

Translate this page into:
Paradigm shifts in orthodontic treatment with mini-implant anchorage
Address for Correspondence: Dr. Johnny Joung-Lin Liaw, Beauty Forever Dental Clinic, 10F, No. 20, Chang Chun Rd, Taipei, Taiwan, ROC. E-mail: ortho168@hotmail.com
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
After the applications of mini-implant anchorage, the envelope of orthodontic treatment was expanded and some treatment modes were changed because of more predictable tooth movement with empowered anchorage. The author tried to share his experience of TADs applications for clarifying the paradigm shifts of orthodontic treatment assisted with the mini-implant anchorage.
Keywords
skeletal anchorage
mini-implant anchorage
temporary anchorage devices

INTRODUCTION
Since the mini-implant anchorage is used in clinical orthodontic treatment widely,[1-7] the treatment planning of orthodontic treatment changes in some aspects basically. For instance, the selection of the extraction sites relies not only on the anchorage condition, but also the conditions of the teeth to be extracted; original extraction cases can be treated without extraction if posterior teeth can be moved distally with the mini-implant anchorage to gain space;[8-11] the protrusive profile after anterior crossbite correction can be avoid by distalize the whole upper and lower dentitions;[12-14] LeFort I maxillary impaction is the only solution for the adult cases with severe gummy smile in the past. With the help of mini-implant anchorage, a large amount of incisor intrusion can be expected, and esthetics can be improved a lot combined with the gingivoplasty.[15-18] Some patients with less than ideal conditions may avoid the orthognathic surgery and get their best orthodontic results with the help of mini-implant anchorage. Molar intrusion used to be very difficult tooth movement before the application of mini-implant anchorage. The use of mini-implant makes the molar intrusion feasible. Consequently, open bite correction with molar intrusion became a predictable treatment strategy.[19-24] The same concept could be applied to the high angle cases for better vertical control.[17,25] These conditions make the orthodontists reconsider the treatment plan with the mini-implant anchorage in mind, because the use of mini-implant shifts the paradigm in orthodontic treatment.
MINI-IMPLANT ANCHORAGE MAKES DIFFERENCE IN MAXIMAL ANCHORAGE CASES
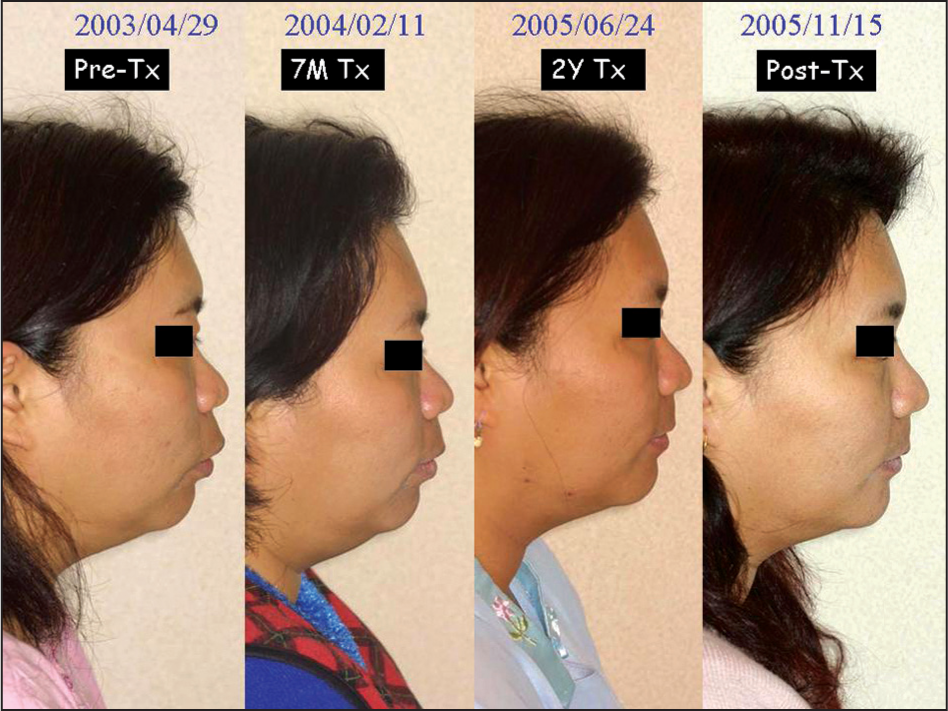
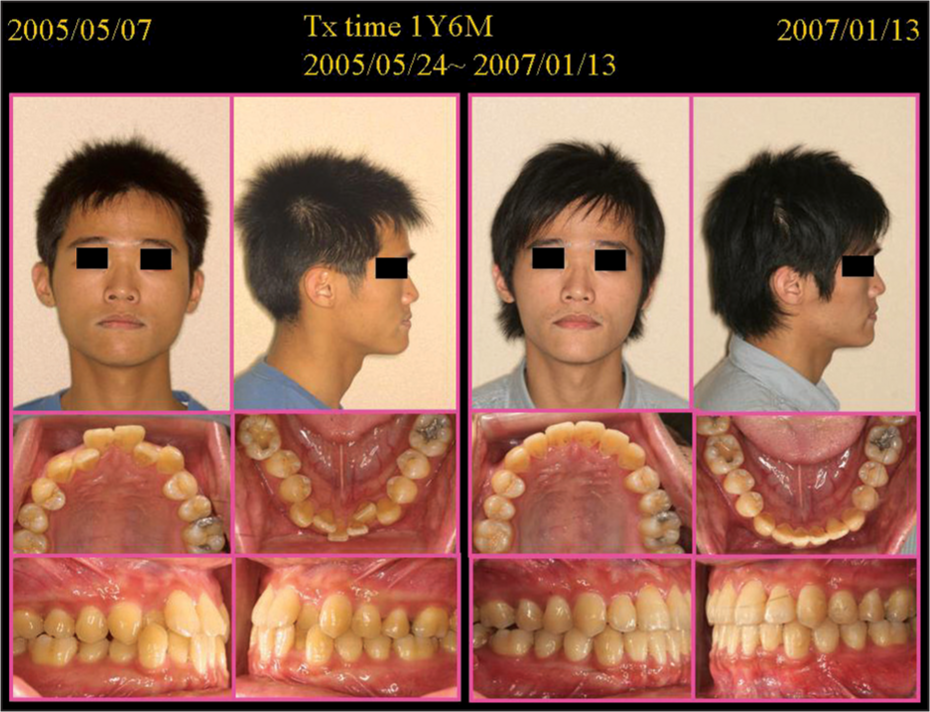
