

Translate this page into:
Preliminary study of articulatory characteristics in open bite subjects revealed by 3T magnetic resonance imaging movies

-
Received: ,
Accepted: ,
How to cite this article: Ozawa E, Honda E, Tomizato H, Kurabayashi T, Nunthayanon K, Ohmori H, et al. Preliminary study of articulatory characteristics in open bite subjects revealed by 3T magnetic resonance imaging movies. APOS Trends Orthod 2021;11(1):14-22.
Abstract
Objectives:
Previous studies have reported that articulatory dysfunction accompanied by a certain type of malocclusion can be improved by orthodontic treatment. We developed a 3-T magnetic resonance imaging (MRI) movie method with tooth visualization that can display the dynamic movement of articulation without radiation exposure. To the best of our knowledge, there is currently no report on the possible differences in articulatory movement between subjects with a normal occlusion and those with malocclusion using the 3T MRI movie method. Thus, the objective of this study was to examine the articulatory difference between subjects with a normal occlusion and those with an open bite using an MRI movie.
Materials and Methods:
Twenty healthy adult females, ten with a normal occlusion and ten with an anterior open bite were recruited. The overbite of the open bite subjects was zero or smaller, and all of them exhibited a tongue-thrusting habit during swallowing. A turbo spin echo image with a contrast medium was used to visualize the anterior teeth, and articulatory movement during articulation of the vowel-consonant-vowel syllable (/asa/) was scanned. The difference in tongue movement between subjects with a normal occlusion and those with an open bite was compared by measuring seven variables. Moreover, the distance between the incisal edge and the tongue apex during articulation of /s/ and the speech duration were compared. Furthermore, frequency analysis on /s/ by fast Fourier transform power spectrum was performed.
Results:
The tongue apex of the open bite subjects moved more anteriorly than that of the normal subjects. However, there was no significant difference in the phonetic analysis between subjects with a normal occlusion and those with an open bite.
Conclusion:
The 3-T MRI movie was an efficient method to quantify articulatory tongue movements. Although there was a difference in tongue movement during swallowing between subjects with a normal occlusion and those with an open bite, the difference in the articulatory tongue movements was minimal, suggesting it could be a functional compensation.
Keywords
Magnetic resonance imaging
Motion pictures
Open bite
Articulation
Tongue-thrusting habit

INTRODUCTION
There are various types of malocclusions such as open bite, mandibular/maxillary protrusion, and crossbite that can cause articulatory disfunction. However, such disorders can be improved with orthodontic treatment.[1,2]
Analytical methods such as visual evaluation, electropalatography,[3] videofluorography,[4] cineradiography,[5] and computed tomography[6] can be used to evaluate the speech production process. The use of radiography and an intraoral appliance is accompanied by radiation exposure and interference with the natural movement of the tongue. In contrast, magnetic resonance imaging (MRI) is non-invasive and can exhibit the teeth and soft tissues using a contrast agent; a modified technique, such as an MRI movie, can delineate the dynamic movement of the organs and tissues.[7-12] This method has made it possible not only to observe the articulation but also to measure the relationship between the teeth and the tongue, which is currently unknown. Nunthayanon et al.[11] have reported the positional differences in the articulatory organs during pronunciation between Japanese and Thai females with a normal occlusion using an MRI movie. However, there are currently no reports on the effects of malocclusion on dynamic articulatory movement.
This study aimed to examine the temporal/positional difference in articulatory organs during pronunciation between subjects with a normal occlusion and those with an anterior open bite using an MRI movie. It was hypothesized that the tongue of the open bite would be located differently from the normal occlusion.
MATERIALS AND METHODS
Participants
Adult female patients with anterior open bite were recruited from a group of patients under 30 years of age who visited the Orthodontic Clinic at Tokyo Medical and Dental University (TMDU) Dental Hospital from 2013 to 2017. As the differences in the velopharyngeal structures between sexes are well-known,[13,14] only female patients were recruited.
