

Translate this page into:
Long-term stability of early anterior open bite treatment by magnetic and spring-loaded bite blocks

*Corresponding author: Dr. Umal H Doshi, Uphar, 68, Builders Society, Near Nandanvan colony, Aurangabad, Maharashtra, India. umal_16@rediffmail.com
-
Received: ,
Accepted: ,
Abstract
Introduction
The purpose of the present study was to evaluate the long-term stability of open bite correction with spring-loaded and magnetic bite blocks.
Materials and Methods
A total of 14 patients out of the original sample of 20 were evaluated clinically and cephalometrically at post-treatment, post-retention, and 4.2 years after retention. Of 14 patients, eight were from spring-loaded bite block group, while remaining six were from magnetic bite block group. Normality of data was checked with Shapiro–Wilk test and one-way repeated measures analysis of variance was used to compare the values at different time intervals. Pearson correlation analysis was used to examine the correlations between various cephalometric variables.
Results
Clinically, decrease in overjet and increase in overbite were evident in 12 patients, while two patients showed non- significant decrease in overbite. Skeletal changes in the form of the closure of mandibular plane angle, clockwise rotation of palatal plane, and significant increase in posterior face height were seen. Molar intrusion relapsed in the follow-up period but was compensated by the incisor extrusion. Overall, the success rate of 85.8% was seen.
Conclusion
Stability of early treatment with active bite blocks is comparable to any other treatment modality for correction of mild-to-moderate skeletal open bite cases. Importance of retention using the passive bite blocks needs further evaluation.
Keywords
Stability
Open bite
Bite blocks

INTRODUCTION
Open bite has long been most difficult type of malocclusion to treat and retain. The cause of this difficulty lies in its multifactorial etiology, which could be combination of skeletal, dental, functional, and habitual factors. This also explains why there is a range of treatment modalities including the growth guidance, elimination of potential etiologic factors, posterior teeth intrusion, anterior teeth extrusion, surgery, or combination of the above. Open bite with no underlying skeletal dysplasia is easy to treat and supposed to be self-correcting in many instances.[1,2] However, cases with abnormal vertical growth require special attention and as the patterns of facial growth get established at very early age, to improve the possibilities of success and stability, early treatment modalities such as functional appliances, multibracket techniques, headgears, and bite blocks have been suggested.[2-14]
Out of these early treatment modalities, posterior bite blocks have been shown to be effective in producing condylar growth and forward rotation of the mandible. Bite blocks could be passive or made active by addition of active elements such as springs or magnets.[11-14] A study comparing the effects of spring-loaded bite blocks and magnetic bite blocks had been carried out by Doshi and Bhad.[14] With both approaches, correction was achieved in patients with the age range of 8–13 years and it was mainly due to enhanced condylar growth and intrusion of buccal segment with increased muscle activity. In a recent systematic review by Greenlee et al.,[15] it was concluded that with any approach relapse tends to occur with success rate of around 75%. They found non-significant chance of increased relapse in growing individuals due to unfavorable growth pattern mainly in the form of insufficient vertical condylar growth and weak musculature. Since spring-loaded and magnetic bite blocks had positive effects with respect to condylar growth and muscle activity, stability of results could be expected. However, there are no studies on long-term stability with these approaches and for this reason, we evaluated the 5-year post-treatment stability of anterior open bite in growing individuals treated with spring-loaded and magnetic bite blocks.
MATERIALS AND METHODS
Before selecting the participants for the study, the research topic was approved by the ethical committee under university of health sciences. Sample size calculation was based on an alpha significance level of 5% (0.05) and a beta of 20% (0.20) to achieve 80% power test to detect a mean difference of 0.6 mm with standard deviation of 0.9 for maxillary molar intrusion.[16] Thus, sample size calculation revealed the need for 10 individuals in each group. Based on this, 20 skeletal open bite patients (8 males and 12 females) with the age range of 8–13 years were selected. Each met the following criteria: (1) Anterior open bite on clinical inspection (incisor overbite: <−1.0 mm), (2) cephalometrically confirmed steep mandibular plane (high SN-MP angle >400), increased gonial angle (>137°), (3) Class I or II occlusion, (4) no finger-sucking habits, and (5) no evidence of enlarged tonsils or adenoids.
