

Translate this page into:
Effect of proclination of the upper incisors on Point A in adult Class II division 2 individuals: A cephalometric study

*Corresponding author: A. T. Prakash, Department of Orthodontics and Dentofacial Orthopedics, Bapuji Dental College and Hospital, Davangere, Karnataka, India. atportho@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Prakash AT, Zoheb M, Priyanka S. Effect of proclination of the upper incisors on Point A in adult Class II division 2 individuals: A cephalometric study. APOS Trends Orthod, doi: 10.25259/APOS_26_2022
Abstract
Objectives:
The study aimed to identify and evaluate changes in the cephalometric position of Point A due to an incisal inclination change caused by orthodontic treatment in non-growing Class II division 2 patients.
Material and Methods:
A total of 24 pairs of consecutive pre-treatment and post-treatment lateral cephalograms were systematically collected from the departmental database and hand traced. The total change in the position of Point A was investigated by superimposing pre-treatment and post-treatment lateral cephalograms at a stable basicranial line. The treatment changes in maxillary incisor inclination, the sagittal position of Point A, SNA angle, movement of incisor root apex, and incisal edge were calculated.
Results:
The mean SNA angle was reduced significantly suggesting that the A point had moved backward solely due to orthodontic remodeling. Point A distance to true vertical was reduced significantly (mean 1.2 mm), suggesting that local remodeling has occurred due to orthodontic treatment. The incisal edge also moved forward significantly (mean 2.6 mm). The apex of the upper incisor moved significantly backward as a result of its counterclockwise rotation (mean 3.2 mm). The upper incisor to palatal plane values also showed a highly significant change in inclination of the upper incisors (mean 12.30).
Conclusion:
Counter-clockwise rotation of the upper incisor causing its root apex to move more palatally makes remodeling changes in Point A in the form of its retraction roughly by one-third the amount of the backward movement of the upper incisors’ root apex. Moreover, it can be inferred that the retraction of Point A in millimeters will roughly be equal to the reduction in SNA angle in degrees.
Keywords
Class II division 2
Point A
Maxillary incisor proclination
Incisal inclination
Dentoalveolar remodeling

INTRODUCTION
Malocclusions in the human race and attempts to treat these conditions have been apparent since early civilization. The depiction or classification of a condition is an important precondition to define the prevalence or severity of that condition in the human population. Although several attempts were made throughout the 19th century to classify malocclusions, it was not until the end of that century that an extensively acknowledged classification became important to the dental profession. Based on the anteroposterior occlusal relationship of the first permanent molar, Dr. Edward H. Angle described three classes of malocclusion in 1899.
Class I malocclusion or neutro-occlusion.
Class II malocclusion or disto-occlusion, is characterized by mandibular first molar occluding distal to the normal relationship with the maxillary first molars. Angle further differentiated the Class II malocclusion into division 1 in which the maxillary incisors are protrusive and division 2 in which the maxillary incisors are retrusive.
Class III malocclusion or mesio-occlusion.
Steady correction of Class II division 2 incisor relationship is challenging as it entails correction of deep bite as well as reduction of inter-incisal angle. In a Class II division 2 malocclusion, the inter-incisal angle can be reduced by:
Torqueing the roots of incisors palatally with a fixed appliance.
Proclination of the upper incisors that is followed by the use of a functional or fixed appliance to reduce the subsequent overjet.
Combination of the above approaches.
The treatment approach for a particular patient will be contingent on the etiology as well as clinical and cephalometric findings.
Cephalometry is a commonly used tool for diagnosis and treatment planning in orthodontics. Several researchers have developed many different methods of analysis for use during diagnosis and treatment planning. Of all these methods, the principal method of measuring encompasses angular and linear measurements which are taken between the cephalometric points. The results are then compared and appraised with the norm.
Achieving an ideal skeletal and denture stability is the most challenging problem in orthodontics. This problem is overstated when there is a poor orientation of the maxillary and mandibular apical bases. In cephalometric analysis, Point A and Point B represent the two jaw bases, respectively, which were first described by Riedal.[1]
The sagittal position of the maxilla represented as Point A is defined as the most concave point on the anterior border of the maxilla. Many of the prevalent analyses use this point due to its easy and accurate identifiability. However, Point A has also been reflected to be an undependable landmark as it is predisposed to growth, dentoalveolar remodeling, and also orthodontic tooth movement.