Some dentists had said that only the orthodontists who are not good at anchorage control will use the mini-implant anchorage for orthodontic treatment. In the past, the author usually had the protrusion patient wear high-pull headgear with J-hook as maximal anchorage control. Now mini-implant anchorage does an even better job than headgear because there is no need for patient compliance, and it works on a full-time basis. Better orthodontic results can be shown on more significant profile change, and better anchorage control can be proved on the cephalometric superimposition. Maybe it will be criticized that different situations make this comparison imprecisely. The author retreat a Class II protrusion case previously treated with high-pull J-hook and bite jumping appliance. There is still some Class II relationship remained after the first treatment. The patient complained of the relapse of protrusion. Retreatment with mini-implant anchorage was performed, and satisfactory result was achieved. The authors believe mini-implant anchorage does make a difference with the other anchorage sources [Figures 1 and 2].

- The left two photographs are before and after treatment records of this 4-premolar extraction case. After 5 years follow-up, patient complained of protrusion again. Retreatment with temporary anchorage devices on upper posterior areas end up with a satisfactory profile improvement

- The difference between the cephalometric superimpositions can be referred to the difference of anchorage between extra-oral headgear and mini-implant anchorage
WHOLE ARCH DISTALIZATION RATHER THAN MAXIMAL ANCHORAGE
If the protrusion is one of the patient’s concerns, extraction treatment will be more satisfactory. The amount of incisor retraction will be more predictable, and subsequent profile improvement will be more pleasing in the extraction treatment. With the help of mini-implant anchorage, some borderline cases can be treated with nonextraction approach but still get pleasing profile change. It is not only more conservative, but also more efficient by reducing treatment duration in the nonextraction treatment. Under certain circumstances, there is no extraction space available in the upper arch and there is a molar space to close in the lower arch, mini-implant anchorage can be used to distalize the whole upper arch to keep proper overjet during lower arch space closure. Exo-dentitional placement of mini-implant is important in this kind of application in order not to touching the roots during tooth movement [Figures 3 and 4].
