

Translate this page into:
Occlusal status among Yemeni children
Address for Correspondence: Dr. Nabil M. Al-Zubair, P.O. Box 85, Sana’a, Yemen. E-mail: dr.nabilzubair7@gmail.com
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Objectives
The purpose of this study was to assess the occlusal status in schoolchildren in Yemen, and to compare the results with those of other studies.
Materials and Methods
The sample for this epidemiological survey consisted of 3003 primary school students, half of whom were boys and the other half girls, aged 12 years. The subjects were randomly selected, and none had received previous orthodontic treatment. Variables examined included intra-arch irregularities and malalignment (crowding and spacing in the incisal segments of the arch and midline diastema) and discrepancies in occlusal contact relationship (maxillary overjet, mandibular overjet, anterior openbite and antero-posterior molar relation).
Results
The results showed that about 26.1% of the subjects were still in the late mixed dentition stage and 73.9% presented with a dentition in the early permanent stage. Normal overjet was found in 55% of the sample. Crowding was observed in 31.4% of the subjects and midline diastema in 14.2%.
Conclusion
Occlusal status among Yemeni children was characterized by a relatively high frequency of dental crowding, as well as a relatively high frequency of anterior mandibular overjet (Class III malocclusions).
Keywords
Malocclusion
occlusal status
Yemen

INTRODUCTION
The practice and teaching of orthodontics at Yemen is still relatively young. A systematic and well-organized dental care program for any target population in a community requires some basic information, such as the prevalence of the condition. In the more developed parts of the world, where the specialty of orthodontics has been established, adequate basic information is available.[1-8] In the developing countries, such information can be lacking. Despite efforts in the Arab world in the past decades to make health systems more equitable, access to dental health care is still far from adequate, especially in poor communities.[9-23]
Yemen is a country on the Arabian Peninsula in Southwest Asia and is part of the Middle East. However, no recent data on the prevalence, distribution and severity of malocclusion or the orthodontic treatment need of the population representative of the whole of Yemen is available. The lack of data on the distribution, prevalence and severity of malocclusion in Yemen could be affecting the effective planning for the orthodontic services, which is needed to address the ever-increasing demand for orthodontic treatment.
MATERIALS AND METHODS
Subjects
The sample consisted of 3003, 12-year-old children attending schools in six governorates (cities and environs) in Yemen. In each governorate the same multi-stage stratified sampling technique was implemented. From each sector, 500 children were included in the survey, half of whom (250 children) were urban and the other half were rural.
Urban children were considered as those living in the center of each governorate taken as clusters of 25 students from 10 randomly selected schools. Rural children were selected from five small villages from each sector, two clusters of 25 students from each village.
This gives a total of 3000 examined children taken from 120 schools; half of whom were males (1500 students from 60 schools) and the other half were females 1500 students from 60 schools).
From each school, the first accessible 25 children were examined. Thirteen schools did not have 25 children 12-year of age so neighboring schools were visited to complete the required number making the total number of visited schools 133.
Permission was obtained from the general directorate of education in Yemen and the regional directorate of education in the governorates. All school authorities were contacted and the purpose of this study was explained to them to ensure full cooperation.
Methods
Examination area
The children examined were seated in a chair with a high backrest with their head supported in an upright position and the examiner standing in front of the chair.[24,25] Whenever possible the examination area was partitioned or arranged in such a way that children enter at one point and leave at another. The children were not permitted to crowd around the examiner. Daylight was used for illumination, and a portable light was used to supplement natural daylight during examination when needed. In the absence of electricity, the portable light was connected to a 12V battery.
Clinical examination
The intraoral examination included the objective registration of the occlusal features, which is divided into two parts according to WHO:32
-
Intra-arch irregularities and malalignment
Crowding in the incisal segments of the arch.
Spacing in the incisal segments of the arch.
Maxillary central diastema.
-
Discrepancies in occlusal contact relationship
Anterior maxillary overjet.
Anterior mandibular overjet (negative overjet).
Vertical anterior openbite.
Antero-posterior molar relation.
