

Translate this page into:
Plaque accumulation and Streptococcus mutans levels around self-ligating bracket clips and elastomeric modules: A randomized controlled trial
Address for Correspondence: Prof. Vaid Nikhilesh, Department of Orthodontics, YMT Dental College, Navi Mumbai, Maharashtra, India. E-mail: orthonik@gmail.com
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Aim
To determine the effect of two different ligating systems that is, elastomeric modules and self-ligating (SL) bracket systems (Smartclip - 3M Unitek) with respect to harboring bacterial plaque in fixed orthodontic treatment.
Objectives
To assess, evaluate, and compare the amount of plaque accumulation and Streptococcus mutans colonization around elastomeric ligation and SL clips in the smart clip appliance.
Materials and Methods
A total of 111 orthodontic patients scheduled for fixed orthodontic treatments were selected for this split maxillary arch study. All the patients were bonded with smart-clip (3M Unitek) SL brackets, and the wire was placed into the bracket slots, on the randomly selected hemi arch, elastomeric modules were placed for the study to be conducted. Microbial and periodontal plaque accumulation was recorded at 3-time intervals post ligation. Plaque index-by Silness and Loe, modified Quigely Hein index, bleeding on probing were evaluated, and biofilm was collected from the tooth surface after 30 days and placed in petri dishes containing Mitis Salivarius agar for bacterial culturing.
Result
It was observed that the side where ligation was done with elastomeric modules accumulated more plaque and increase in S. mutans colony forming units as compared to the side without external ligation (P < 0.05).
Conclusion
Reduced bacterial colonization and better plaque control was seen with SL orthodontic bracket appliance system as compared to conventional ligation method.
Keywords
Biofilm retention
plaque control
randomized clinical trial
self-ligation
Streptococcus mutans levels
white spot lesions

INTRODUCTION
Orthodontic treatment does improve the self-image of the patients through the provision of better esthetics and a more attractive smile. However, the journey of orthodontic treatment poses an increased risk of tooth decalcification due to plaque accumulation around the brackets leading to the formation of white spot lesions.[1,2] These changes are an esthetic problem that persist for many years after treatment.[3,4] In addition, decalcification related to bonded orthodontic appliances appears to occur primarily near the appliance and not farther away along the facial surface. Gorelick et al.[5] reported that the tooth most commonly affected was the maxillary lateral incisor.
Addition of external ligation over these brackets which are used to fix the wires within the bracket slot create added plaque retentive sites that are suitable for bacterial colonization and biofilm formation impending adequate oral hygiene maintenance leading to increased risk of caries in orthodontic patients.[6]
Zachrisson and Zachrisson[7] stated the etiology and pathogenesis of periodontal diseases are multifactorial, but dental plaque certainly is an essential precursor. The presence of elastomeric modules and stainless steel ligatures are taken into account for microbial dental plaque retention which causes enamel demineralization due to decrease in pH level caused by increase in number of acid-producing bacteria, mainly Streptococcus mutans and lactobacilli,[8,9] which ultimately results in appearance of white spots and caries in approximately 50% of patients undergoing fixed orthodontic treatment.[4,5,10]
Self-ligating (SL) brackets were introduced to orthodontics several decades ago. One of the most favorable aspects with the use of SL brackets clinically, possibly would be the elimination of elastomeric ligation and steel ligature wires.[11,12] Thereby advantageous in the eradication of cross-contamination that may occur accidentally during ligature placement, the possibility of better oral hygiene because of reduced complexity of the bracket system, which has fewer retentive sites for microbial colonization. Manufacturers have also reported that due to the SL designs, SL brackets accumulate less dental plaque when compared to conventional ligation appliance bracket systems.
The aim of this randomized clinic trial was to determine the effect of two different ligation methods on harboring bacterial plaque and subsequent S. mutans levels that is, to compare the microbiological environment and the clinical parameters by means of a de novo plaque growth experiment within a duration of 30 days at intervals of 7 (T1), 15 (T2) and 30 (T3) days respectively.
MATERIALS AND METHODS
A randomized clinical trial involving a set of 111 patients were evaluated for the initiation and progression of periodontal disease with the use of fixed SL orthodontic bracket appliance system when compared to conventional ligation method over a period of 30 days at intervals of 7 (T1), 15 (T2) and 30 (T3) days, respectively.