- The progressive records of lateral profile revealed the power of mini-implant anchorage for this severe protrusion case

- Cephalometric superimpositions showed the upper incisors were retracted about 12 mms at the incisal edge. The achieved tooth movement was not only maximal retraction without any anchorage loss, but also further total arch distalization by 5 mm after the extraction spaces were all closed
MOLAR DISTALIZATION IN SEVERE CROWDING CASES
Arch length discrepancy can be resolved by extractions of teeth or arch expansion. If the choice is arch expansion, there are three directions:
Anterior
Posterior and
Transverse.
Anterior expansion makes the incisors advanced and proclined, which is unfavorable for Mongolian patients that are usually more protrusive than Caucasian patients. Transverse expansion is more favorable in the Caucasians because they are more dolichocephalic than Mongolians which are more brachycephalic. Hence, posterior expansion is the best treatment choice for the Mongolian crowding cases. If the molars are not distalized successfully in the Mongolian crowding cases, the incisors will be advanced, and the profile will become protrusive. Exo-dentitional mini-implant can be used to distalize both the upper and lower posterior teeth and get the space to align the whole dentition without anterior expansion [Figure 5].
- The use of mini-implant anchorage in severe crowding cases can avoid the protrusion in nonextraction treatment and the midface dish-in after extraction treatment
LOWER MINI-IMPLANT ANCHORAGE TO CORRECT THE ANTERIOR CROSSBITE
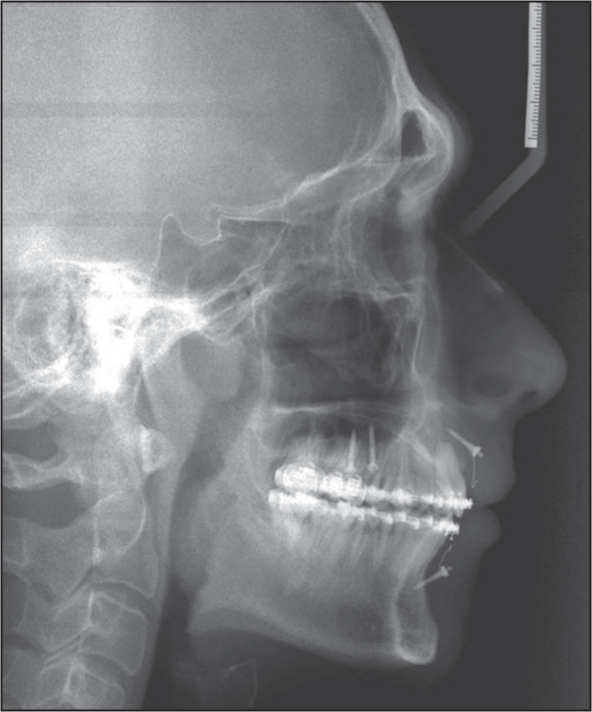
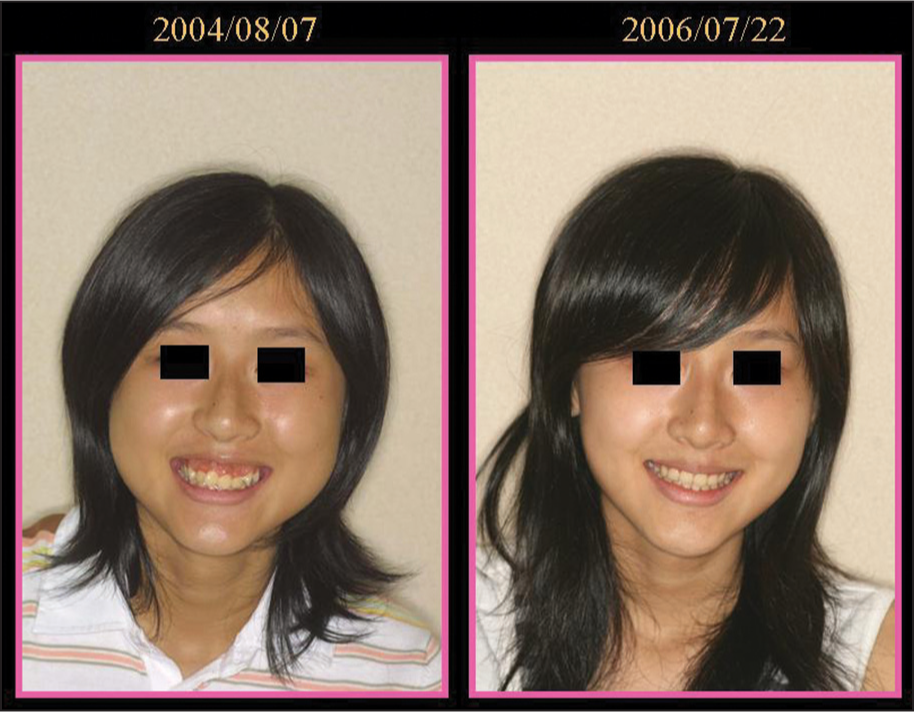
Class III malocclusions are quite common in Asian population, and the bimaxillary dentoalveolar protrusion is another common characteristic in oriental races. There is a common problem for the orthodontists to consider whether the patients will become protrusive after anterior crossbite correction. If the answer were yes, then maybe extraction is a better option for the treatment plan. With the help of mini-implant anchorage, Class IIII malocclusion can be treated successfully with nonextraction approach without subsequent perioral protrusion. This paradigm shift in treatment of Class III malocclusion greatly reduces the treatment duration and achieves more pleasing profile change after anterior crossbite correction [Figures 6 and 7].