Several studies have reported a significant association between the position of Point A and the axial inclination of the upper incisors.[2-6] A study conducted by Al-Nimri et al.[7] concluded that the position of Point A was affected by local bone remodeling associated with proclination of the upper incisor in Class II Division 2 malocclusion. However, the drawback of this study was that growing individuals were included in the sample.
Hence, to evaluate the effect of any tooth movement on skeletal structures, studies should be conducted on non-growing individuals. Furthermore, much attention has not been given to the effect of counter-clockwise rotation of the upper incisors on alveolar bone remodeling that causes changes in the position of Point A. Therefore, the present study aims to evaluate the effect of the proclination of maxillary incisors on the sagittal position of Point A in non-growing Class II division 2 incisor relation subjects as a result of orthodontic treatment. In addition, correlation of several factors that may affect the changes in the position of Point A following upper incisor proclination such as the age of the patient, sex, initial incisor inclination, initial incisor position, and degree of counter-clockwise rotation of incisor at the end of the treatment was established.
MATERIAL AND METHODS
Sample size determination
A pilot study was conducted with n = 5, to determine the sample size. Based on the pilot study, the average mean difference of true vertical to Point A was 0.7 mm and a standard deviation of 1.2 mm was used in sample size calculation. The formula below[8] was used to determine the sample size, which was calculated to be 23.07. It was then rounded to 24.
α (two-tailed) = 0.05 and Za = 1.960
β = 0.200 and β = Zβ = 0.842
Effect Size (E) for VertT-A = 0.7
S (∆) = 1.2
A = 1.000 B = (Zα + Zβ)2 = 7.849
C = (E/S [∆])2 = 0.340
AB/C = 23.07
Data collection
The study group consists of lateral cephalograms of 24 subjects who had Class II division 2 malocclusion.
Criteria for selection of patients
The criteria for the selection of patients in the study groups were as follows:
Inclusion criteria
The following criteria were included in the study:
Both pre-treatment and post-treatment lateral cephalograms were taken from the same X-ray machine.
Subjects with Stage 6 of Hassel and Farman cervical maturity indicator.
Post-treatment maxillary incisors parallel or ±2 degrees to the Ricketts facial axis.
Non-extraction treatment plan of Class II division 2 type of incisor relation.
Exclusion criteria
The following subjects were excluded from the study:
Subject with syndromes that influence the craniofacial region.
Previous orthodontic treatment.
Missing maxillary incisors.
Supernumerary tooth/any other pathology in the anterior maxillary region.
Analysis of lateral cephalograms
Lateral cephalograms were taken under standardized conditions with a cephalostat. Each cephalogram was taken with the patient’s teeth in habitual occlusion and lips at rest position. Standardization was done by taking the cephalograms with the same machine, that is, Orthoralix 9200 by Gendex in the Department of Oral Medicine and Radiology of Bapuji Dental College and Hospital, Davangere. Tracings were made on 0.003 inch thick acetate paper with 0.3 mm lead pencil and the landmarks were identified. Midpoints of the right and left images were used for bilateral landmarks. Angular measurements were recorded with a protractor to a nearest of 1 degree and linear measurements were made with a ruler to the nearest of 1 mm.
Parameters used [Figure 1]:

- Cephalometric landmarks and planes used in this study.
SNA angle: Angle formed by the intersection of the nasion-sella and nasion-point A-lines.
U1-palatal plane angle (U1-PP): Angle formed by the intersection of the long axis of the maxillary incisors and the anterior nasal spine – posterior nasal spine line.
Vert T-U1Ap: Perpendicular distance from the maxillary incisors root apex to the vertical reference line.
Vert T-A distance: Perpendicular distance from Point A to the vertical reference line.
Vert T-U1Ed: Perpendicular distance from the incisal edge of the maxillary incisor to the vertical reference line.
