Minimum | 175 | 135 | ||
| Maximum | 195 | 155 | ||
| Mean | 184 | 147 | ||
| SD | 6.5 | 6.3 | ||
| DENT-H (128 g–4.5 oz) | ||||
| Median | 175 | 137.5 | 0.004* | 22.0% |
| Minimum | 170 | 130 | ||
| Maximum | 185 | 150 | ||
| Mean | 175 | 136.5 | ||
| SD | 5.2 | 6.6 | ||
| RMO-H (99 g–3.5 oz) | ||||
| Median | 180 | 140 | 0.004* | 22.37% |
| Minimum | 170 | 130 | ||
| Maximum | 190 | 150 | ||
| Mean | 181 | 140.5 | ||
| SD | 6.1 | 5.5 | ||
| P-value | NS |
AO: American orthodontics, DENT: Dentaurum, SD: Standard deviation, NS: Non significant, *P<0.01, Wilcoxon signed-rank test was used for comparisons between the time-related changes
Former studies focused on the force levels provided with intermaxillary elastics commonly stretched the elastics 2 or 3 times of the lumen size as reference distances.[9,10] Kanchana and Godfrey[9] evaluated the force levels of the latex elastics at extension lengths varying from 20 mm to 40 mm in a wet environment. Moreover, he evaluated activation lengths varying between 15 mm and 60 mm for the force measurements in dry condition. Mansour[8] calculated the mean distances from canine to the first molar and from canine to the second molar to base his experiments to the clinical scenario and he evaluated the force degradation of the elastics at the mean canine-molar distances. In the present study, we measured the force levels at four different stretching lengths referring to former studies: 2 times of the lumen size (9.52 mm), 3 times of the lumen size (14.2 mm), the mean distance between upper canine and upper first molar (22.3 mm), and the mean distance between upper canine and upper second molar (38.7 mm). We found that the force deviations increase as stretching distance increases and that when stretched to 3 times of their lumen size, the closest mean force to the force level stated by the manufacturer was provided with medium AO (3.6 g difference) elastics and heavy RMO (7.9 g difference).
In clinical conditions, some patients state that some elastics break through usage requiring replacement and that some elastics from the same package are often thinner or thicker than the others. Accordingly, it was formerly reported that when stretched at the same length, the force values produced by the same type of elastics show variations.[9,11] The previous studies suggested that these differences may have been due to the dimensional differences such as cross-sectional area and the inner diameter of the elastics.