Anterior open bite was defined as a vertical overlap at the incisal edges of anterior teeth having a zero or negative value.[15] Ten healthy females with normal occlusion with appropriate vertical overlap at the edge of the anterior teeth (control group) and ten females with anterior open bite (open bite group) voluntarily participated in this study. Written informed consent was obtained from the 20 participants before their participation in the study. All procedures performed in this experiment were a priori approved by the Ethics Committee (No. 934) of TMDU and complied with the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Preparation
Customized plates, facial markers, and medium gel were prepared before the MRI examination; the customized plates and facial markers are necessary to visualize the incisor teeth.[7,9,10] Both maxillary and mandibular impressions of all participants were made to obtain individualized plaster models. The maxillary and mandibular central incisors were covered with silicon putty (EXAFINE PUTTY TIYE, GC, Tokyo, Japan) to make space for the contrast medium gel, and a customized clear plate was fabricated using Biostar® (DURAN +, JM Ortho Corporation, Tokyo, Japan). The 0.5-inch thick individualized plate had two holes for removal of the excess gel containing ferric ammonium citrate (FAC) solution. The facial markers were fabricated from square plastic straws, composite resin (ESTELITE Σ QUICK, Tokuyama Dental Corporation, Tokyo, Japan), and 4 mg/mL FAC solution. FAC was used for obtaining the positive enhancement effect in the MRI.[7] The medium gel consisted of FAC, 14 mg sodium bicarbonate, 950 mg agar powder, and 1100 mg sugar in 10 mL of boiled water. All the materials were mixed and cooled until gelation.
MRI
A custom-made circuit was connected to a 3-Tesla (3T) MRI scanner (Magnetom Spectra, Siemens, Munich, Germany) with a head/neck coil and face markers. Three face markers were fixed to the forehead, tip of the nose, and jaw by adhesion tapes. First, the participant was asked to lie in a supine position with the head stabilized inside the head coil and then she was fitted with headphones to provide an auditory cue for synchronization of the participant’s pronunciation with scanning time. A programmed external trigger pulse was used to control the timing scan sequence and provide the acoustic cue, allowing the scan to be synchronized with pronunciation. A fiber-optic microphone (FOMRI, Phone-or, Or Yahuda, Israel) was placed in front of the participant’s lips to capture the pronunciation. The frequency characteristic of the microphone was between 30 Hz and 15 kHz. A connected digital recorder (PMD670, Marantz, Middlesex, UK) was used to record the pronunciation and external trigger pulse.[9]
Speech task
An external trigger pulse was fed to the MR scanner 16 times at 1500-ms intervals, and the participants were required to repeat the vowel-consonant-vowel (VCV) syllable (i.e., / asa/) 16 times in a synchronized manner in response to the auditory cue. The consonant /s/ was chosen because a previous study showed that the velopharyngeal structures were not affected by the difference in the body position.[9] The participants were asked to breathe between repetitions of the VCV articulation and return the tongue and mandible to the resting position at the beginning and end of each pronunciation. Each participant fully exercised the pronunciation outside the MR gantry before imaging, and recording were conducted in the room without noise.
Dental MR image acquisition
Both the maxillary and mandibular trays with the medium gel were set in the participant’s mouth during acquisition of dental MR images. A turbo spin echo (TSE) sequence with a repetition time (TR) of 500 ms, an echo time (TE) of 20 ms, and a flip angle (FA) of 150 degrees were used for high-resolution static imaging. The image had a pixel size of 0.5 × 0.5 mm, slice thickness of 4 mm, and a field of view (FOV) of 256 × 256 mm. The time required for the static image was approximately 2 min.
MR movie image acquisition
Image acquisition consisted of a gradient-echo (GRE) sequence, fast low-angle shot with segmented cine, and a parallel imaging technique by GRAPPA. The mid-sagittal plane was imaged using the following parameters: a TR of 22.5 ms, a TE of 2.07 ms, an FA of 12 degrees, an FOV of 256 × 256 mm, a pixel size of 1 × 2 mm, a slice thickness of 4 mm, and an acceleration factor of 2. The repeat count of pronunciation was 16, and total acquisition time was 24 s.