Method of study
All pre-treatment and post-treatment radiographs used in the present study were taken from the same X-ray machine. To determine the errors associated with cephalometric measurements, all the cephalograms were hand traced twice by two separate investigators at a gap of 1 week. A vertical reference line (Vert T) was used as a reference plane constructed through a stable craniofacial structure, that is, the stable basicranial line (SBL). SBL is traced through the most superior point of the anterior wall of the sella tursica at the junction with tuberculum sellae (Point T) and it was drawn tangent to the cribriform plate of ethmoid bone (lamina cribrosa). Vert T is constructed perpendicular to SBL and passes through Point T.[9]
Statistical analysis
The data were compiled systematically in a Microsoft Excel sheet and subjected to statistical analysis. Based on the normality of the data, the values obtained were statistically analyzed using the following tests:
Paired t-test was employed to compare the difference between pre-treatment and post-treatment values.
Unpaired t-test was employed to compare the difference between the changes in the position of Point A in males and females.
Pearson’s correlation was used to assess the correlation between changes in Point A position and age, initial incisor inclination, initial incisor position, and degree of counter-clockwise rotation of the upper incisors whereas Spearman’s correlation was used to find a correlation between sex and change in Point A position.
P < 0.05 was considered statistically significant.
RESULTS
The present study evaluates the effect of maxillary incisor proclination on the sagittal position of Point A on non-growing Class II division 2 subjects as a result of orthodontic treatment. The present study consists of 24 subjects who had Class II division 2 malocclusion, Stage 6 of Hassel and Farman cervical maturity indicator, and post-treatment maxillary incisors parallel to or ±2 degrees to the Ricketts facial axis. All pre-treatment and post-treatment cephalograms were analyzed. A total of six parameters were used in this study. Based on the normality of the data, the values obtained were statistically analyzed using the Paired t-test to compare the changes between the pre-treatment and post-treatment. “P = 0.05” or less was considered for the differences to be statistically significant. The arithmetic mean and standard deviation values were calculated for all the measured cephalometric variables. The intergroup comparison is shown in [Table 1 and Figures 2-6].
| Pre (n=23) | Post (n=23) | t | df | P value | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||||
| SNA° | 82.6 | 3.24 | 81.6 | 3.08 | 3.28 | 22 | 0.003** |
| U1-PP° | 102.3 | 7.09 | 114.6 | 8.81 | 6.42 | 22 | <0.001*** |
| Vert T-U1Ap (mm) | 62.7 | 6.03 | 59.5 | 6.56 | 5.84 | 22 | <0.001*** |
| Vert T-A distance (mm) | 66.3 | 6.13 | 65.1 | 6.80 | 3.15 | 22 | 0.005** |
| Vert T-U1Ed (mm) | 65.4 | 7.13 | 68.0 | 8.26 | 3.34 | 22 | 0.003** |

- Intergroup comparison of SNA
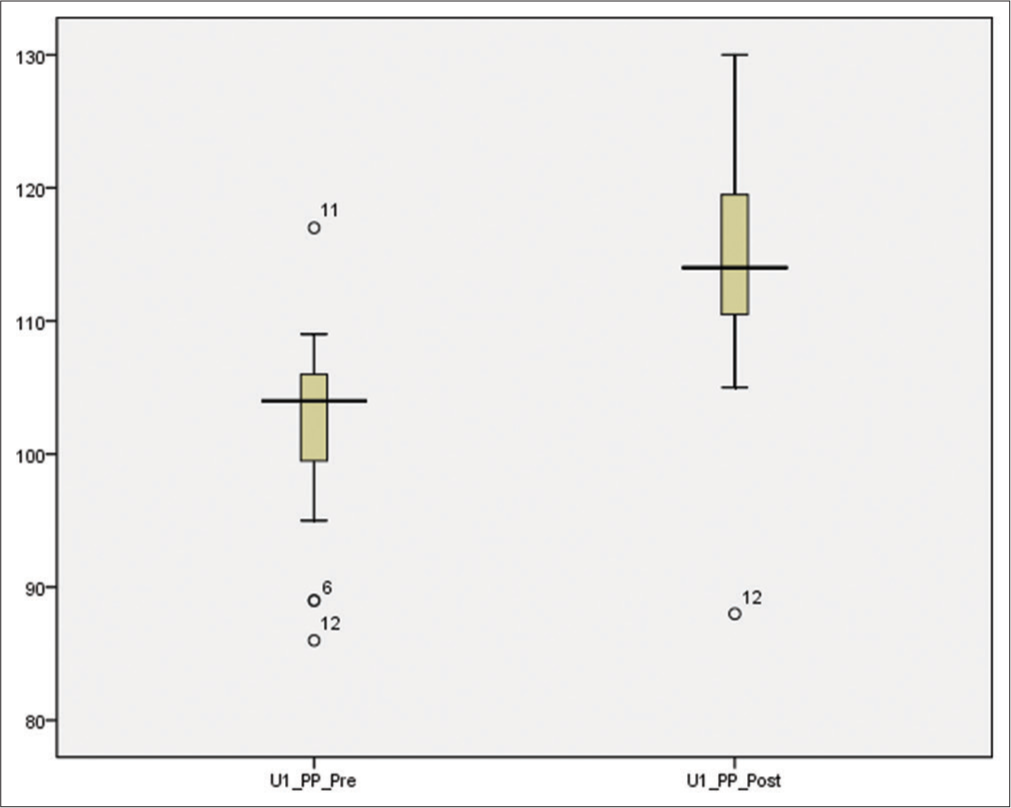
- Intergroup comparison of U1-PP?