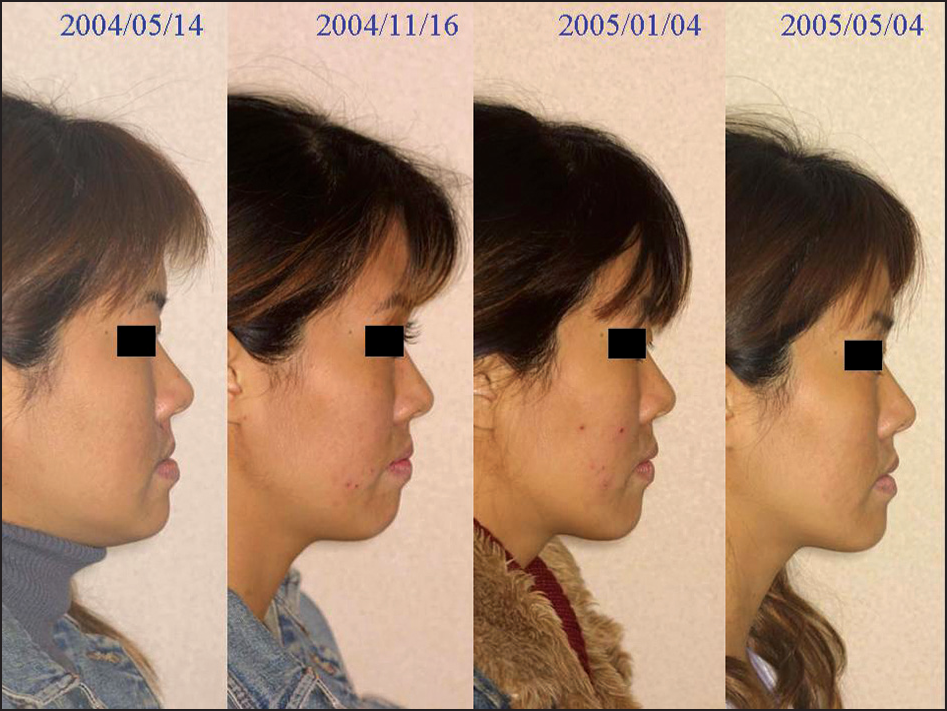
- The progressive records of lateral profile of a Class III case with anterior crossbite
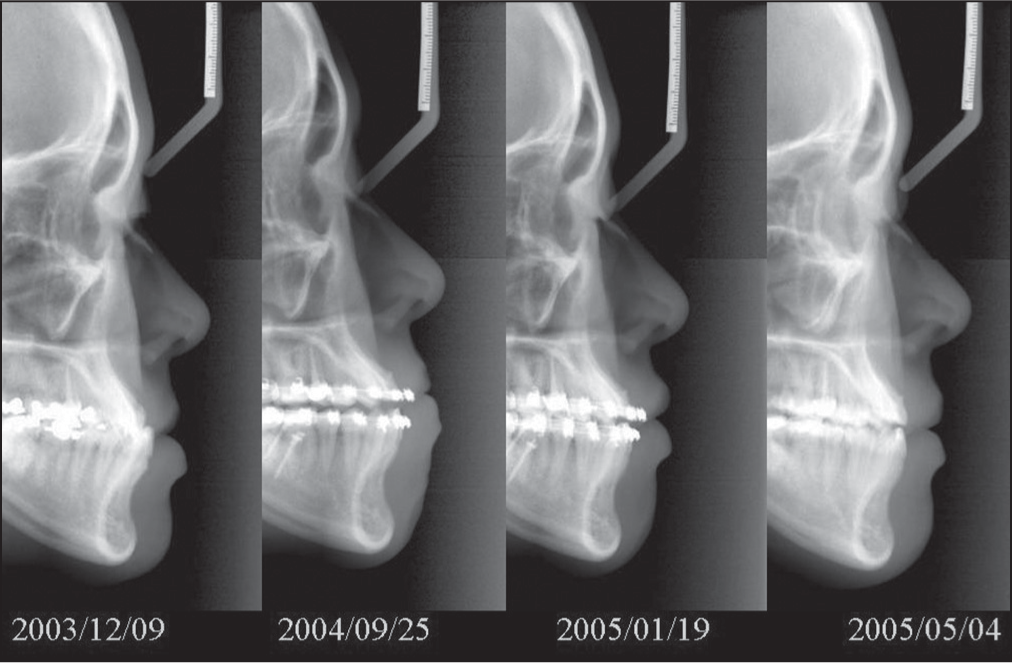
- The corresponding cephalograms of the lateral profiles in Figure 6. Correction of anterior crossbite often turned out protrusion in lateral profile, which usually required four bicuspids extraction to retract the profile. With the help of mini-implant anchorage, we can maintain or even improve the lateral profile while the anterior crossbite was corrected in Class III cases
MINI-IMPLANT ANCHORAGE IS ALSO IMPORTANT IN SOME ADOLESCENT PATIENTS
Usually the anchorage requirement is not very critical in the adolescent patients because there is some growth that may help the correction of malocclusion. But in some severe adolescent patients, anchorage gained from the favorable growth is not enough to correct the skeletal discrepancy. Extra anchorage can be provided by mini-implant without any noticeable side-effects. No interference of growth was observed after the use of mini-implant anchorage. Favorable growth pattern can be seen after the proper use of mini-implant anchorage [Figure 8].

- Although the growth potential is good for adolescent patients, which makes the anchorage requirement is not so critical for most adolescent patients, it is still very important for some severe protrusion cases
DEEPBITE CORRECTION WITH ANTERIOR SUBAPICAL MINI-IMPLANT