Tooth superimposition
The pixel size ratio between the GRE and TSE sequences was set at 2:1 for height and 4:1 for width to eliminate error from linear interpolation during superimposition. Superimposition was performed using a customized software (Image Rugle 2009, Medic Engineering Inc., Kyoto, Japan). To superimpose the maxillary incisors in the dental MRI and the oral tissue image, three landmarks on the forehead, tip of the nose, and chin were used. After the superimposition, a photo-editing software (Adobe Photoshop CS6 Adobe, San Jose, CA, USA) was used to extract the maxillary tooth boundary. Next, the soft-tissue image was again superimposed on the maxillary tooth boundary until the soft-tissue MR image revealed the maxillary tooth. For the maxillary incisors, the chin marker and mandibular margin were used as landmarks, and an identical procedure was performed. Finally, a soft-tissue MR image revealing the maxillary and mandibular anterior teeth was obtained. The superimposition procedure has been explained in detail elsewhere.[8-10]
Area of interest and measurements
Four images obtained at the rest phase (100 ms before pronunciation; Stage A), the first vowel (the middle of the first vowel /a/; Stage B), and consonant phases (the middle of the consonant /s/; Stage C) were chosen for analysis [Figure 1]. The middle points were determined using MR images, voice data, and a spectrogram. Seven linear variables were defined on the images [Figure 2]. All parameters and definitions are shown in [Table 1]. The distance from the incisal edge to the tip of the tongue at Stage C was measured on each image with the superimposed teeth [Figure 3].
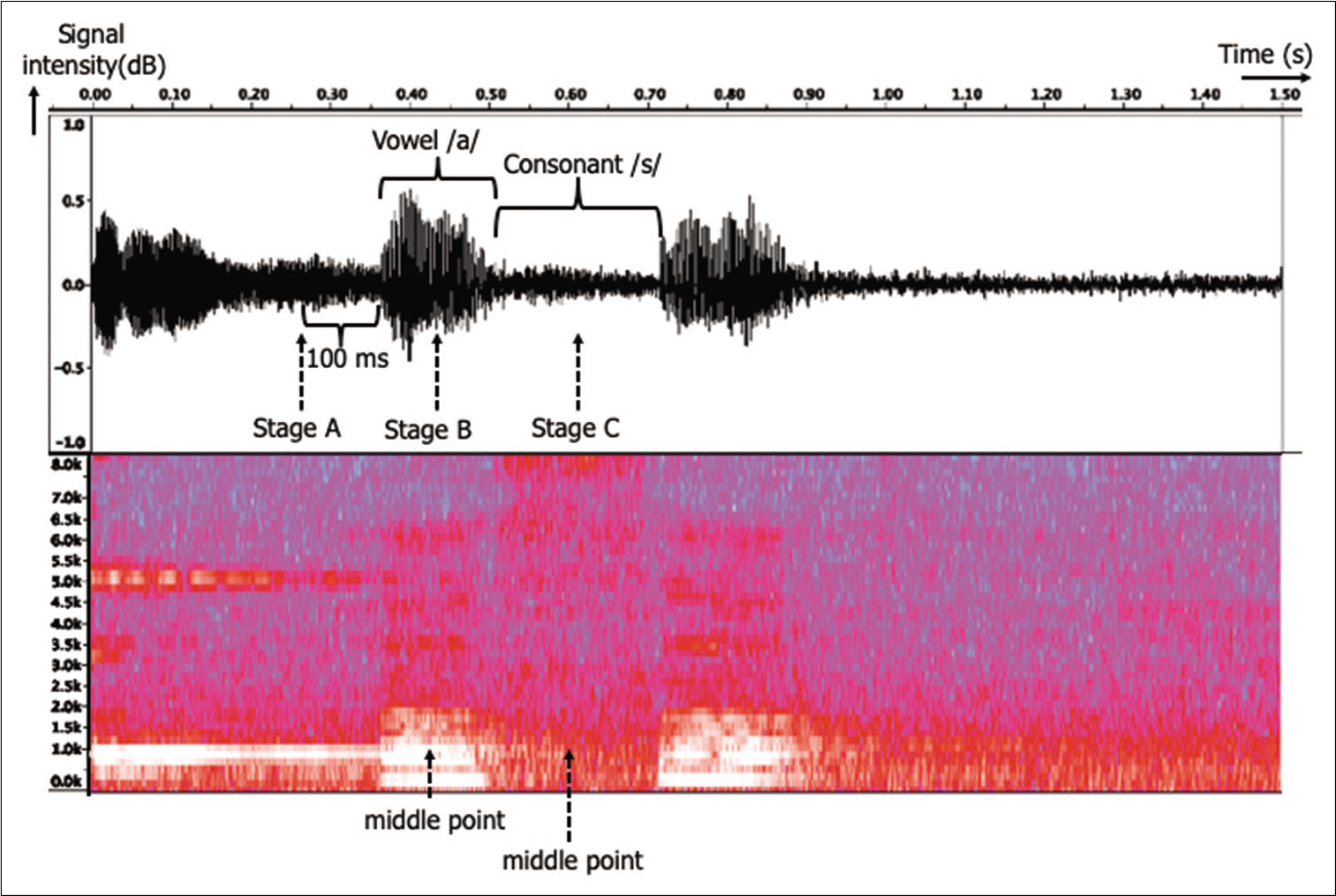
- A representative sound wave, timing chart, and spectrogram. At rest (Stage A), the first vowel (Stage B), and the middle of production of the consonant (Stage C) were determined using magnetic resonance imaging images, voice data, and spectrogram; the middle points were then analyzed.

- Two lines parallel and vertical to the hard plate were used as the standard lines. Seven linear measurements are shown. TTHH: Tongue tip–hard palate height, THH: Tongue-hard palate height, RH: Retroglossal height, TD: Tongue depth, TPD: Tongue tip–posterior pharyngeal wall depth, RD: Retroglossal depth, HPD: Hard palate depth, VD: Velopharyngeal depth.
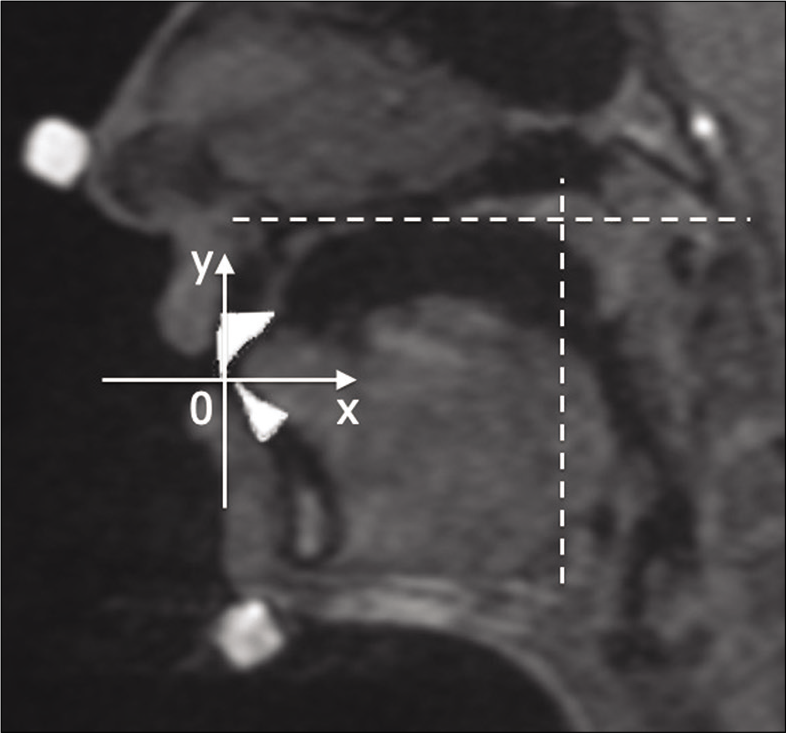
- Two lines parallel and vertical to the hard plate were used as the standard lines. The X-axis and Y-axis were set with the maxillary anterior incision as 0.