Informed consent forms were signed by parents of all participants. All the patients were randomly divided into two treatment groups. The first group (five males and five females) with average open bite of –3.2 mm was treated with the spring-loaded bite blocks, while the second group (three males and seven females) with average open bite of −3.5 was treated with the magnetic bite blocks. Spring-loaded bite block appliance [Figure 1] consisted of a mandibular plate with occlusal coverage and two posterior bite blocks connected to each other by two 0.9-mm springs on each side. The hooks in the bite blocks served to gauge the compression force. The springs were activated after 4 weeks to supply intrusive fore of 250 cN per side. Magnetic bite block appliance [Figure 2] consisted of two maxillary blocks and two mandibular blocks connected by 1 mm steel bar. Each block had one neodymium boron circular magnet (1.5 mm × 10.0 mm). On each side, maxillary and mandibular magnets were in repelling mode, thus producing intrusive force of about 300 cN per side. Patients were instructed to wear the appliance full time except during meals and brushing. After 8 months of treatment, successful closure of open bite was obtained with both the appliances. Spring-loaded bite blocks produced average closure by 3.3 mm, while magnetic blocks closed the bite by 4.9 mm. Passive bite blocks were given to all patients as a retainer to be worn full time except meals and brushing for further 10 months.[14] After this period, none of the patients received any orthodontic treatment. Of the original sample of 20 patients (mean age, 10 years 1 month), it was possible to obtain long-term follow-up records for 14 (n = 14, six males and eight females) at a mean age of 15 years 2 months. Of 14 patients, eight (three males and five females) were from spring-loaded bite block group, while remaining six (three males and three females) were from magnetic bite block group.

- Spring-loaded bite blocks.
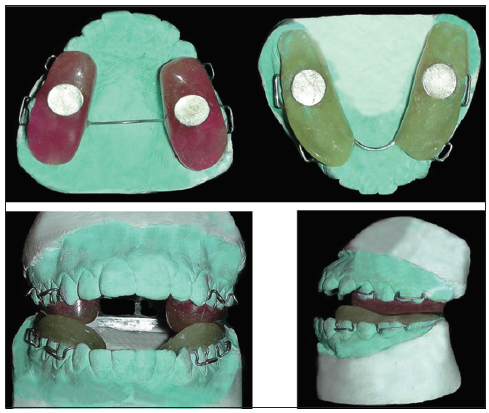
- Magnetic bite blocks.
Lateral cephalograms were obtained before starting the treatment (T1; mean age 10 years 1 month), after 8 months of active treatment (T2; mean age 10 years 9 months), post-retention (T3; mean age 11 years 8 months), and again at the post-retention follow-up stage (T4; 15 years 2 months). For all cephalograms, a single machine (PM 2002, Planmeca) was used. Every lateral cephalogram was traced by one of the authors (U.H.D.) on lead acetate paper, and 18 linear and 16 angular parameters were measured by both authors [Figure 3]. These were digitized with a Numonics AccuGrid XNT, model A30TLF digitizer (Numonics, Montgomeryville, Pa). These data were stored and analyzed with Dentofacial Planner 7.0 (Dentofacial Planner Software, Toronto, Ontario, Canada), which corrected the image magnification factors of the groups.

- Cephalometric measurements.
Method error
All tracings and measurements were repeated by the two operators at 2-week intervals. The method error was calculated. The mean difference was within 0.2 mm for linear and 0.5° for angular measurements and was insignificant.
Statistics
Since the aim of the present study was to evaluate the long- term post-treatment changes, the comparisons for all clinical and cephalometric parameters were done at T2, T3, and T4. Comparison at T1 and T2 has already been done in previous publication.[14] For all clinical and cephalometric parameters, the mean differences, standard deviations, and standard errors were calculated. The Shapiro–Wilk test was used to check whether the continuous variables were normally distributed. Then, one- way repeated measures analysis of variance was used to evaluate the effects of treatment at T2, T3, and T4. Tukey’s post hoc tests were performed to determine whether differences between times were statistically significant. Post-treatment changes between the groups were evaluated using unpaired t-test. Significance was determined at 0.05 level of confidence.
RESULTS
There were no significant differences for all parameters between two groups at T1. Successful closure of open bite was seen with both the treatment approaches at 8 months (T2) [Table 1].