Statistical analysis
All statistical analyses were performed using SPSS 13.0, IBM Corporation, New York, NY. Pearson’s Chi-square test was used to test the differences between gender urbanization and dentition stage. Statistical significance was set at (P < 0.05).
RESULTS
The prevalence of dentition stage
Division of the sample in the late mixed dentition stage and early dentition stage indicated that 26.1% of the study population are still in the late mixed dentition stage and 73.9% presented with a dentition in the early permanent stage [Figure 1]. The results indicated that there are more 12-year-old girls presenting with a dentition in the early permanent stage than boys, 77.61% and 70.11%, respectively. The distribution of the number of males and females in the two stages of dental development was statistically significant different (P < 0.05).
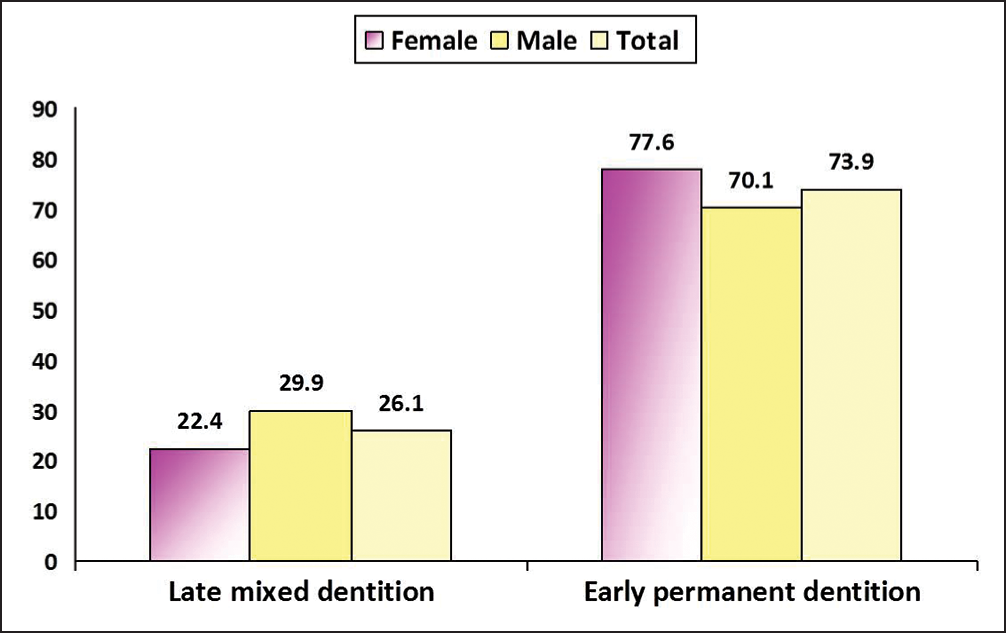
- Distribution of the sample according to gender and dentition stage
Intra-arch irregularities and malalignment
Table 1 depicts the distribution of intra-arch irregularities according to gender, residency and dentition stage. Of the whole sample, 31.4% presented with crowding either in one dental arch or both (maxillary and mandibular), whereas 24.3% presented with spacing either in one dental arch or both (maxillary and mandibular).
| Crowding in the incisal segments | No crowding n (%) | Crowding in one/two segment n (%) |
|---|---|---|
| Gender | ||
| Female n=1501 | 1045 (69.6) | 456 (30.4) |
| Male n=1502 | 1013 (67.4) | 489 (32.6) |
| Residency | ||
| Urban n=1502 | 971 (64.6)* | 531 (35.4)* |
| Rural n=1501 | 1087 (72.4)* | 414 (27.6)* |
| Dentition stage | ||
| Late mixed dentition n=785 | 544 (69.3) | 241 (30.7) |
| Early permanent dentition n=2218 | 1514 (68.3) | 704 (31.7) |
| Total | ||
| 3003 | 2058 (68.6) | 945 (31.4) |
| Spacing in the incisal segments | No spacing n (%) | Spacing in one/two segment n (%) |
|---|---|---|
| Gender | ||
| Female n=1501 | 1114 (74.2) | 387 (25.8) |
| Male n=1502 | 1159 (77.2) | 343 (22.8) |
| Residency | ||
| Urban n=1502 | 1165 (77.6) | 337 (22.4) |
| Rural n=1501 | 1108 (73.8) | 393 (26.2) |
| Dentition stage | ||
| Late mixed dentition n=785 | 590 (75.2) | 195 (24.8) |
| Early permanent dentition n=2218 | 1683 (75.9) | 535 (24.1) |
| Total | ||
| 3003 | 2273 (75.7) | 730 (24.3) |
*P < 0.05
Crowding was more prevalent in urban children than rural children, and the difference was considered as statistically significant (χ2 = 10.969, df = 1, P = 0.0004).