Each patient with permanent dentition, free of dental plaque, motivated for good oral hygiene, and who were willing to take part in the study were included, and an informed consent was obtained for the same. Patients with systemic diseases, periodontal disease (pocket depth >4 mm), those taking antibiotics 3 months prior to study and Smokers were excluded from the study.
The sample size was determined by power analysis based on the results of the pilot study that showed that the Plaque accumulation and bacterial biofilm retention was more on the side with conventional ligation to that of the control side.
P0 = Population proportion
Pα= Sample proportion
α = Significance level
1-β = Power
According to Pandis et al.,[13] with a permissible error of 5%, that is, α = 0.05, the sample size of 16 patients per group yields a statistical power close to 0.8; our sample consisted of a greater number than that, for this split-mouth design.
The recruitment, allocation and follow-up details are featured in the CONSORT chart [Figure 1].
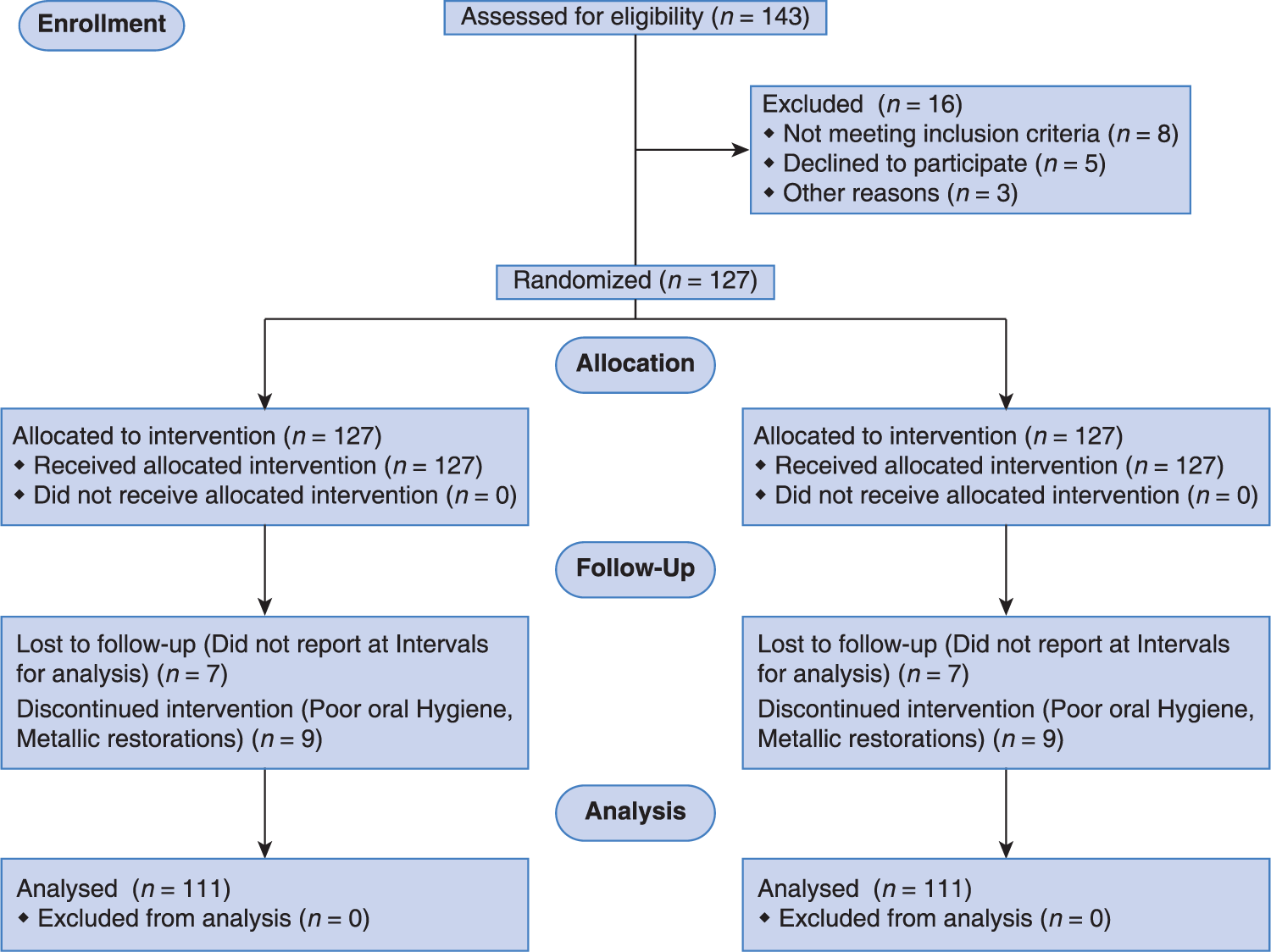
- CONSORT flow diagram of participants through each stage of trial
In this multi-centric randomized trial, a week before beginning orthodontic treatment for these patients, oral hygiene instructions were reinforced, proper brushing technique that is, modified bass technique of brushing was demonstrated to all patients to avoid bias in the method of brushing, use of interdental floss was advised, no professional cleaning was done for these patients prior to study and they were advised not to use any chemical antiplaque agents or mouthwashes as a part of the study design.