| Measurements | Spring-loaded bite block | Magnetic bite block | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T2-T1 (mean±SD) |
T3-T1 (mean±SD) |
T4-T1 (mean±SD) |
T2-T3 P value |
T3-T4 P value |
T2-T4 P value |
T2-T1 (mean±SD) |
T3-T1 (mean±SD) |
T4-T1 (mean±SD) |
T2-T3 P value |
T3-T4 P value |
T2-T4 P value |
|
| Overjet | −0.7±0.2 | −0.8±0.4 | −0.9±0.1 | 0.049* | 0.1 | 0.00* | −1.6±0.5 | −1.7±0.3 | −1.9±0.1 | 0.22 | 0.01* | 0.00* |
| Overbite | 3.5±1.3 | 3.7±1.2 | 3.9±1.4 | 0.063 | 0.005* | 0.005* | 4.8±1.5 | 4.9±1.2 | 4.9±1.4 | 0.08 | 1 | 0.15 |
T2 -After treatment, T3 -Post-retention, T4-4.2 years after retention, negative values represent decrease during treatment; positive values represent increase during treatment. *Statistically significant
Clinical changes
Slight decrease in overjet and increase in overbite were seen after 10 months of retention (T3) in both the groups [Table 1]. At post- retention follow-up stage (T4), further decrease in overjet and increase in overbite were noted in 12 patients. In two patients, there were slight increase in overjet and slight decrease in overbite. Between groups comparison [Table 2] showed significant (P < 0.5) difference in decrease in overjet, with magnetic group showing more decrease than spring-loaded group. Overbite comparison showed highly significant (P < 0.05) increase in spring-loaded group when compared with magnetic bite block group.
| Measurements | Spring-loaded bite block (mean change±SD) | Magnetic bite block (mean change±SD) | P value |
|---|---|---|---|
| Overjet | −0.2±0.1 | −0.3±0.4 | 0.024* |
| Overbite | 0.4±0.1 | 0.1±0.1 | 0.000* |
T2 - After treatment, T4-4.2 years after retention, negative values represent decrease during treatment; positive values represent increase during treatment. *Statistically significant
Cephalometric evaluation
Results for 24 cephalometric variables are shown in Tables 3-5.
| Measurements | T2 (mean±SD) | T3 (mean±SD) | T4 (mean±SD) | T2-T3 P value | T3-T4 P value | T2-T4 P value |
|---|---|---|---|---|---|---|
| Anteroposterior skeletal angular measurements | ||||||
| SNA (°) | 79.4±2.1 | 79.3±2.6 | 80.3±2.8 | 0.170 | 0.013* | 0.020* |
| SNB (°) | 77.4±1.5 | 77.7±2.4 | 78.8±1.7 | 0.594 | 0.002* | 0.000* |
| ANB (°) | 2±1.5 | 1.6±0.2 | 1.5±1.1 | 0.015* | 0.646 | 0.048* |
| Vertical skeletal angular measurements | ||||||
| SN-GoGn (°) | 35.1±3.5 | 34.2±3.2 | 33.5±2.1 | 0.000* | 0.000* | 0.000* |
| Ar-Go-Me (°) | 131±2.2 | 129.1±2.3 | 129.2±1.8 | 0.000* | 0.380 | 0.000* |
| Ar-Go-N (°) | 53.4±2.1 | 53.2±1.4 | 53.4±1.5 | 0.170 | 0.121 | 1 |
| N-Go-Me (°) | 74.2±1.2 | 74±1.4 | 73.5±1.1 | 0.009 | 0.000* | 0.000* |
| S-Gn/FH (°) | 64.4±1.9 | 63.8±2.7 | 62.9±1.5 | 0.000* | 0.000* | 0.000* |
| SN/ANS-PNS (°) | 7.8±2.6 | 8.4±2.8 | 8.9±1.1 | 0.000* | 0.000* | 0.000* |
| SN/OP (°) | 16.3±1.5 | 16.1±1.3 | 15.9±0.8 | 0.037* | 0.045* | 0.007* |
| FMA (°) | 29.3±1.8 | 28.8±1.8 | 27.5±0.9 | 0.000* | 0.000* | 0.000* |