| Linear measurement | Abbreviation | Definition |
|---|---|---|
| Length involved with the tongue on the plane vertical to the hard palate | ||
| Tongue tip–hard palate height | TTHH | Distance between the tongue tip and hard palate |
| Tongue–hard palate height | THH | Distance between the top of the tongue and the hard palate |
| Retroglossal height | RH | Distance between the most posterior margin of the tongue and the hard palate |
| Length involved with the tongue on the plane parallel to the hard palate | ||
| Tongue depth | TD | Distance between the tongue tip and the posterior margin of the tongue |
| Tongue tip–posterior pharyngeal wall depth | TPD | Distance between the tongue tip and the posterior pharyngeal wall |
| Retroglossal depth | RD | Distance between the most posterior margin of the tongue and the hard palate |
| Length involved with tissue other than the tongue on the plane parallel to the hard palate | ||
| Velopharyngeal depth | VD | Distance between the PNS and the posterior pharyngeal wall |
Sound data manipulation
The recorded sound data were manipulated by Audacity (open source software) and SoundEngine (Code Helium, Hokkaido, Japan) that allowed the time of articulation and sound wave to be recorded. The noise included in sound data was eliminated; and then, the data were digitized at a sampling rate of 44.1 kHz with 16-bit quantization by Audacity. The sound stage was determined by the manipulated sound data by SoundEngine. The speech duration of each participant was measured and compared between the control and open bite groups [Figure 1].
Phonetic analysis
Three blinded orthodontists judged the sound data using a grading scale that ranged from 1 to 5. The scales were ranked as follows: One = absolutely open bite group, 2 = probably open bite group, 3 = uncertain, 4 = probably control group, and 5 = absolutely control group. Then, phonetic analysis was performed for the /a/ and /s/. The subjects were the participants judged as four or five were chosen from the control group and judged as one or two were chosen from the open bite group.
Statistical analysis
Each image was measured 3 times over 5 days. A single examiner (EO) performed the measurements to avoid inter-observer error. Intraobserver reliability was assessed by intraclass correlation coefficients (ICC). Seven linear variables were based on Stage A of each subject in the control group and open bite group. Three ratios of Stage A/Stage A, Stage B/Stage A, and Stage C/Stage A were set.
The ratios of each stage were used to eliminate the difference in the amplitude. Statistical analyses were performed using the analysis of variance (ANOVA), multiple comparisons when significant differences were determined by ANOVA. Welch’s test was conducted for phonetic analysis, and significance level was set at P < 0.05. The measurement errors determined by ICC were small (range: P < 0.05), and the measurements were reproducible.
RESULTS
Description of the sample population
The mean age of participants in the control group was 27.5 ± 2.5 (mean ± standard deviation) years and that of the open bite group was 23.6 ± 4.6 years. The mean height in the control group was 159.2 ± 5.2 cm and that of the open bite group was 157.2 ± 5.2 cm. The mean weight in the control group was 47.0 ± 3.0 kg and that of the open bite group was 47.8 ± 9.2 kg. The mean of body mass index in the control group was 18.5 ± 0.7 kg/m2 and that of the open bite group was 19.3 ± 2.4 kg/m2. The mean of overjet in the control group was 2.4 ± 1.1 mm and that of the open bite group was 3.8 ± 3.8 mm. The mean of overbite in the control group was 2.2 ± 0.8e mm and that of the open bite group was –2.6 ± 1.1 mm. Age and overbite were significantly different between the two groups, whereas height, weight, body mass index, and overjet were not. All patients in the open bite group showed tongue thrust, while none in the control group had such a habit.