Only patients undergoing treatment with the smart clip SL brackets (3M Unitek, Monrovia, USA) were recruited for this study. This was done to prevent any hindrance in the ongoing treatment protocols, as well have standardized bracket designs in the control and experimental group.[14,15] Smart clip brackets are essentially twin brackets with the addition of a clip; whereby they render themselves convenient to ligature placement. This was essential for comparing two sides in our study. The maxillary dentition was used for the study to be conducted.
The maxillary dentition was divided into two halves that is, right and left hemi arch, the elastomeric modules were placed from the central incisor to 2nd premolar in one-half randomly selected. Whereas, on the other half of the arch the wire was press inserted into the bracket slot and was secured with the spring clip [Figure 2].

- Elastomeric modules placed on left hemi arch
A plaque swab was collected separately for the two halves of each patient and was subjected to bacterial culturing with Mitis Salivarius agar selective for growth of S. mutans species, incubated for 48 h. The growth obtained on the petridish was then counted to determine the colony forming units (CFU) for the maxillary hemiarches with conventional ligation and SL [Figure 3a and b].

- (a and b) Plaque swab collection on maxillary right (self-ligation) and left (conventional ligation with elastomeric modules) hemiarch
The patients were then recalled after 7 (T1) days evaluated for presence of the amount of plaque deposits on the teeth around the orthodontic brackets using:
Plaque index-by Silness and Loe.[16]
Modified Quigely Hein index[17] using disclosing agent and
Bleeding on probing.
The disclosing agent used for the study conducted was erythrosine. The patient was first asked to rinse the mouth with plain water, and then the area was dried using 3-way syringe. The disclosing agent was then applied onto the tooth surface around the orthodontic brackets mainly in the gingival portion of the teeth from 2nd premolar on the right side to the 2nd premolar on the left side with the use of cotton pellets.
Same procedure was repeated at 15 (T2) and 30 (T3) days respectively. At the 30th day the plaque swab was again collected with sterile cotton swab from the bracket margins of all the patients separately for the right and left maxillary hemiarch and subjected to bacterial culturing and incubated for 48 h at 37° in an incubator and colonies were assessed [Figure 4a-c].