| Skeletal linear measurements | ||||||
| S-Go (mm) | 71.7±2.1 | 72.8±1.7 | 78.7±1.2 | 0.000* | 0.000* | 0.000* |
| LAFH (mm) | 70.1±1.4 | 69.7±1.6 | 69.8±1.3 | 0.000* | 0.121 | 0.005* |
| Ar-Go (mm) | 40.3±1.4 | 42±0.5 | 46.3±1.2 | 0.000* | 0.000* | 0.000* |
| Dentoalveolar measurements | ||||||
| U1-NA (°) | 22.1±1.5 | 22±1.1 | 22.7±0.9 | 0.085 | 0.001* | 0.010* |
| L1-NB (°) | 23.7±1.3 | 23.8±1.7 | 24.5±1.2 | 0.018 | 0.000* | 0.000* |
| UI-NA (mm) | 3.6±1.7 | 3.4±1.5 | 3.9±1.7 | 0.003 | 0.000* | 0.005* |
| L1-NB (mm) | 3.8±0.7 | 3.9±1 | 3.9±1.2 | 0.033* | 1 | 0.067 |
| U1-PP (mm) | 29.8±2.1 | 30.3±1.2 | 30.7±1.4 | 0.010* | 0.003* | 0.000* |
| L1-GoMe (mm) | 41.3±1.6 | 42.3±1.3 | 43.1±0.7 | 0.000* | 0.000* | 0.000* |
| U6-PP (mm) | 24.1±0.5 | 23.7±0.9 | 24.3±0.8 | 0.000* | 0.000* | 0.012* |
| L6-GoMe (mm) | 32.1±1.7 | 31.8±0.9 | 32.5±1.1 | 0.002* | 0.000* | 0.010* |
| Overjet (mm) | 2.2±0.8 | 2±1.1 | 1.9±0.6 | 0.012* | 0.007* | 0.002* |
| Overbite (mm) | 2.2±1.2 | 2.4±0.7 | 2.6±0.9 | 0.007* | 0.001* | 0.000* |
T2 - After treatment, T3 - Post-retention, T4-4.2 years after retention, *statistically significant
| Measurements | T2 (mean±SD) | T3 (mean±SD) | T4 (mean±SD) | T2-T3 P value | T3-T4 P value | T2-T4 P value |
|---|---|---|---|---|---|---|
| Anteroposterior skeletal angular measurements | ||||||
| SNA (°) | 79.6±1.4 | 79.6±2.4 | 80.8±2.1 | 1 | 0.004* | 0.004* |
| SNB (°) | 77.6±1.7 | 78.9±1.5 | 79.1±1.3 | 0.000* | 0.002* | 0.000* |
| ANB (°) | 2±0.3 | 0.7±0.9 | 1.7±0.8 | 0.000* | 0.054* | 0.487 |
| Vertical skeletal angular measurements | ||||||
| SN-GoGn (°) | 34.1±1.5 | 33.4±2.6 | 32.3±1.3 | 0.000* | 0.000* | 0.000* |
| Ar-Go-Me (°) | 132±2.1 | 131.3±1.6 | 130.1±1.7 | 0.000* | 0.000* | 0.000* |
| Ar-Go-N (°) | 52.6±2.2 | 52.3±1.5 | 52.6±2.1 | 0.063 | 0.020* | 1 |
| N-Go-Me (°) | 75.1±2.4 | 74.3±1.1 | 74.3±1.4 | 0.002* | 1 | 0.003* |
| S-Gn/FH (°) | 65.2±1.4 | 64.3±1.9 | 63.4±1.2 | 0.000* | 0.000* | 0.000* |
| SN/ANS-PNS (°) | 7.4±1.8 | 8.5±2.3 | 8.8±0.9 | 0.000* | 0.002* | 0.000* |
| SN/OP (°) | 16.7±2.4 | 16.6±1.3 | 16.4±1.4 | 0.011* | 0.032* | 0.017* |
| FMA (°) | 29.8±2.1 | 28.6±1.5 | 27.8±1.6 | 0.000* | 0.000* | 0.000* |
| Skeletal linear measurements | ||||||
| S-Go (mm) | 71.1±1.6 | 72.9±1.2 | 77.8±0.8 | 0.000* | 0.000* | 0.000* |
| LAFH (mm) | 71.8±2.1 | 71.6±1.1 | 71.7±1.2 | 0.032* | 0.011* | 0.174 |
| Ar-Go (mm) | 40.2±1.7 | 41.9±0.9 | 45.8±1.5 | 0.016* | 0.000* | 0.000* |
| Dentoalveolar measurements | ||||||
| U1-NA (°) | 21.9±2.1 | 21.6±1.7 | 22.7±1.6 | 0.011* | 0.000* | 0.005* |
| L1-NB (°) | 24.8±1.2 | 25.1±1.3 | 25.4±1.1 | 0.000* | 0.009* | 0.001* |
| UI-NA (mm) | 3.6±1.4 | 3.5±1.6 | 3.8±2.3 | 0.040* | 0.009* | 0.110 |
| L1-NB (mm) | 3.9±0.9 | 4±1.5 | 4.1±1.4 | 0.075 | 0.011* | 0.006* |
| U1-PP (mm) | 28.8±2.1 | 29.8±1.6 | 30.3±1.6 | 0.000* | 0.000* | 0.000* |
| L1-GoMe (mm) | 40.9±0.8 | 41.8±2.1 | 42.1±0.9 | 0.001* | 0.000* | 0.000* |
| U6-PP (mm) | 23.2±1.1 | 22.9±0.9 | 23.6±1.5 | 0.007* | 0.000* | 0.004* |