Besides anterior-posterior control, the mini-implant anchorage can be used to control the vertical problem successfully. In fact, this is the first application of mini-implant anchorage proposed in modern orthodontics, which was published in JCO, 1983. Dr. Creekmore inserted a vitallium miniscrew beneath the ANS to provide the anchorage for upper anteriors intrusion. Although this approach was proved to be effective, many orthodontists still regard this as the last resort because the anatomical limitation in the upper anterior regions makes the patients more discomfort. The authors change the insertion technique to be closed methods in the upper anterior regions so that the extension ligature wire is no more too irritating to use. If the deepbite can be corrected efficiently with mini-implant anchorage, the large overjet can be corrected subsequently without occlusal interference. So with mini-implant anchorage in anterior and posterior regions, a difficult situation of large overjet and deep overbite can be resolve at the same time efficiently [Figures 9 and 10].

- Anterior subapical miniscrews for intrusion were very efficient for bite opening
- Anterior subapical areas were quite safe to insert miniscrews
AN EFFECTIVE SOLUTION FOR GUMMY SMILE IN ADULT CASES
In the past, the only way to correct gummy smile in the adult cases is LeFort I maxillary impaction. Now, the other way to correct gummy smile is anterior subapical mini-implant anchorage to intrude the upper anteriors. The problem of this approach may exist in some cases with relatively short clinical crowns. Gingivoplasty or crown lengthening may be indicated after or even during orthodontic treatment [Figure 11].