[12-14] Mansour[8] measured the force level of elastics from three different manufacturers at three different activation length and reported similarly a large variation in force. Other than the dimensional differences, the authors suggested that the reason for this variation may be the lack of standardization in the manufacturing process. We evaluated a larger total number of the elastics in the present study compared to other similar studies.[12-14] We found statistical differences between the force levels of elastics (for both medium and heavy elastics) from four different manufacturers (P < 0.05). We also observed that the standard deviation of the force values increased while the stretching lengths increased. These findings are in harmony with the results of the study by Mansour.[8]
| Group | Immediately after stretching | After a 24-h period of stretching | P-value | Force degradation (%) |
|---|---|---|---|---|
| n=10 | n=10 | |||
| ORMCO-H (170 g–6 oz) | ||||
| Median | 260 | 207.5 | 0.004* | 20.65% |
| Minimum | 250 | 200 | ||
| Maximum | 270 | 220 | ||
| Mean | 261.5 | 207.5 | ||
| SD | 7 | 7.9 | ||
| AO-H (184 g–6.5 oz) | ||||
| Median | 292.5 | 225 | 0.004* | 21.89% |
| Minimum | 280 | 220 | ||
| Maximum | 300 | 235 | ||
| Mean | 290 | 226.5 | ||
| SD | 7 | 4,7 | ||
| DENT-H (184 g–6.5 oz) | ||||
| Median | 242.5 | 190 | 0.004* | 22.08% |
| Minimum | 230 | 180 | ||
| Maximum | 255 | 205 | ||
| Mean | 244.5 | 190.5 | ||
| SD | 8.9 | 7.6 | ||
| RMO-H (142 g–5 oz) | ||||
| Median | 230 | 180 | 0.004* | 20.84% |
| Minimum | 210 | 170 | ||
| Maximum | 235 | 190 | ||
| Mean | 225.5 | 178.5 | ||
| SD | 7.9 | 6.2 | ||
| P-value | NS |
AO: American orthodontics, DENT: Dentaurum, SD: Standard deviation, NS: Non significant, *P<0.01, Wilcoxon signed-rank test was used for comparisons between the time-related changes
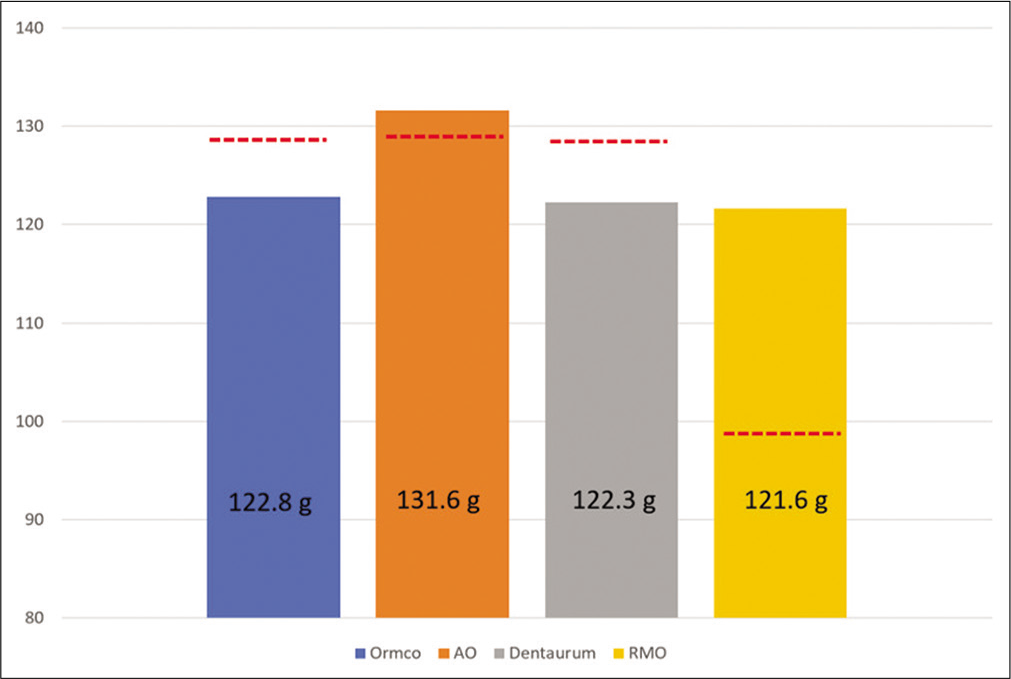
- Comparison graphs of recorded mean force level at 3 times the lumen size extension with force levels on packs stated by manufacturers for medium elastics. Dashed lines represent the force levels stated by manufacturers.
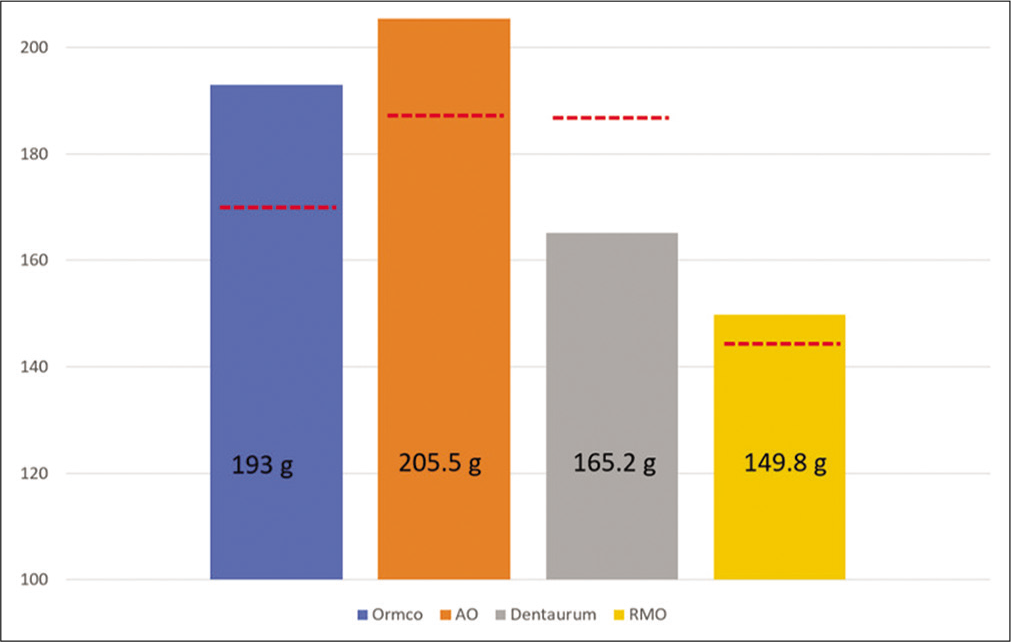
- Comparison graphs of recorded mean force level at 3 times the lumen size extension with force levels on packs stated by manufacturers for heavy elastics. Dashed lines represent the force levels stated by manufacturers.