Maxillary midline diastema
Of the 3003 children examined, 426 or 14.2% presented with maxillary midline diastema of 1 mm or more. If spaces >2 mm are taken into account, 1.8% of the children presented with diastema. Considering gender differences, diastema was found to be almost equally distributed between males and females. If diastema larger than 2 mm is taken into account, about twice as many females (2.6%) than males (1.3%) presented with diastema, the difference between gender was statistically significant (P < 0.05), there are more girls than boys with a midline diastema larger than 2 mm. The results for the interaction of dentition stage and midline diastema larger than 2 mm indicated that midline diastema is more prevalent in the late mixed dentition than in the early permanent dentition (P < 0.05).
Discrepancies in occlusal contact relationship
Maxillary overjet
The mean maxillary overjet of the sample was 2.9 mm. Table 2 shows maxillary overjet distribution according to gender, residency and dentition stage. About 55% of the subjects presented with a normal maxillary overjet ranged from 1 to 3 mm, 11.5% presented with a 0 mm overjet (edge-to-edge) and 33.5% presented with an overjet larger than 3 mm. The interaction between maxillary overjet and gender showed statistical significance difference, indicating that more boys than girls had an increased overjet that is, overjet >3 mm and more girls than boys had an edge-to-edge overjet (0 mm overjet). Statistically insignificant difference was found between urban and rural children, while the difference between stages of dental development was statistically significant (P < 0.05).
| Maxillary overjet | 0 mm n (%) | 1-3 mm n (%) | >3 mm n (%) |
|---|---|---|---|
| Gender | |||
| Female n=1501 | 181 (12.1)* | 859 (57.2)* | 461 (30.7)* |
| Male n=1502 | 164 (10.9)* | 792 (52.7)* | 546 (36.4)* |
| Residency | |||
| Urban n=1502 | 168 (11.2) | 812 (54.1) | 522 (34.7) |
| Rural n=1501 | 177 (11.8) | 839 (55.9) | 485 (32.3) |
| Dentition stage | |||
| Late mixed dentition n=785 | 107 (13.6)* | 420 (53.5)* | 258 (32.9)* |
| Early permanent dentition n=2218 | 238 (10.7)* | 1231 (55.5)* | 749 (33.8)* |
| Total | |||
| 3003 | 345 (11.5) | 1651 (55.0) | 1007 (33.5) |
*P < 0.05
Mandibular overjet and anterior openbite
Of the whole sample, 10.7% presented with mandibular overjet and 8.3% presented with anterior open bite [Table 3]. There are more children in the late mixed dentition with mandibular overjet and anterior open bite than those children in the early permanent dentition, the difference between stages of dental development was statistically significant (P < 0.05).
| Mandibular overjet and anterior open bite | Mandibular overjet (%) | Anterior open bite (%) |
|---|---|---|
| Gender | ||
| Female n=1501 | 11.3 | 9.2 |
| Male n=1502 | 10.1 | 7.3 |
| Residency | ||
| Urban n=1502 | 10.3 | 7.8 |
| Rural n=1501 | 11.1 | 8.8 |
| Dentition stage | ||
| Late mixed dentition n=785 | 12.4* | 11.1* |
| Early permanent dentition n=2218 | 8.9* | 7.3* |
| Total | ||
| 3003 | 10.7 | 8.3 |
*P < 0.05
Antero-posterior molar relation
The prevalence of discrepancies in the antero-posterior molar relationship is presented in Table 4. The results indicated that 69.4% of the sample presented with a normal molar relationship and 30.6% presented with an antero-posterior molar relationship discrepancy. Of the affected group 19.8% presented with a half a cusp displacement and 10.8% presented with a full cusp displacement. The differences in the distribution of antero-posterior molar between male and females and stages of dental development was statistically significant (P < 0.05), whereas the distribution of antero-posterior molar relation according to residency was statistically insignificant.