| L6-GoMe (mm) | 31.8±0.9 | 31.5±1.1 | 32.1±1.3 | 0.003* | 0.000* | 0.014* |
| Overjet (mm) | 2.1±0.9 | 2±1.3 | 1.8±0.7 | 0.040* | 0.002* | 0.000* |
| Overbite (mm) | 1.9±0.6 | 2±0.9 | 2±0.8 | 0.011* | 1 | 0.011* |
T2 - After treatment, T3 - Post-retention, T4-4.2 years after retention, *Statistically significant
| Measurements | Spring-loaded bite block (mean change±SD) | Magnetic bite block (mean change±SD) | P value |
|---|---|---|---|
| Anteroposterior skeletal angular measurements | |||
| SNA (°) | 0.9±0.7 | 1.2±0.7 | 0.010* |
| SNB (°) | 1.4±0.2 | 1.5±0.4 | 0.233 |
| ANB (°) | −0.5±0.4 | −0.3±0.5 | 0.000* |
| Vertical skeletal angular measurements | |||
| SN-GoGn (°) | −1.6±1.4 | −1.8±0.2 | 0.418 |
| Ar-Go-Me (°) | −1.8±0.4 | −1.9±0.4 | 0.798 |
| Ar-Go-N (°) | 0±0.6 | 0 ± 0.1 | 1 |
| N-Go-Me (°) | −0.7±0.1 | −0.8±1 | 0.142 |
| S-Gn/FH (°) | −1.5±0.4 | −1.8±0.2 | 0.023* |
| SN/ANS-PNS (°) | 1.1±1.5 | 1.4±0.9 | 0.001* |
| SN/OP (°) | −0.4±0.7 | −0.3±1 | 0.211 |
| FMA (°) | −1.8±0.9 | −2±0.5 | 0.070 |
| Skeletal linear measurements | |||
| S-Go (mm) | 7±0.9 | 6.7±0.8 | 0.074 |
| LAFH (mm) | −0.3±0.1 | −0.1±0.9 | 0.000* |
| Ar-Go (mm) | 6±0.2 | 5.6±0.2 | 0.701 |
| Dentoalveolar measurements | |||
| U1-NA (°) | 0.6±0.6 | 0.8±0.5 | 0.000* |
| L1-NB (°) | 0.8±0.1 | 0.6±0.1 | 0.000* |
| UI-NA (mm) | 0.3±0 | 0.2±0.9 | 0.001* |
| L1-NB (mm) | 0.1±0.5 | 0.2±0.5 | 0.008* |
| U1-PP (mm) | 0.9±0.9 | 1.5±0.5 | 0.002* |
| L1-GoMe (mm) | 1.8±0.9 | 1.2±0.1 | 0.000* |
| U6-PP (mm) | 0.2±0.3 | 0.4±0.4 | 0.000* |
| L6-GoMe (mm) | 0.4±0.6 | 0.3±0.4 | 0.009* |
| Overjet (mm) | −0.3±0.2 | −0.3±0.2 | 0.832 |
| Overbite (mm) | 0.4±0.3 | 0.1±0.2 | 0.000* |
T2 - After treatment, T4-4.2 years after retention, negative values represent decrease during treatment; positive values represent increase during treatment. *Statistically significant
Anteroposterior changes
For both groups, anterior-posterior skeletal changes showed improvement [Tables 3 and 4]. At 5-year follow-up period (T4), ANB angle decreased to 1.5° for the spring-loaded group (P < 0.05) from post-treatment value of 2°, but for the magnetic bite block group, there was non-significant decrease to 1.7° from post-treatment value of 2° [Table 5].
Vertical changes
For vertical measurements, further closure of mandibular plane angle (MPA) (SN-GoGn) by 1.6° (P < 0.05) and 1.8° (P < 0.05) was noted for spring loaded and magnetic group, respectively. Significant clockwise rotation of palatal plane (SN/ANS-PNS) by 1.1° and 1.4° was noted for spring loaded and magnetic group, respectively [Table 5].
From post-treatment to 5-year follow-up, vertical linear measurements showed a significant increase in the posterior face height (S-Go) of 7 mm and 6.7 mm in spring-loaded and magnetic block groups, respectively. In the spring-loaded group, ramus height (Ar-Go) increased by 6 mm, while in the magnetic group, it increased by 5.6 mm [Table 5].