Former studies compared the forces generated with elastics with those indicated on the packages by the manufacturers and there are conflicting results. Many studies reported that the generated forces were higher than the force levels defined on the packs.[12,15] On the other hand, some authors reported the lower force levels compared to the ones written on the packs.[9,13,16] We observed that the majority of the medium and the heavy elastics produced lower and some of them produced higher forces compared to the amount of force defined on their package. These differences may be dependent brand of the elastic and on the standardization in the production process.
It was previously reported that majority of force degradation occurs within the first 24-h and most of the clinicians advise to replace the elastics at least once a day.[17] Therefore, the force degradation of the elastics was evaluated after 24-h period in the present study and the force decrease ranged from 20% to 23% for both medium and heavy elastics. Paulich[10] tested the elastics with three different diameters from three different brands following 24-h in wet conditions. He reported similarly that when the elastics were stretched to 2 times their lumen size, the force degradation after 24-h was 13–23%. On the other hand, Kanchana and Godfrey[9] reported that the tested elastics showed 32.3% of force loss. The reason why the force loss is higher in Kanchana’s study compared with our results may be explained that we tested the elastics with a longer activation distance. Yang et al.[18] incubated the elastics in a 37°C artificial saliva and they reported about 34% force degradation. A possible explanation for the higher amount of force loss compared to our findings may be the deteriorating enzymatic activity of the saliva on the elastics. Thus, distilled water usage can be considered as a limitation of the present study.
The application of the appropriate amount of force for the desired orthodontic tooth movement is one of the critical factors in clinical orthodontics. Heavy forces might indesirable harmful effects to teeth and the surrounding tissues. On the other hand, the forces that remain beyond the minimum required level are unable to start the tooth movement. The orthodontists should well-understand the forces that apply and the force diminution characteristics of the latex elastics. This study proved that the force generated with of the same type of elastics showed variations. Therefore, the manufacturers need to apply strict quality control mechanisms and standardization methods. The mean amount of force variation may also be indiated on the packages to help clinicians. We may advise clinicians to screen the force level of the elastics in cases who need special care such as root resorption affinity or periodontal damage. Further studies may be performed to test the force degradation characteristics of orthodontic latex and non-latex elastics with different dimensions in different environments.
Finally, a number of limitations of this study need to be considered. Different environment conditions may have different effects on the forces provided by orthodontic latex elastics. The characteristics of elastics are influenced by many variables such as oral liquid environment, oral temperature, saliva, and types of foods.[3] Thus, in vitro studies could be unable to represent precisely the oral environment. Since orthodontic patients are routinely instructed to wear the latex elastics for 24-h, except eating and brushing teeth, the effects of the diet can be neglected within the scoop of the present study. Furthermore, Paige et al.[19] aimed to compare the force loss of medium latex elastics to non-latex elastics from two companies after being cycled between different temperatures. The authors suggested that heat reduce the force of latex and non-latex elastics even when cycled for brief periods of time. Although they are removed during eating and drinking, elastics are stretched at different distances in clinical conditions.[9,20] Kersey et al.[21] made a comparative study evaluating the force decay when elastics undergo repeated stretching and static testing. They reported that cyclic testing caused significantly more force decay (approximately 10%). Liu et al.[22] evaluated the properties and strength loss of elastics at different stretching distances and stated that the normal range of clinical use is between 20 and 50 mm. They reported that there was no statistical difference in the force or compliance measurements after the elastics were stretched more than 200 times. When stretched for 1000 cycles of 400% extension, they found that the force was reduced by approximately 12%. The use of static stretching distance in our study (22.3 mm) during the incubation period can be considered as a limitation.