- Anterior subapical miniscrews were helpful for the correction of gummy smile, even in nongrowing patients
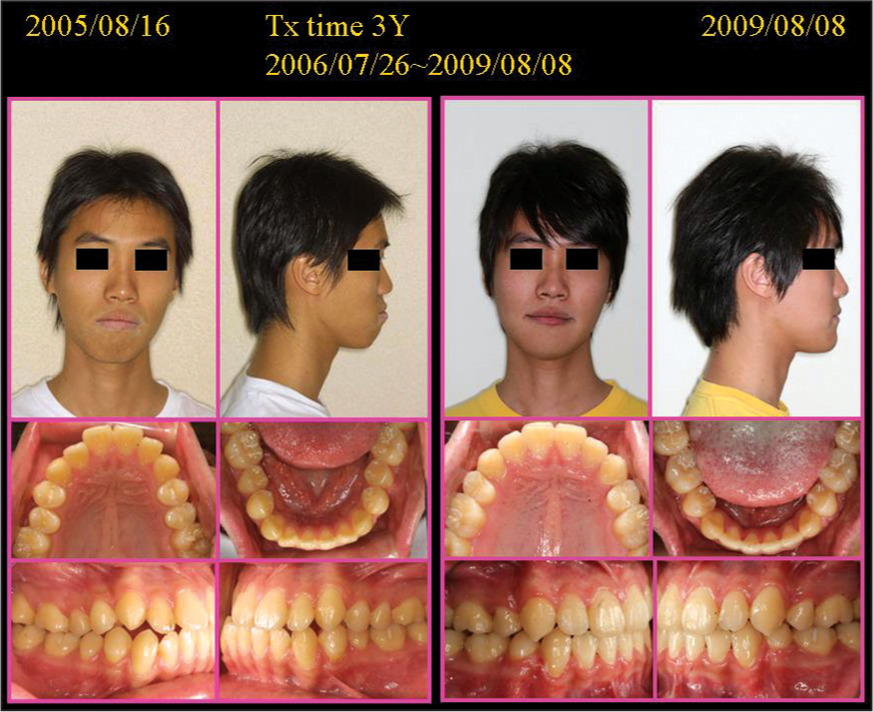
EXTRACTION PATTERN DEPENDS MORE ON THE PROGNOSIS THAN ON THE ANCHORAGE VALUE
The anchorage values of the different extraction patterns change with the application of mini-implant anchorage. The first bicuspids extraction is the regular extraction pattern for the protrusion cases. The choice of this extraction pattern is based upon the anchorage consideration. If mini-implant anchorage can be used, there will be no difference to extract first or second bicuspids. The choice of tooth to be extracted will be focused on the conditions of the tooth, such as large decays or restorations, poor periodontal condition, endodontically involved or crowns [Figures 12 and 13].
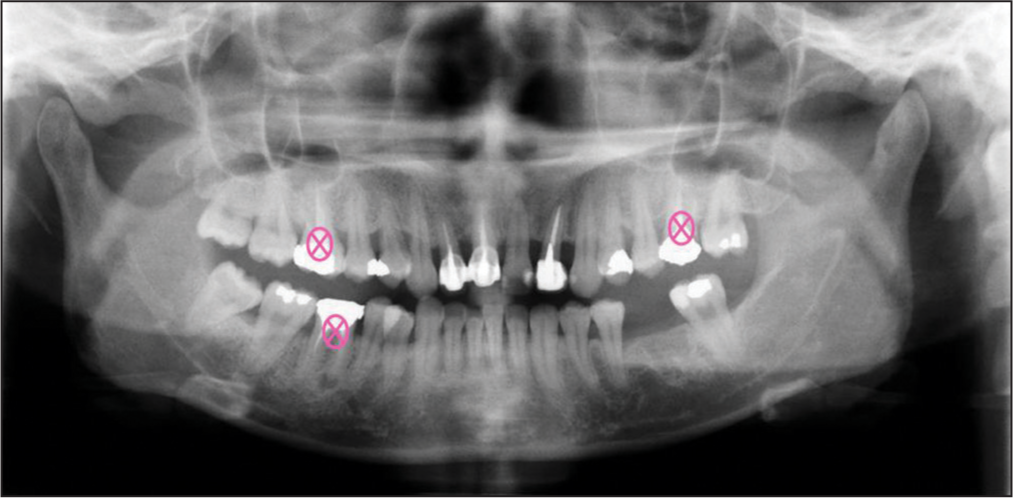
- The applications of miniscrews makes possible to decide treatment plan according to the prognosis of the teeth rather than the anchorage value

- With the help of miniscrews, profile could be retracted successfully by space closure of four first molars
GENUINE MOLAR INTRUSION IS FEASIBLE WITH MINI-IMPLANT ANCHORAGE
It is easier for any tooth to be extruded than to be intruded, so leveling is extrusive in nature. Reactive extrusive force is inevitable for any appliance except mini-implant anchorage device. With the help of mini-implant anchorage, genuine molar intrusion is much more predictable. Besides molar elongation, genuine molar intrusion is also very important for posterior crossbite correction. The force system with mini-implant anchorage avoids the unfavorable extrusive forces of the criss-cross elastics. In some open bite cases, the intrusion of the molars makes the mandible autorotated counterclockwisely to close the anterior open bite. The applications of mini-implant anchorage do change the biomechanical considerations in some difficult situations [Figures 14 and 15].