Dentoalveolar changes
In the post-retention period, there was increase in incisor angulations for both groups [Tables 3 and 4]. Dental heights were increased for both groups [Tables 3 and 4]. Magnetic group showed significantly (P < 0.05) more extrusion of maxillary incisors (1.5 mm) and molars (0.4 mm) as compared to spring-loaded group. Spring-loaded group showed significantly (P < 0.05) more extrusion of mandibular incisors (1.8 mm) and molars (0.4 mm) as compared to magnetic group [Table 5].
Overjet further decreased in both groups (0.3 mm). Overbite increased significantly (P < 0.05) more in the spring-loaded group (0.4 mm) as compared to the magnetic group (0.1 mm) [Table 5].
While analyzing the correlations between cephalometric variables [Table 6] for both groups, overbite correction was mainly due to the closure of MPA (SN-GoGn). For rest of parameters, no significant correlations were found.
| Variable 1 | Variable 2 | Spring-loaded bite block | Magnetic bite block | ||||
|---|---|---|---|---|---|---|---|
| R | P | Sig (two-tailed) | R | P | Sig (two-tailed) | ||
| U6-PP | FMA | 0.253 | 0.5841 | NS | −0.544 | 0.0658 | NS |
| U6-PP | OB | −0.353 | 0.4380 | NS | 0.316 | 0.6042 | NS |
| L6-GoMe | FMA | 0.016 | 0.9730 | NS | −0.101 | 0.8715 | NS |
| L6-GoMe | OB | 0.143 | 0.7596 | NS | −0.316 | 0.6042 | NS |
| U1-PP | OB | −0.218 | 0.6390 | NS | 0.109 | 0.8614 | NS |
| L1-GoMe | OB | 0.049 | 0.9167 | NS | 0.257 | 0.6761 | NS |
| OB | SN-GoGn | −0.752 | 0.05 | * | −0.910 | 0.0319 | * |
| OB | SNB | −0.413 | 0.3577 | NS | 0.866 | 0.0577 | NS |
| SNB | SN-GoGn | −0.280 | 0.5433 | NS | −0.586 | 0.2990 | NS |
| OB | SN/ANS-PNS | 0.583 | 0.1698 | NS | −0.770 | 0.1279 | NS |
T2 - After treatment; T4 - Post-retention; R - Pearson correlation coefficient; P -P value; * - Significant; NS - Not significant. *P<0.05
DISCUSSION
The present study evaluated the long-term stability of open bite patients treated with spring-loaded and magnetic bite blocks, based on clinical and cephalometric changes. To evaluate the stability, post-treatment changes were compared with the post-retention and 4.2-year follow-up changes. These changes were calculated in 14 patients of the original sample of 20. Of 14 patients, eight (three males and five females) were from the spring-loaded bite block group, while remaining six (three males and three females) were from the magnetic bite block group.
Clinical changes
Based on clinical examination, there were decrease in overjet and increase in overbite through post-treatment period to 5-year follow-up stage for both the groups. However, increase in overbite was significantly more in patients treated with spring-loaded bite blocks. To explore the reasons behind these changes, cephalometric variables were compared.
Anteroposterior changes
As noted in the earlier publication,[14] both the appliances were effective in increasing mandibular prognathism and holding of maxillary forward growth. These effects were continued during 10 months of retention with passive bite blocks. However, after retention phase, continued mandibular as well as maxillary forward growth was noted. In fact, highly significant (P < 0.05) maxillary growth of 1.2° and 0.9° was observed in magnetic and spring-loaded group, respectively. This could be explained by release of pressure during post-retention phase on maxilla induced by increased lip pressures generated by the patients in an attempt to keep their lips sealed. Another reason for such favorable anteroposterior growth could be attributed to contribution from natural forward growth since all the patients were in growth phase.
Vertical changes
In the vertical direction, favorable changes in the form of the closure of MPA (Sn GoGn) and clockwise rotation of palatal plane (SN-ANS-PNS) were noted. In a longitudinal study, Karlsen[17] has noted that boys with high angles display significantly less closure of MPA than low angle boys, with the difference being most pronounced during childhood. Moreover, as shown by Garcia- Morales and Buschang[18] in untreated open bite cases with high angle, between ages 10 and 15 years, there is very little change in MPA. In our sample during same period, MPA decreased by 1.6° and 1.8° in spring-loaded and magnetic bite block groups, respectively. The palatal plane rotated in clockwise fashion by 1.1° and 1.4° in spring-loaded and magnetics group, respectively. This effect is similar to changes in the position of ANS and PNS seen by Majourau and Nanda[19] for a case treated with a high-pull chincup with posterior bite block as expander appliance.