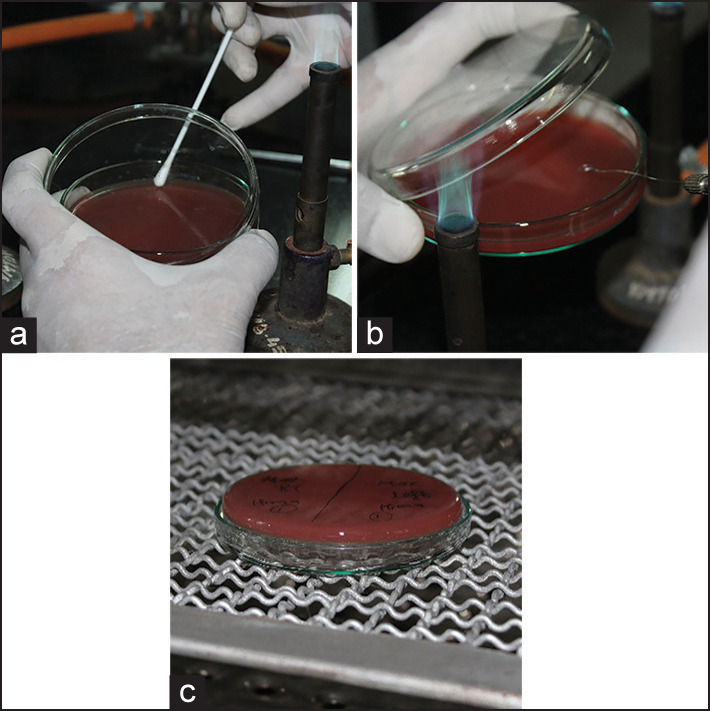
- (a-c) Plaque swab inoculation in petridish and incubation at 37° for 48 h respectively
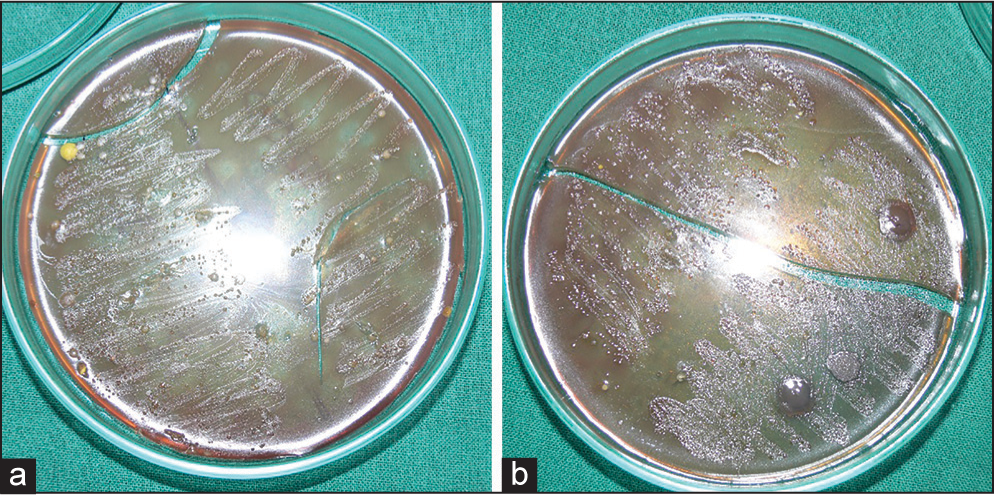
The readings then were made for each tooth included in the study of the maxillary arch and the results were then obtained by the visual examination and as per the guidelines given by the above-mentioned indices as well as by the difference in the CFUs of the S. mutans levels growth on the selective media [Figure 5a and b]. The results were separately recorded for each side of the arch and compared to the side of the maxillary arch where the elastomeric ligation was done.
-
Streptococcus mutans growth at the beginning (a), at 30 days (b)
Statistical analysis
One-way analysis of variance test followed by Tukey test was performed to test the differences in amount of plaque accumulation scores in left and right quadrant measured by the indices performed at 7th, 15th and 30th days respectively. Furthermore, the comparison to test the difference in S. mutans CFU/ml at the beginning and 30th day was done using mean bacterial counts. P < 0.05 was considered as statistically significant.
RESULT
Biofilm was detected using the disclosing agents. Based on the readings available and the calculation of the two indices taken as a part of the study along with evaluation of bleeding and probing, it was found that there was presence of more amount of plaque deposits on the side of maxillary dentition where elastomeric ligation was done as those areas were inaccessible for proper brushing as compared to the other side of the arch where less deposits were observed due to simplicity of bracket design and easy accessibility for proper brushing and maintenance of oral hygiene [Figure 6]. Also, the microbiological analysis showed a significant amount of difference in plaque biofilm accumulation depending on the ligation method. The elastomeric module ligation had the mean value of 6.39 log colony-forming units per milliliter (range 5.63-7.21). SL had less of plaque biofilm as compared to elastomeric modules, an average of 4.34 log CFUs per milliliter (range 3.03-4.98) [Figure 7].