- The vertical control by mini-implant anchorage makes the open bite treatment more predictable

- Cephalometric superimpositions showed counterclockwise rotation of mandible by means of posterior intrusion of both arches
VERTICAL CONTROL IN HIGH ANGLE CASES: FROM GOOD TO GREAT
The optimal force system for high angle, protrusive cases was proposed to be the upper and lower posterior miniscrews for anterior retraction and the upper and lower anterior subapical miniscrews for overbite control. The vertical control can be achieved simultaneously with A-P anchorage control. The directional force system in Tweed-Merrifield technique cannot be simulated by posterior miniscrews easily because of the proper implant sites are much lower than the ideal implant site for high-pull direction. The combination use of the posterior and anterior miniscrews can simulate the directional force system of Tweed-Merrified technique without patients’ compliance. These combination use of posterior and anterior miniscrews on both maxillary and mandibular dentitions makes the mandible rotated counterclockwisely to advance the chin point and get so-called “mandibular response” in adult patients. It helps those high angle, protrusive patients to get the greatest improvement by nonsurgical approach [Figures 16-18].
- High angle protrusion cases with retruded chin could be treated with mini-implant anchorage to achieve maximal retraction and active vertical control
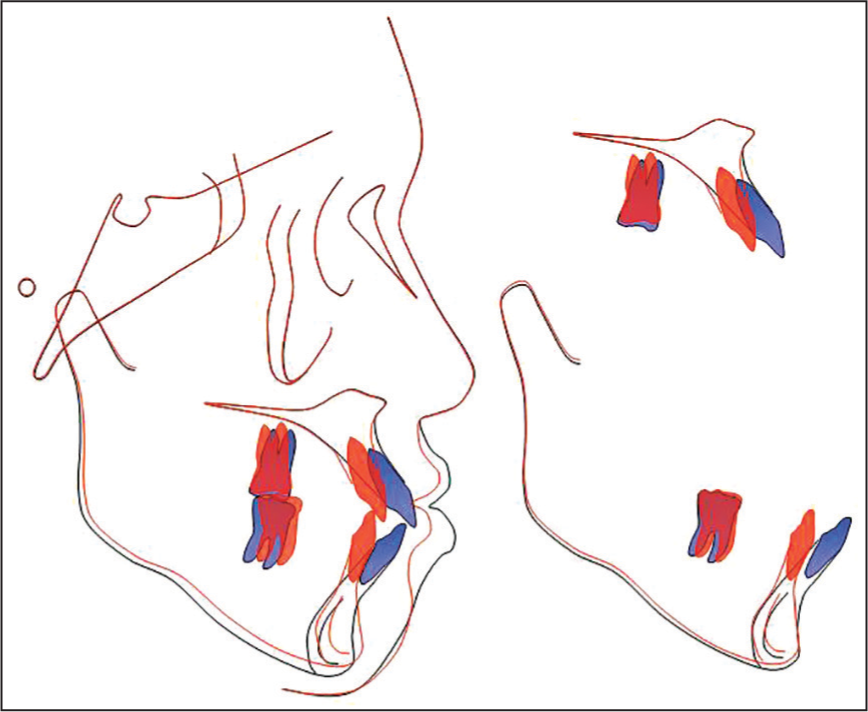
- Cephalometric superimpositions showed maximal retraction and overall intrusion on both arches
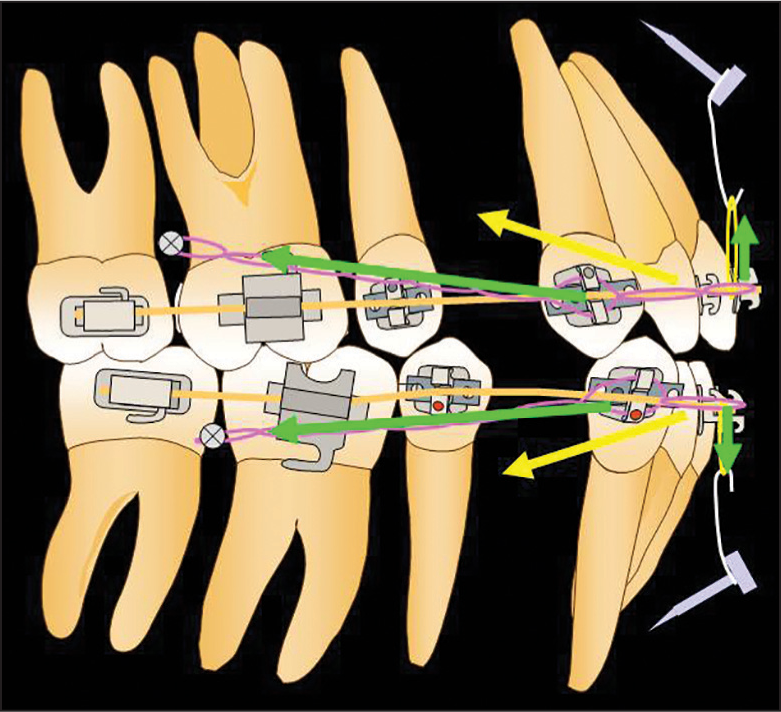
- This is the combined intrusion and retraction force system suggested for the high angle protrusion cases
CONCLUSIONS
All the above are major paradigm shifts during my journey of mini-implant anchorage. I think the applications of mini-implant anchorage have created a new world in orthodontics. It is a quite powerful anchorage device and deserve every orthodontist to keep it in mind during making a treatment plan.