| Antero-posterior molar relation | Normal molar relation | Abnormal molar relation (half a cusp/full cusp displacement) |
|---|---|---|
| Gender | ||
| Female n=1501 | 71.6* | 28.4 |
| Male n=1502 | 67.2* | 32.8 |
| Residency | ||
| Urban n=1502 | 69.0 | 31.0 |
| Rural n=1501 | 69.8 | 30.2 |
| Dentition stage | ||
| Late mixed dentition n=785 | 68.8 | 31.2 |
| Early permanent dentition n=2218 | 70.0 | 30.0 |
| Total | ||
| 3003 | 69.4 | 30.6 |
*P < 0.05
DISCUSSION
Study and determination of criterion for different ethnic groups is essential to promote accurate diagnosis and planning for orthodontic treatment. Each ethnic group has certain characteristics that should not be taken as standards for other areas with different developmental and ecological foundation.
Intra-arch irregularities and malalignment
The majority of the sample 73.9% presented with a dentition in the early permanent stage. Most 12-year-old children will present with a dentition in the early permanent dentition stage, and the remainder will still be in the late mixed dentition stage.[26,27] A considerable number of 12-year-old girls presented with a dentition in the early permanent stage than boys. This is in accordance with the finding of Johnson and Harkness[28] and Drummond.[29]
The prevalence of crowding in this study was much higher than that of Al-Huwaizi[23] in his 13 year old Iraqi sample. The reason for this may be the difference in the criteria used as he recorded space discrepancies ≥2 mm. However, it was lower than that of Abdulla[17] and Batayine[18] in their Iraqi and Jordanian samples respectively and of Drummond[29] in his 12 year old South African sample.
This study revealed nonsignificant differences between the two genders concerning the distribution of crowding. This coincides with the findings of Al-Huwaizi,[23] while it contradicts that of Salonen et al.[30] who found that females had more crowding than males, which may be attributed to sample size, age group and racial variation. However this study reveals an insignificant difference in the prevalence of crowding between the late mixed dentition stage and the early permanent dentition stage.
The slight increase in the anterior arch dimension during normal development is not sufficient to overcome moderate to severe discrepancies. Crowding is therefore likely to persist into the permanent dentition, particularly if it was severe initially.[27]
One of the characteristic features of normal occlusion is arch continuity as expressed by proximal contact between all teeth in each dental arch. Factors such as mesial drift, transeptal fibers, the slope of the occluding cusp and the direction of occlusal forces contribute to the maintenance of this continuity.[31-33]
A comparison with other studies on spacing is difficult because of the differences in the age of the samples, criteria and method used to assess the space discrepancy. The Yemeni figure for maxillary central diastema is close to that of other Arab population sample results[17,18] and African population results,[29] but higher than that of Swedish population results[34,35] and this may be attributed to racial differences. There are more girls than boys with a midline diastema larger than 2 mm. These coincide with the findings of Drummond.[29]
On the other hand, Brunelle et al.[36] found that males had significantly more diastemas than females. Midline diastema is more prevalent in the late mixed dentition than in the early permanent dentition. This was also true for a midline diastema larger than 2 mm. The result of this study supports the findings by Richardson et al.[37] and Lindsey[38] who indicated that midline diastema reduces with the transition from the mixed dentition to the permanent dentition.
Discrepancies in occlusal contact relationship
The mean maxillary overjet of the sample was 2.9 mm, which was smaller than those found by many previous studies,[17,18,22] but was near to the finding of Al-Huwaizi[23] and Corruccini and Lee.[39]
Concerning gender differences, there are more boys than girls had an increased overjet that is, overjet >3 mm and significantly more girls than boys had an edge-to-edge overjet (0 mm overjet). This implies that 12-year-old boys have larger overjets and a higher prevalence of Class II malocclusions.