- The difference in the amount of bacterial plaque deposits with two methods of ligation
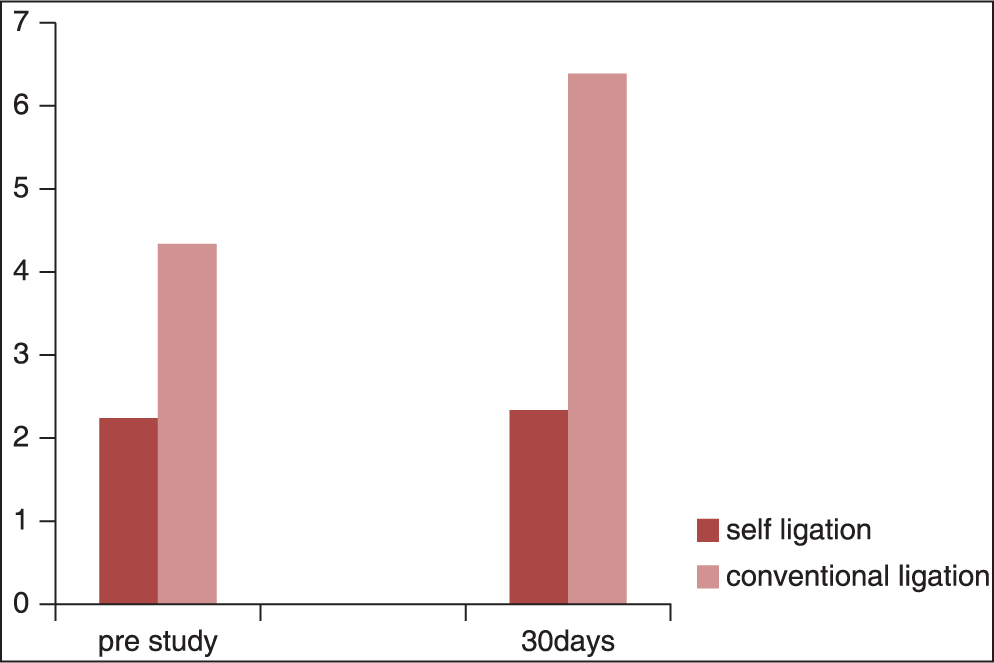
-
Streptococcus mutans levels over a period of 30 days
Also found in the study conducted was discoloration of the elastomeric modules due to food deposits accumulation giving it a very unaesthetic appearance and also inducing further bacterial colonization in the area leading to gingivitis, which is an advantage with the SL bracket (smart clip [3M Unitek]) system due to simplicity of the design and less retentive areas for plaque accumulation.
DISCUSSION
Effects of fixed orthodontic mechano-therapy on plaque biofilm formation and bacterial colonization have been evaluated in many studies. However, adhesion of plaque bacteria with different ligation methods have been evaluated in a few studies.[6,8,9,18-21]
The dental plaque formation varies among patients due to certain factors like oral hygiene, diet, age, systemic diseases and other host factors also dento-alveolar malocclusion leads to increased plaque retention.
The development of the acid-etch bonding technique and the subsequent orthodontic application via the bonding of brackets in lieu of full banded appliances have not only facilitated the efficiency of orthodontic appliance construction, but also reduced the amount of tooth surface covered with appliances.[22] Nonetheless, bonded orthodontic brackets still hinder access for good oral hygiene and create microbial shelters, resulting in the accumulation of plaque.[6,23] The appliance architecture — specifically, the archwire ligation method - is an additional factor influencing bacterial colonization.
Previous studies that compare the influence of Self-ligating brackets and conventional brackets on periodontal health use elastomeric ligature as ligation method, although it has been shown that the elastomeric ligatures represent a bio-hostile material.[6,9,21,24]
Our study, a randomized clinical trial in determining the effect of two different ligating systems on harboring bacterial plaque accumulation and S. mutans colonization that is, to compare the microbiological environment and the clinical periodontal parameters by means of a de novo plaque growth experiment within a duration of 30 days at intervals of 7 (T1), 15 (T2) and 30 (T3) days respectively, which makes it a simple and effective chairside method for evaluating presence of plaque deposits.
The smart clip bracket is the only SL bracket, the design of which is similar to any preadjusted edge-wise appliance bracket. The uniqueness of the study design is to quantify the difference in plaque adherence, in a similar environment when the only variable, that is, the elastomeric ligature is added to the conditions in experimental group.