CONCLUSION
The forces exerted by intermaxillary elastics were not found to be standard and the force stated on the package was not always provided precisely.
Regardless of the brand and type (medium-heavy) of the elastics, variations in the force level were observed at all stretching distances. On the other hand, the value of the standard deviation of the force increased when the activation length of the elastics increased.
When the elastics were stretched to 3 times of their lumen size, the medium and heavy elastics from four different manufacturers produced either lower or higher forces compared to the ones indicated by the manufacturers.
Statistically significant force degradations ranging from 20% to 23% were found with all elastics (for both medium and heavy forces) after passing 24-h in wet conditions.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- The effect of pH levels on nonlatex vs latex interarch elastics. Angle Orthod. 2011;81:1070-4.
- [CrossRef] [PubMed] [Google Scholar]
- Farklı Kauçuk Karısşımlarının Vulkanizasyonuna Hızlandırıcıların Etkisi. SAÜ Fen Bilimleri Enstitüsü Yüksek Lisans Tezi.
- [Google Scholar]
- An in vitro study simulating effects of daily diet and patient elastic band change compliance on orthodontic latex elastics. Angle Orthod. 2004;74:234-9.
- [Google Scholar]
- Evaluation of force degradation characteristics of orthodontic latex elastics in vitro and in vivo. Angle Orthod. 2007;77:688-93.
- [CrossRef] [PubMed] [Google Scholar]
- Force extension relaxation of medium force orthodontic latex elastics. Angle Orthod. 2011;81:812-9.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of the cytotoxicity of latex and non-latex orthodontic separating elastics. Orthod Craniofac Res. 2010;13:28-33.
- [CrossRef] [PubMed] [Google Scholar]
- Perceived vs measured forces of interarch elastics. Am J Orthod Dentofacial Orthop. 2012;141:298-306.
- [CrossRef] [PubMed] [Google Scholar]
- A comparison of orthodontic elastic forces: Focus on reduced inventory. J Orthod Sci. 2017;6:136-40.
- [CrossRef] [PubMed] [Google Scholar]
- Calibration of force extension and force degradation characteristics of orthodontic latex elastics. Am J Orthod Dentofacial Orthop. 2000;118:280-7.
- [CrossRef] [PubMed] [Google Scholar]
- Mechanical properties intermaxillary latex and latex-free elastics. J World Fed Orthod. 2013;2:e15-8.
- [CrossRef] [Google Scholar]
- In vitro assessment of the mechanical properties of latex and non-latex orthodontic elastics. Am J Orthod Dentofacial Orthop. 2001;120:36-44.
- [CrossRef] [PubMed] [Google Scholar]
- An in vitro comparison of 4 brands of nonlatex orthodontic elastics. Am J Orthod Dentofacial Orthop. 2003;123:401-7.
- [CrossRef] [PubMed] [Google Scholar]
- Force-extension characteristics of orthodontic elastics. Am J Orthod. 1977;72:296-302.
- [CrossRef] [Google Scholar]
- A study of force extension and force degradation of orthodontic latex elastics: An in vitro study. APOS Trends Orthod. 2013;3:184-9.
- [CrossRef] [Google Scholar]
- Force degradation of orthodontic latex elastics: An in vivo study. Am J Orthod Dentofacial Orthop. 2017;151:507-12.
- [CrossRef] [PubMed] [Google Scholar]
- Force degradation of orthodontic latex elastics analyzed in vivo and in vitro. Am J Orthod Dentofacial Orthop. 2020;157:313-9.
- [CrossRef] [PubMed] [Google Scholar]
- Latex and non-latex orthodontic elastic force loss due to cyclic temperature. Tex Dent J. 2011;128:541-5.
- [Google Scholar]
- Force relaxation characteristics of medium force orthodontic latex elastics: A pilot study. ISRN Dent. 2011;53:60-89.
- [CrossRef] [PubMed] [Google Scholar]
- A comparison of dynamic and static testing of latex and nonlatex orthodontic elastics. Angle Orthod. 2003;73:181-6.
- [Google Scholar]
- The effect of repeated stretching on the force decay and compluance of vulcanized cispolyisoprene orthodontic elastics. Dent Mater. 1993;9:37-40.
- [CrossRef] [Google Scholar]