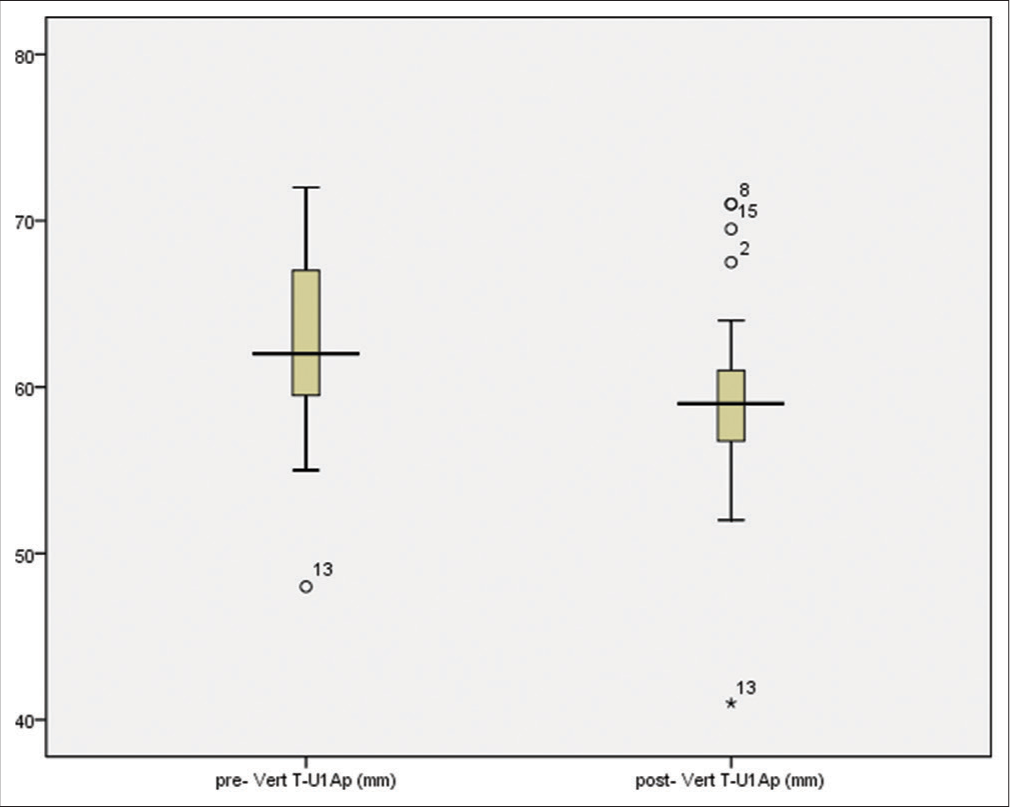
- Intergroup comparison of Vert T-U1Ap (mm).