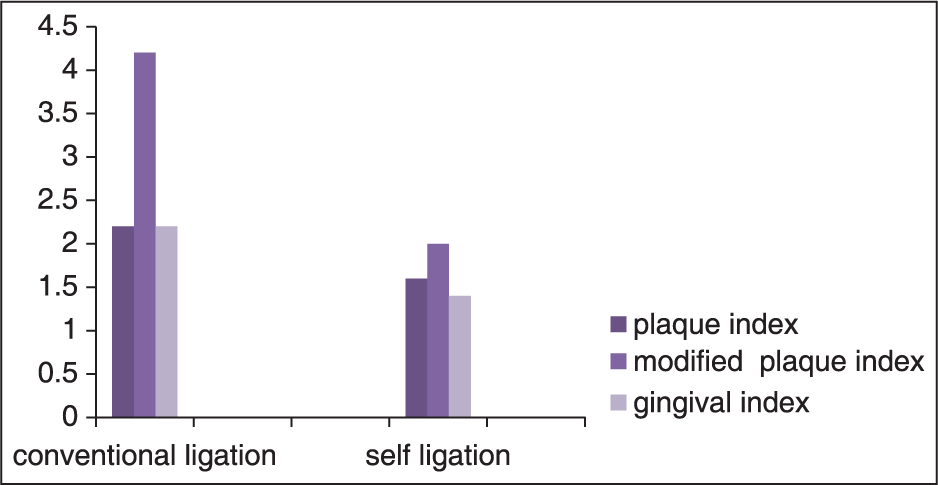
In this trial, the time interval with respect to individual quadrants showed clinically insignificant results (P > 0.05), while the comparison between the two ligation methods resulted in statistically significant values (P < 0.05) suggesting increased plaque levels with convention ligation as compared to SL [Table 1, Figure 8].
| N | Mean | SD | t-test | D.F. | P-value | |
|---|---|---|---|---|---|---|
| Plaque index | ||||||
| Conventional ligation | 111 | 2.07 | 0.70 | 2.366 | 28 | 0.025* |
| Self ligation | 111 | 1.53 | 0.52 | |||
| Modifi ed plaque Index | ||||||
| Conventional ligation | 111 | 3.80 | 1.08 | 4.731 | 28 | 0.000** |
| Self ligation | 111 | 2.00 | 1.00 | |||
| Gingival index | ||||||
| Conventional ligation | 111 | 2.20 | 0.68 | 3.666 | 28 | 0.001** |
| Self ligation | 111 | 1.40 | 0.51 | |||
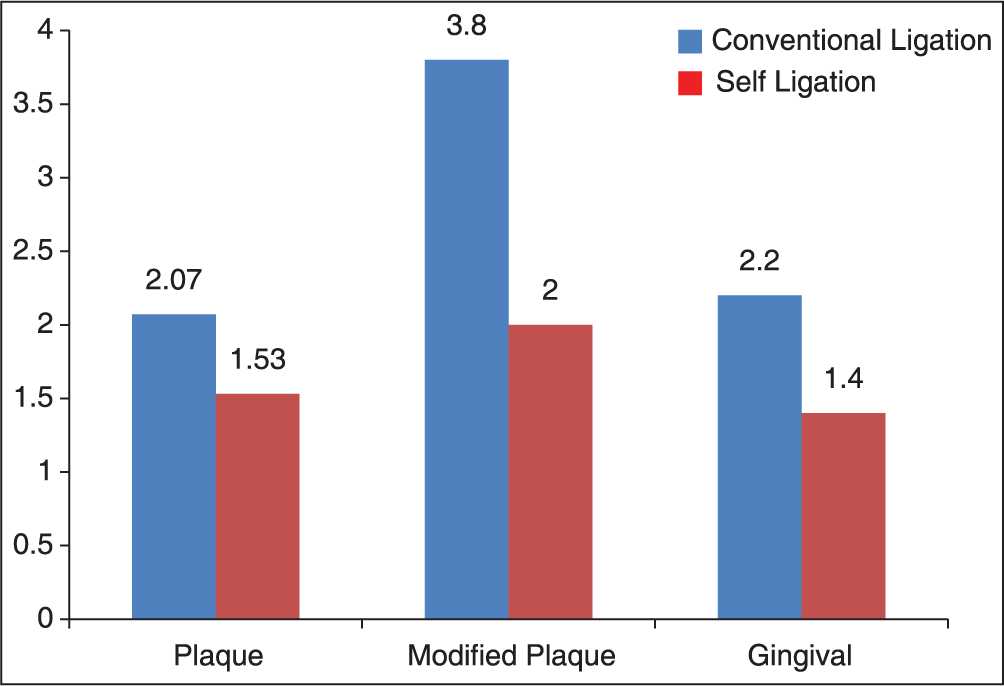
- Comparison of indices between maxillary hemiarch with conventional ligation and self-ligation
Also when arch with conventional ligation with control maxillary hemiarch were evaluated by the total means of scores obtained irrespective of the indices indicated that since P < 0.05 indicates significant difference between the means of two quadrants when taken irrespective of index [Table 2, Figure 9].