In hyperdivergent patients for improvement in skeletal pattern, along with the inhibition of growth of anterior facial height, augmenting posterior facial height is an equally important goal.[20,21] In both the groups, in post-treatment period, there was slight decrease of 0.3 and 0.2 mm in LAFH for spring-loaded and magnetic block group, respectively. This is significant since during similar period of transition from mixed dentition to permanent dentition, Karlsen[22] had reported increase in LAFH by around 5 mm. In the post-treatment period, there was increase in posterior face height (S-Go) and ramus height (Ar-Go). Major contribution for increase in the posterior facial height of 7 mm and 6.7 mm came mainly from increase in ramus height (6 mm and 5.6 mm). This is in agreement with Karlsen’s study[22] in which posterior face height increased by 7 mm and ramus height increased by 5.5 m.
Dentoalveolar changes
In both the groups, the incisor proclination increased over a period of 5 years. This is, in contrast, to decrease in incisor angulation observed at the end of the treatment period. This could be due to the release of increased lip pressures generated by the children in the attempt to keep their lips sealed during the treatment period.
In the post-retention period, when compared with the post- treatment position, the maxillary molars extruded by 0.2 mm and 0.4 mm, while mandibular molars extruded by 0.4 mm and 0.3 mm for spring-loaded and magnetic block group, respectively. Similar relapse has also been observed by Baek et al.[23] in open bite patients treated with implants, evaluated after 3 years of retention. In the present study, results have been evaluated after 4.2 years without retention. As observed by Baek et al.,[23] most of the relapse in molar intrusion occurs in the 1st year after treatment and use of passive blocks during this period could have been the most important factor in preventing such changes in the present study. The relapse in molar intrusion was compensated by significant (P < 0.05) extrusion of maxillary and mandibular incisors. Maxillary incisors extruded by 0.9 and 1.5 mm while mandibular incisors extruded by 1.8 and 1.2 mm for spring-loaded and magnetic block group, respectively. Such changes are in agreement with studies by Baek et al.[23] and Sugawara et al.[24]
In the post-treatment period, there was further decrease in overjet by 0.3 mm, which is mainly due to favorable maxillary and mandibular growth as well as closure of MPA. In both the groups, further deepening of the bite was observed (0.4 and 0.1 mm), despite slight relapse of molar intrusion. Main contribution for this was from incisor extrusion and favorable skeletal changes such as closure of MPA, clockwise rotation of palatal plane, inhibition of growth of LAFH, and augmentation of the growth of posterior face height.
In analyzing the correlations between cephalometric variables from post-treatment period to follow-up period, we verified that overbite correction was mainly attained by the closure of MPA. However, no significant correlation was found for rest of the parameters. This may suggest that stability of open bite correction was mainly attained by favorable changes in skeletal growth, especially in condylar region, while changes in molar and incisor regions supplemented the final outcome. Thus, closure of the MPA can be taken as predictor of success and stability of both appliances. However, in view of small sample size, this assumption needs further evaluation with larger sample.
In assessing the success rate of spring-loaded and magnetic bite blocks, we observed absolute stable results in 85.8% and clinically non-significant relapse in 14.2% of cases. This is in agreement with Baek et al.[23] who observed success rate of 83% in open bite patients treated with molar intrusion using implants. When stability of both groups was compared, none was superior to other. This may indicate that the effect of bite block may be more important than the effect of active elements such as springs and magnets.
Although it was not the purpose of the study to evaluate the changes using passive block as a retainer, its effects could had been the most important factor in achieving long-term stability. Subsequent studies might further elaborate on this point by analyzing the relapse patterns in patients treated with retainer having vertical control and no vertical control such as Hawley retainer.
One of the shortcomings of the present study was lack of control group. Due to ethical reasons and issues involving unwanted radiation exposure, it was not possible to have control group. Second, loss of six subjects from original sample size of 20 was another limiting factor. Future prospective studies with larger sample size and matched controls with specific retention protocol are expected to overcome both these shortcomings and further support the results of the present study.
CONCLUSION
The following conclusions can be drawn:
Clinically, 5 years after treatment with no retention for a period of 4.2 years, slight decrease in overjet and increase in overbite were seen in 12 patients. In two patients, non-significant decrease in overbite was seen.
Skeletally, closure of MPA, clockwise rotation of palatal plane, inhibition of growth of LAFH, and augmentation of growth of posterior face height were seen.