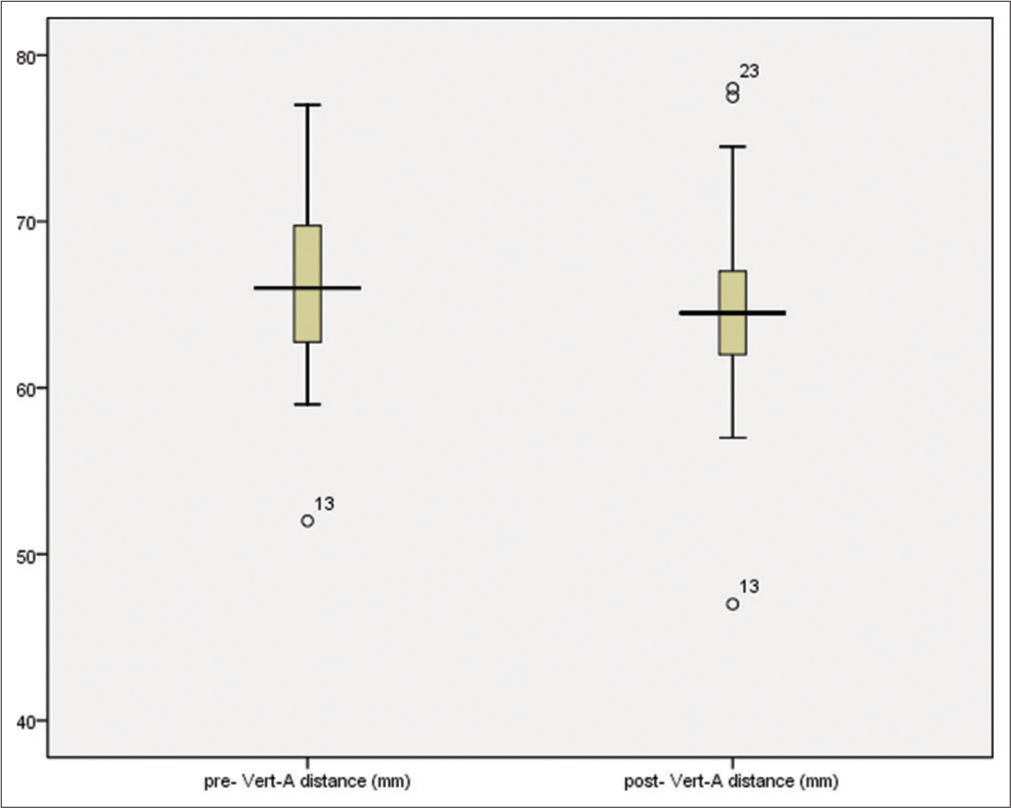
- Intergroup comparison of Vert T-A distance (mm).
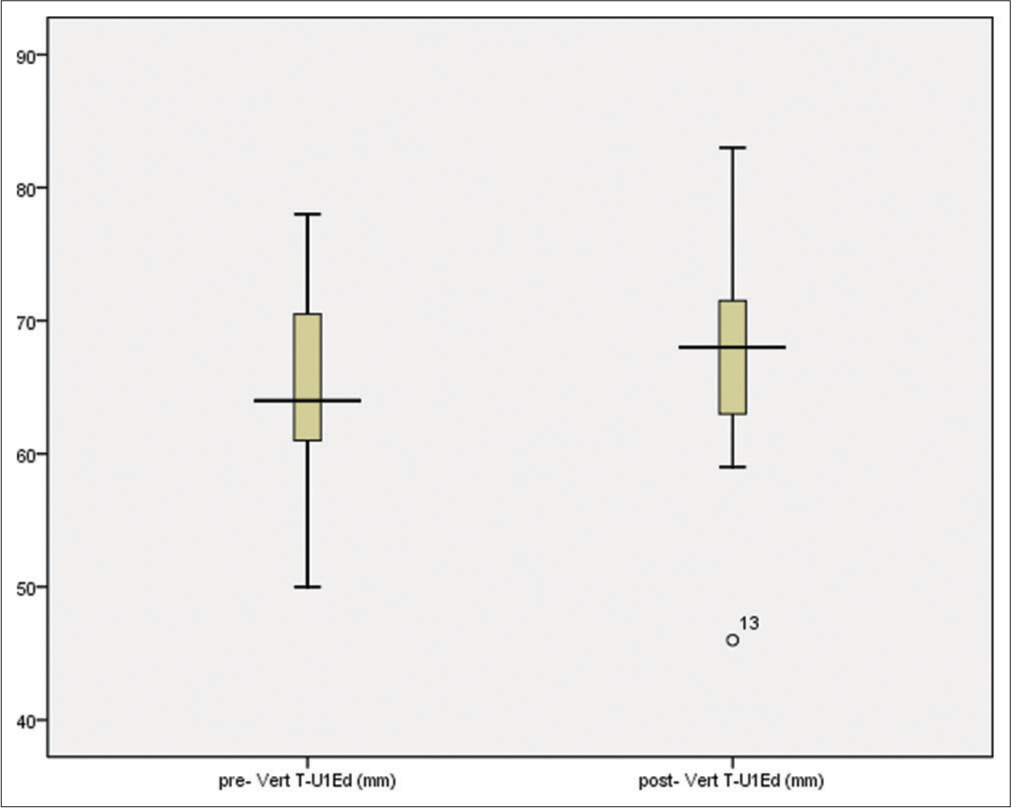
- Intergroup comparison of Vert T-U1Ed (mm).