Furthermore, 12-year-old Yemeni girls tend to have fewer overjets larger than 3 mm and a higher prevalence of edge-to-edge overjet indicating a tendency toward Class III malocclusion. Furthermore, there are more 12-year-old children presented with a normal overjet in the early permanent dentition stage than 12-year-old children in the late mixed dentition stage. In other words, there is a higher prevalence of normal (1-3 mm) overjet in 12-year-old children in the permanent dentition stage than in the mixed dentition stage. Certain occlusal indicators including overjet, naturally improves with age.[36]
The differences between the prevalence of mandibular overjet of the present study and those reported by other investigators is difficult because of the differences in the age of the sample, criteria and method used to assess mandibular overjet in addition to possible racial variation. Anterior mandibular overjet that is, Class III malocclusion or anterior crossbite, is more prevalent in the late mixed dentition stage than in the early permanent dentition stage. Of the children, 8.3% presented with anterior openbite, in a malocclusion study in Nigeria, on 12- to 13-year-old children, Otuyemi et al.[40] have reported that anterior openbite is a common malocclusion trait, and that it occurs in 10.2% of the rural and urban Nigerian communities.[40]
Anterior openbite is more prevalent in the late mixed dentition stage than in the early permanent dentition stage especially among females compared with males. These improvements may be due to normal developmental changes and growth that occur during the transition from the mixed dentition stage to the permanent dentition stage.
The majority of the sample (69.4%) presented with a normal molar relationship, and this figure fell within the range of previously given prevalences (40-86.8%). It was also comparable to the figures given by several authors.[6,12,18,23,30,39]
Girls presented with more normal molar relationship than boys. This finding is in agreement with that of Drummond,[29] but it contradicts with that of Al-Huwaizi;[23] who found statistically insignificant difference between the two genders. The distribution of antero-posterior molar relation showed no statistically significant relation with residence. This finding is in agreement with that of Al-Huwaizi[23] and Ast et al.[41] While Salonen et al.[30] found that abnormal molar relation was more in urbans than rurals, and the result was statistically significant.
CONCLUSIONS
Crowding in the incisal segment was found in 31.5%, while spacing in the incisal segment was found in 24.3% of the sample.
A maxillary central diastema (>2 mm) was found in 1.8% of the sample, being more prevalent in the late mixed dentition than in the early permanent dentition.
The mean overjet of the sample was 2.9 mm; overjet >3 mm was more in boys than girls, while edge-to-edge overjet (0 mm overjet) was more in girls than boys.
Anterior mandibular overjet was found in 10.7% of the sample, being more in the late mixed dentition stage than in the early permanent dentition stage.
Normal antero-posterior molar relationship was found in 69.4% of the sample and abnormal antero-posterior molar relationship was found in 30.6% (19.8% half a cusp displacement and 10.8% full cusp displacement).
Source of Support:
Nil.
Conflict of Interest:
None declared.
References
- Orthodontics and the school child: A survey of 680 children. Br Dent J. 1945;79:278-80.
- [Google Scholar]
- The face in profile: An anthropological x-ray investigation on Swedish children and conscripts. Sverisk Tandi Tidsk (5B):40.
- [Google Scholar]
- A survey of malocclusion and some aetiological factors in 1000 Sheffield school children. Dent Practit. 1957;Vl:187-98.
- [Google Scholar]
- The frequency of the incidence of malocclusion in American Negro children aged 12-16. Angle Orthod. 1959;29:189-200.
- [Google Scholar]
- Prevalence of malocclusion in children aged 14 to 18 years. Am J Orthod. 1951;37:751-68.
- [Google Scholar]
- A survey of malocclusion and the need for orthodontic treatment in a Shropshire school population. Br J Orthod. 1974;1:73-8.
- [Google Scholar]
- Prevalence and severity of malocclusion in Israeli Arab urban children 13 to 15 years of age. Am J Orthod. 1983;84:337-43.