| N | Mean | SD | t-test | D.F. | P-value | |
|---|---|---|---|---|---|---|
| Conventional ligation | 333 | 2.69 | 1.145 | 5.134 | 88 | 0.000** |
| Self ligation | 333 | 1.64 | 0.75 |
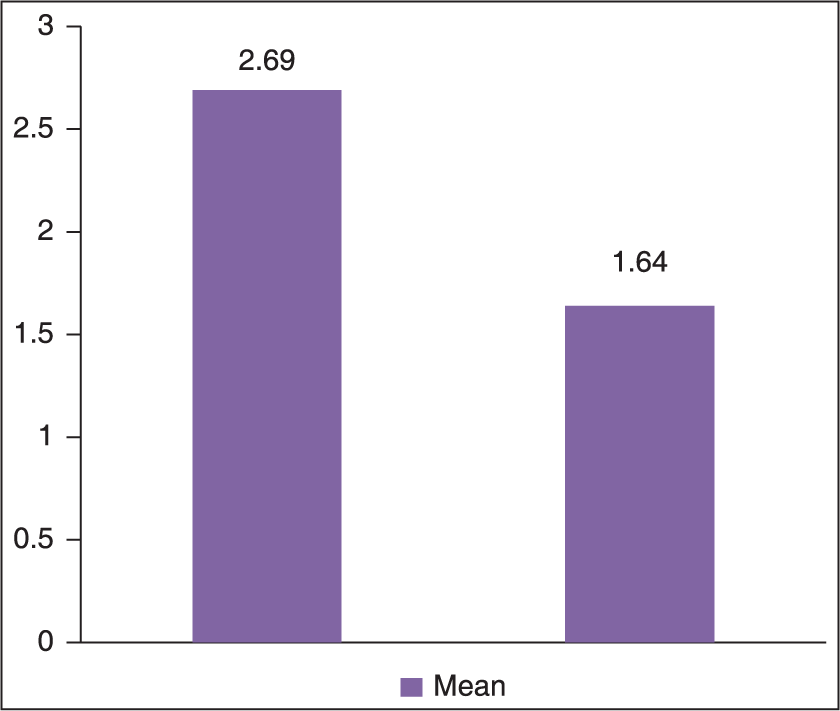
- Comparison of plaque accumulation mean scores between the maxillary hemiarches with conventional and self-ligation
Literature corroborates the findings of our study with the studies of Forsberg et al.[9] and Pellegrini et al.[6] Tukkahraman et al.,[18] however, found no significant differences in the numbers of microorganisms from teeth ligated with either elastomeric rings or steel ligature wires. Garcez et al.[8] showed a significant difference in the amount and composition of biofilm close to different types of brackets. They showed that there was a less supra-gingival biofilm on conventional brackets ligated with stainless steel ligature than on SLBs in in vitro conditions. van Gastel et al.[25] in their in vivo study, have also proved comparatively that bracket designs can have a significant impact on bacterial load and on periodontal parameters.
Our results from the plaque accumulation staining by the dye clearly indicated that around SL brackets there was less plaque accumulation and less biofilm formation as compared to the side where elastomeric ligation was done. This method of disclosing plaque deposits can also serve to be an important method of patient motivation while illustrating benefits of SL brackets to patients. Also, the microbiological analysis with bacterial culturing showed increased in CFUs per mm of the S. mutans on the side of ligation as compared to control half.
CONCLUSION
This study comprehensively observed that the conventional ligation with an elastomeric module s harbors more amount of plaque as compared to smart clip SL bracket system. This information should be an important parameter in choosing Bracket Systems for a more hygienic orthodontic therapy.