SNA (°)
In pre-treatment, the mean angular measurement was 82.60 while in the post-treatment, the angle had reduced to 81.60. The intergroup comparison [Figure 2] showed that the change in angular measurement between the two groups was significant (P = 0.003).
U1-PP (°)
In the pre-treatment group, the mean upper incisors to palatal plane angle were 102.30. The post-treatment angle was increased to 114.60. The intergroup comparison [Figure 3] showed that the change between the groups was significant (P = 0.001).
Vert T-U1Ap (mm)
In the pre-treatment group, the mean linear measurement of the upper incisor apex to the true vertical was 62.7 mm while the post-treatment mean was reduced to 59.5 mm. The intergroup comparison [Figure 4] showed that the change between the groups was significant (P = 0.001).
Vert T- A distance (mm)
In the pre-treatment group, the mean linear measurement of Point A to the true vertical was 66.3 mm while the post-treatment mean was reduced to 65.1 mm. The intergroup comparison [Figure 5] showed that the change between the groups was significant (P = 0.005).
Vert T- U1Ed (mm)
In the pre-treatment group, the mean linear measurement of the upper incisal edge to the true vertical was 65.4 mm while the post-treatment mean was increased to 68 mm. The intergroup comparison [Figure 6] showed that the change between the groups was significant (P = 0.003).
Table 2 represents the comparison of changes in the position of Point A following incisor proclination in males and females. The mean change in the position of Point A following upper incisor proclination was found to be more in female subjects as compared to males. However, the results were not statistically significant (P = 0.89). On establishing the correlation of several factors that might affect the position of Point A on proclination of the upper incisors, it was found that the age of the patient (r = −0.04) and initial incisor position (r = −0.2) were negatively correlated whereas patient gender (r = 0.01), initial incisor inclination (r = 0.01), and the degree of counter-clockwise rotation of the incisor at the end of the treatment (r = 0.28) were positively correlated with the amount of change in the position of Point A. Nevertheless, none of the variables were statically significant (P > 0.005). The same is represented in Table 3.
| Mean (in mm) | S D | t value | df | P value | Mean deviation | Confidence interval | |
|---|---|---|---|---|---|---|---|
| Males (n=10) | −1.22 | 1.56 | 0.138 | 21 | 0.89 | 0.099 | −1.39–1.59 |
| Females (n=14) | −1.32 | 1.74 |
| Changes in the position of Point A | ||
|---|---|---|
| Correlation value (r) | P value | |
| Sex | 0.01 | 0.95 |
| Age of the patient | −0.04 | 0.84 |
| Initial incisor inclination | 0.01 | 0.95 |
| Initial incisor position | −0.2 | 0.35 |
| Degree of counter-clockwise rotation of incisor | 0.28 | 0.19 |
DISCUSSION
Local bone remodeling associated with proclination of the upper incisors in Class II division 2 malocclusion influences the position of Point A. Variations in the position of Point A can be ascribed to skeletal changes ensuing from the movement of the maxilla relative to the anterior cranial base (growth), and local changes instigated by local bone remodeling attendant to orthodontic proclination or retroclination of the upper incisors. In the present study, the positional change of Point A due to growth was eliminated by the fact that only adult non-growing cases were selected. Therefore, any change in the position of Point A was solely due to the orthodontic treatment.