- [Google Scholar]
- Maxillary arch dimensions in Saudi and Egyptian population sample. Am J Orthod. 1984;85:83-8.
- [Google Scholar]
- Malocclusion and facial types in a group of Saudi Arabian patients referred for orthodontic treatment: A preliminary study. Brit J Orthod. 1987;14:143-6.
- [Google Scholar]
- Prevalence of malocclusion and need for orthodontic treatment in Saudi Arabia. Community Dent Oral Epidemiol. 1990;18:253-5.
- [Google Scholar]
- Occlusal features and perception: A sample of 13-17 years old adolescents. Master Thesis thesis
- [Google Scholar]
- Occlusal features and perception of occlusion of Jordanian adolescents: A comparative study with an Iraqi sample. Master Thesis thesis
- [Google Scholar]
- Prevalence of malocclusion in a sample of Lebanese schoolchildren: An epidemiological study. East Mediterr Health J. 1999;5:337-43.
- [Google Scholar]
- A survey of oral health in Iraq Population characteristics, occlusion and enamel mottling of senior secondary school students. Iraqi Dent J. 1982;9:8-16.
- [Google Scholar]
- A study of the prevalence of maxillary diastema and dental midlines deviation in Iraqi adults. Iraqi Dent J. 1989;14:128-36.
- [Google Scholar]
- Overjet and overbite distribution and correlation: A comparative epidemiological English-Iraqi study. Br J Orthod. 1986;13:79-86.
- [Google Scholar]
- Occlusal features, perception of occlusion, orthodontic treatment need and demand among 13-year-old Iraqi school children. Doctorate Thesis thesis
- [Google Scholar]
- Oral Health Surveys, Basic Methods (4th ed). Geneva: World Health Organisation; 1997. p. :47.
- A method of examining occlusal traits developed by the FDI commission on classification and statistics for oral conditions. Int Dent J. 1973;23:530-7.
- [Google Scholar]
- Handbook of Orthodontics (4th ed). Chicago: Year Book Medical Pub.; 1988.
- Contemporary Orthodontics (3rd ed). St Louis: Mosby; 2000.
- Prevalence of malocclusion and orthodontic treatment need in 10-year-old New Zealand children. Aust Orthod J. 2000;16:1-8.
- [Google Scholar]
- Orthodontic status and treatment need of 12-year-old children in South Africa: An epidemiological study using the dental aesthetic Index. Master Thesis thesis
- [Google Scholar]
- Need and demand for orthodontic treatment in an adult Swedish population. Eur J Orthod. 1992;14:359-68.
- [Google Scholar]
- Changes in crowding and spacing of the teeth with age. Dent Pract Dent Rec. 1969;19:218-24.
- [Google Scholar]
- Handbook of Orthodontics (3rd ed). Chicago: Yearbook Medical Publishers; 1972. p. :188-92.
- An experimental study of the effect of functional occlusion on mesial tooth migration in macaque monkeys. Arch Oral Biol. 1977;22:269-71.
- [Google Scholar]
- Prevalence and awareness of malocclusion in Swedish men. Community Dent Oral Epidemiol. 1978;6:308-14.
- [Google Scholar]
- Need and demand for orthodontic treatment in a group of women in Sweden. Eur J Orthod. 1982;4:231-42.
- [Google Scholar]
- Prevalence and distribution of selected occlusal characteristics in the US population, 1988-1991. J Dent Res. 1996;75:706-13.
- [Google Scholar]
- The upper mid-line space and its relation to the labial fraenum in children and in adults. A statistical evaluation. Br Dent J. 1977;15(143):327-32.
- [Google Scholar]
- Occlusal variation in Chinese immigrants to the United Kingdom and their offspring. Arch Oral Biol. 1984;29:779-82.
- [Google Scholar]
- Malocclusion and orthodontic treatment need of secondary school students in Nigeria according to the dental aesthetic index (DAI) Int Dent J. 1999;49:203-10.
- [Google Scholar]
- The prevalence and characteristics of malocclusion among senior high school students in upstate New York. Am J Orthod. 1965;51:437-45.
- [Google Scholar]