References
- Demineralization and remineralization around orthodontic appliances: An in vivo study. Am J Orthod Dentofacial Orthop. 1987;92:33-40.
- [Google Scholar]
- Spot on orthodontics! Pun intended: The impact of white spot lesions on 21st century orthodontics. APOS Trends Orthod. 2014;4:148-50.
- [Google Scholar]
- A posttreatment evaluation of direct bonding in orthodontics. Am J Orthod. 1977;71:173-89.
- [Google Scholar]
- Prevalence of white spot lesions in 19-year-olds: A study on untreated and orthodontically treated persons 5 years after treatment. Am J Orthod Dentofacial Orthop. 1989;96:423-7.
- [Google Scholar]
- Incidence of white spot formation aer bonding and banding. Am J Orthod. 1982;81:93-8.
- [Google Scholar]
- Plaque retention by self-ligating vs elastomeric orthodontic brackets: Quantitative comparison of oral bacteria and detection with adenosine triphosphate-driven bioluminescence. Am J Orthod Dentofacial Orthop. 2009;135:426.e1-9.
- [Google Scholar]
- Gingival condition associated with orthodontic treatment. Angle Orthod. 1972;42:26-34.
- [Google Scholar]
- Biofilm retention by 3 methods of ligation on orthodontic brackets: A microbiologic and optical coherence tomography analysis. Am J Orthod Dentofacial Orthop. 2011;140:e193-8.
- [Google Scholar]
- Ligature wires and elastomeric rings: Two methods of ligation, and their association with microbial colonization of Streptococcus mutans and lactobacilli. Eur J Orthod. 1991;13:416-20.
- [Google Scholar]
- Prevalence of carious white spots after orthodontic treatment with multibonded appliances. Eur J Orthod. 1986;8:229-34.
- [Google Scholar]
- In-vivo effects of fluoridated antiplaque dentifrice and bonding material on enamel demineralization adjacent to orthodontic appliances. Am J Orthod Dentofacial Orthop. 2006;130:357-63.
- [Google Scholar]
- Orthodontic appliances and enamel demineralization. Part 2. Prevention and treatment of lesions. Am J Orthod Dentofacial Orthop. 1988;94:123-8.
- [Google Scholar]
- Salivary Streptococcus mutans levels in patients with conventional and self-ligating brackets. Eur J Orthod. 2010;32:94-9.
- [Google Scholar]
- A clinical and radiographic study to evaluate the rate of retraction of maxillary canine using nickel-titanium closed coil spring with two different bracket systems. APOS Trends Orthod. 2014;4:169-77.
- [Google Scholar]
- Relative distribution of bacteria at clinically healthy and periodontally diseased sites in humans. J Clin Periodontol. 1978;5:115-32.
- [Google Scholar]
- Periodontal disease in pregnancy. I. Prevalence and severity. Acta Odontol Scand. 1963;21:533-51.
- [Google Scholar]
- Comparative cleansing efficiency of manual and power brushing. J Am Dent Assoc. 1962;65:26-9.
- [Google Scholar]
- Archwire ligation techniques, microbial colonization, and periodontal status in orthodontically treated patients. Angle Orthod. 2005;75:231-6.
- [Google Scholar]
- Periodontal condition of the mandibular anterior dentition in patients with conventional and self-ligating brackets. Orthod Craniofac Res. 2008;11:211-5.
- [Google Scholar]
- Bacterial colonization associated with fixed orthodontic appliances. A scanning electron microscopy study. Eur J Orthod. 2001;23:475-84.
- [Google Scholar]
- Periodontal and microbiologic evaluation of 2 methods of archwire ligation: Ligature wires and elastomeric rings. Am J Orthod Dentofacial Orthop. 2008;134:506-12.
- [Google Scholar]
- Effects of orthodontic attachments on the gingival health of permanent second molars. Am J Orthod Dentofacial Orthop. 1991;100:337-40.
- [Google Scholar]
- The effect of orthodontic treatment on the periodontium. Angle Orthod. 1974;44:127-34.
- [Google Scholar]
- Enamel demineralization with two forms of archwire ligation investigated using an in situ caries model — A pilot study. Eur J Orthod. 2009;31:542-6.
- [Google Scholar]
- Influence of bracket design on microbial and periodontal parameters in vivo. J Clin Periodontol. 2007;34:423-31.
- [Google Scholar]