In the present study, the total change in the position of Point A was investigated by superimposing pre-treatment and post-treatment lateral cephalogram at SBL. SBL was delineated as consisting of structures that do not undergo remodeling after the age of 4–5 years.[9] All the subjects were in Stage 6 of Hassel and Farman’s skeletal maturity, which suggests that no active growth was remaining.[10] The results of this research indicated that noteworthy changes were perceived in the position of the upper incisor to the palatal plane, the apex of the upper incisors to the true vertical representing that the incisors were rotated counter-clockwise to an ideal position during the treatment, correcting the Class II division 2 malocclusion to an ideal overjet.
The mean SNA angle had decreased from pre-treatment to post-treatment suggesting that the A point had moved backward solely due to orthodontic remodeling. This change in the SNA angle from pre-treatment to post- treatment was statistically significant and is opposite to the finding of Al-Nimri et al.[7] probably because of their sample which included growing patients. Point A distance to true vertical has reduced from pre-treatment to post-treatment (mean 1.2 mm), proposing that local remodeling has occurred due to orthodontic treatment. Similar significant changes were noticed with the incisal edge moving forward from pre-treatment to post-treatment (mean 2.6 mm). The apex of the upper incisor also moved significantly backward as a result of counter-clockwise rotation (mean 3.2 mm). The upper incisor to palatal plane values also showed a highly significant change in inclination of the upper incisors (mean 12.30).
The present study is in contrast to the study by Bicakci et al.[2] who overestimated the backward movement of Point A by around half the incisor root apex, probably because more incisor proclination than torqueing of retroclined incisors were carried out in their study subjects.
CONCLUSION
The position of Point A is affected by local bone remodeling associated with proclination of the upper incisor in Class II division 2 malocclusion, and this change significantly affects the value of the SNA angle.
Counter-clockwise rotation of the upper incisors causing their root apex to move more palatally makes remodeling changes in Point A in the form of its retraction roughly by one-third the amount of the backward movement of the upper incisors’ root apex.
Retraction of Point A in millimeters will roughly be equal to the reduction in SNA angle in degrees.
Acknowledgment
The authors would like to extend their heartfelt acknowledgment to the following contributors for their unparalleled support in this article: Dr. Puja C. Yavagal, Professor, Department of Public Health Dentistry, Bapuji Dental College and Hospital, Davangere, Karnataka, India. Dr. Arun Kumar, Consultant Biostatistician, Bapuji Dental College and Hospital, Davangere, Karnataka, India. Dr. Nikunj Maniyar, Postgraduate student, Department of Orthodontics and Dentofacial Orthopaedics, Bapuji Dental College and Hospital, Davangere, Karnataka, India.
Declaration of patient consent
Institutional Review Board (IRB) permission was obtained for the study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Does proclination of maxillary incisors really affect the sagittal position of point A? Angle Orthod. 2013;83:943-7.
- [CrossRef] [PubMed] [Google Scholar]
- Biomechanics and Esthetic Strategies in Clinical Orthodontics United Kingdom: Elsevier; 2004. p. :38-73.
- [Google Scholar]
- A cephalometric study of changes in point a under the influence of upper incisor inclination. J Nihon Univ Sch Dent. 1991;33:160-5.
- [CrossRef] [PubMed] [Google Scholar]
- Nonextraction treatment of severe Class II division 2 malocclusion: Part 1. Am J Orthod Dentofacial Orthop. 1990;97:510-21.
- [CrossRef] [Google Scholar]
- Diagnosis and treatment of Class II division 2 malocclusion. Angle Orthod. 1982;52:38-60.
- [Google Scholar]
- Maxillary incisor proclination effect on the position of point A in Class II division 2 malocclusion. Angle Orthod. 2009;79:880-4.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment and post-treatment craniofacial changes after rapid maxillary expansion and facemask therapy. Am J Orthod Dentofacial Orthop. 2000;118:404-13.
- [Google Scholar]
- Skeletal maturation evaluation using cervical vertebrae. Am J Orthod Dentofacial Orthop. 1995;107:58-66.
- [CrossRef] [Google Scholar]