References
- Clinical applications of the Miniscrew Anchorage System. J Clin Orthod. 2005;39:9-24.
- [Google Scholar]
- Micro-implant anchorage for treatment of skeletal Class I bialveolar protrusion. J Clin Orthod. 2001;35:417-22.
- [Google Scholar]
- Uprighting mandibular second molars with direct miniscrew anchorage. J Clin Orthod. 2007;41:627-35.
- [Google Scholar]
- Miniscrew anchorage used to protract lower second molars into first molar extraction sites. J Clin Orthod. 2003;37:575-9.
- [Google Scholar]
- Intrusion of overerupted maxillary molars with miniscrew anchorage. J Clin Orthod. 2006;40:378-83.
- [Google Scholar]
- Correction of a canted occlusal plane with miniscrews in a patient with facial asymmetry. Am J Orthod Dentofacial Orthop. 2006;130:244-52.
- [Google Scholar]
- Distal movement of maxillary molars in nongrowing patients with the skeletal anchorage system. Am J Orthod Dentofacial Orthop. 2006;129:723-33.
- [Google Scholar]
- Treatment of Class II protrusion with severe crowding using indirect miniscrew anchorage. Angle Orthod. 2007;77:1109-18.
- [Google Scholar]
- En-masse distalization with miniscrew anchorage in Class II nonextraction treatment. J Clin Orthod. 2006;40:472-6.
- [Google Scholar]
- Class III nonextraction treatment with miniscrew anchorage. J Clin Orthod. 2006;40:480-4.
- [Google Scholar]
- Treatment of Class III relapse due to late mandibular growth using miniscrew anchorage. J Clin Orthod. 2008;42:400-11.
- [Google Scholar]
- Distal movement of mandibular molars in adult patients with the skeletal anchorage system. Am J Orthod Dentofacial Orthop. 2004;125:130-8.
- [Google Scholar]
- Treatment of skeletal-origin gummy smiles with miniscrew anchorage. J Clin Orthod. 2008;42:285-96.
- [Google Scholar]
- Severe high Angle Class II Division 1 malocclusion with vertical maxillary excess and gummy smile: A case report. Am J Orthod Dentofacial Orthop. 1999;116:317-20.
- [Google Scholar]
- Correction of deep overbite and gummy smile by using a mini-implant with a segmented wire in a growing Class II Division 2 patient. Am J Orthod Dentofacial Orthop. 2006;130:676-85.
- [Google Scholar]
- The use of skeletal anchorage in open bite treatment: A cephalometric evaluation. Angle Orthod. 2004;74:381-90.
- [Google Scholar]
- Severe anterior open-bite case treated using titanium screw anchorage. Angle Orthod. 2004;74:558-67.
- [Google Scholar]
- Treatment of severe anterior open bite with skeletal anchorage in adults: Comparison with orthognathic surgery outcomes. Am J Orthod Dentofacial Orthop. 2007;132:599-605.
- [Google Scholar]
- Skeletal anchorage system for open-bite correction. Am J Orthod Dentofacial Orthop. 1999;115:166-74.
- [Google Scholar]
- Closing anterior open bites by intruding molars with titanium miniplate anchorage. Am J Orthod Dentofacial Orthop. 2002;122:593-600.
- [Google Scholar]
- Bimaxillary orthognathic surgery in a patient with long face: A case report. Int J Adult Orthodon Orthognath Surg. 1999;14:304-9.
- [Google Scholar]