Relapse in molar intrusion with significant incisor extrusion was seen in both groups.
Success rate of 85.8% was seen. This was thought to be mainly due to the use of passive blocks as retainers in critical 1st year following completion of treatment.
Stability for both groups was remarkably similar, suggesting the effect of bite block may be more important than the addition of active elements such as springs and magnets.
Declaration of patient consent
Patient's consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- A biological approach to diagnosis, mechanics and treatment of vertical dysplasia. Angle Orthod. 1980;50:279-300.
- [PubMed] [Google Scholar]
- Vertical growth versus anteroposterior growth as related to function and treatment. Angle Orthod. 1964;34:75-93.
- [Google Scholar]
- Changes in facial dimensions associated with the use of forces to retract the maxilla. Am J Orthod. 1981;80:17-30.
- [CrossRef] [Google Scholar]
- Maxillary traction splint: A cephalometric evaluation. Am J Orthod. 1984;85:376-84.
- [CrossRef] [Google Scholar]
- Vertical control in treatment of patients having backward-rotational growth tendencies. Angle Orthod. 1978;48:132-40.
- [Google Scholar]
- Effects of vertical chincap therapy on the mandibular morphology in open-bite patients. Am J Orthod Dentofacial Orthop. 2002;122:506-11.
- [CrossRef] [PubMed] [Google Scholar]
- A functional approach to treatment of skeletal open bite. Am J Orthod. 1983;84:54-68.
- [CrossRef] [Google Scholar]
- Elastic activator for treatment of open bite. Br J Orthod. 1999;26:89-92.
- [CrossRef] [Google Scholar]
- Early orthodontic treatment of skeletal open-bite malocclusion with the open-bite bionator: A cephalometric study. Am J Orthod Dentofacial Orthop. 2007;132:595-8.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of 2 early treatment protocols for open-bite malocclusions. Am J Orthod Dentofacial Orthop. 2007;132:743-7.
- [CrossRef] [PubMed] [Google Scholar]
- A clinical assessment of the active vertical corrector-a nonsurgical alternative for skeletal open bite treatment. Am J Orthod. 1986;89:428-36.
- [CrossRef] [Google Scholar]
- Progressive increase in lower anterior facial height and the use of posterior bite block in its management. In: , ed. Orthodontics: State of Art, Essence of Science. St. Louis: C V Mosby; 1986. p. :200-21.
- [Google Scholar]
- Intrusion of posterior teeth with magnets: An experiment in nongrowing baboons. Am J Orthod Dentofacial Orthop. 1991;100:393-400.
- [CrossRef] [Google Scholar]
- Early management of skeletal open bite with spring-loaded and magnetic bite blocks. World J Orthod. 2010;11:107-16.
- [PubMed] [Google Scholar]
- Stability of treatment for anterior open-bite malocclusion: A meta-analysis. Am J Orthod Dentofacial Orthop. 2011;139:154-69.
- [CrossRef] [PubMed] [Google Scholar]
- A cephalometric evaluation of anterior openbite correction with the magnetic active vertical corrector. Angle Orthod. 1991;61:93-102.
- [PubMed] [Google Scholar]
- Craniofacial growth differences between low and high MP-SN angle males: A longitudinal study. Angle Orthod. 1995;65:341-50.
- [PubMed] [Google Scholar]
- Biomechanical basis of vertical dimension control during rapid palatal expansion therapy. Am J Orthod Dentofacial Orthop. 1994;106:322-8.
- [CrossRef] [Google Scholar]
- Anterior open-bite: A cephalometric analysis and suggested treatment procedures. Am J Orthod. 1975;67:523-21.
- [CrossRef] [Google Scholar]
- Normal and abnormal growth of the mandible. A synthesis of longitudinal cephalometric implant studies over a period of 25 years. Eur J Orthod. 1983;5:1-46.
- [CrossRef] [PubMed] [Google Scholar]
- Association between facial height development and mandibular growth rotation in low and high MP-SN angle faces: A longitudinal study. Angle Orthod. 1997;67:103-10.
- [PubMed] [Google Scholar]
- Long-term stability of anterior open-bite treatment by intrusion of maxillary posterior teeth. Am J Orthod Dentofacial Orthop. 2010;138(396):e1-9.
- [Google Scholar]
- Treatment and posttreatment dentoalveolar changes following intrusion of mandibular molars with application of a skeletal anchorage system (SAS) for open bite correction. Int J Adult Orthodon Orthognath Surg. 2002;17:243-53.
- [PubMed] [Google Scholar]