Difference in the articulatory lingual movement
MR movies of the representative participants in the control [Figure 4a] and open bite groups [Figure 4b, Videos 1 and 2]. The maxillary and mandibular incisors did not contact during rest and pronouncing the target syllable in both groups. Tongue thrust, a prominent habit in the open bite participants, was recognized in the movie. During the pronunciation of /s/, the tongue tip was in contact with the lingual surfaces of maxillary anterior teeth in the control participants, whereas the tongue was caught between the incisors of both jaws and was protruded in the open bite participants. Otherwise, no significantly different findings were observed.
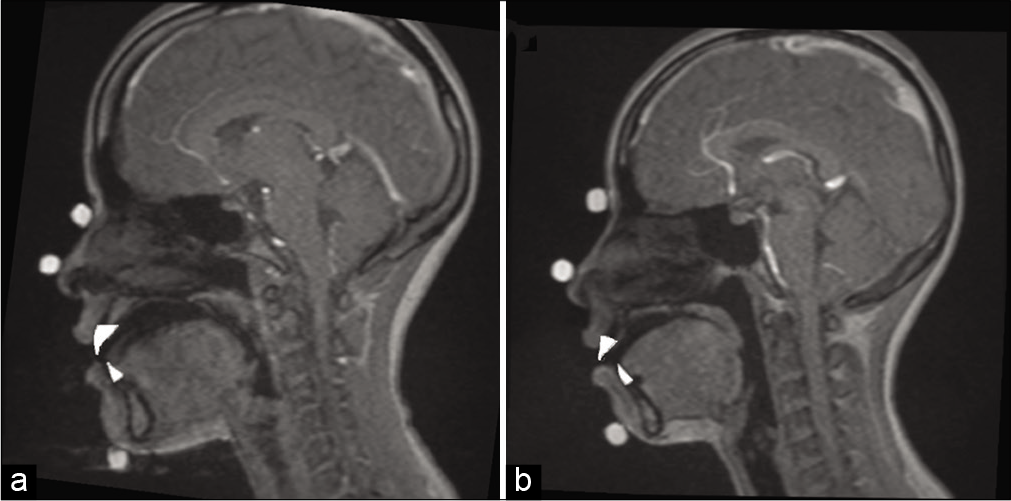
- Snapshots of magnetic resonance imaging movie-superimposed teeth of representative subjects in the control (a) and open bite groups (b).
Linear measurements
Seven linear measurements at each stage were compared between the two groups [Table 2]. There were no significant differences in all the parameters between the control and open bite groups.
| Linear measurements | Stage A | Stage B | Stage C | |||
|---|---|---|---|---|---|---|
| Control | Open bite | Control | Open bite | Control | Open bite | |
| TTHH | 28.2±2.7 | 30.0±3.6 | 33.0±4.4 | 35.9±2.3 | 27.6±3.0 | 27.3±2.1 |
| THH | 9.2±23.0 | 8.9±3.3 | 12.8±3.2 | 13.4±2.6 | 11.1±1.4 | 12.7±3.2 |
| RH | 32.2±32.5 | 33.6±4.7 | 33.0±2.7 | 36.3±5.1 | 34.1±6.2 | 34.5±3.6 |
| TD | 64.0±3.9 | 64.4±7.3 | 64.9±4.4 | 64.9±6.4 | 65.3±5.1 | 67.8±7.2 |
| TPD | 74.5±5.4 | 76.2±5.5 | 72.2±5.3 | 72.6±6.6 | 75.8±4.9 | 80.3±5.9 |
| RD | 9.8±2.7 | 10.0±2.5 | 5.7±1.8 | 6.7±1.6 | 8.0±2.2 | 10.1±2.2 |
| VD | 35.1±3.0 | 35.0±4.0 | 34.0±3.2 | 34.4±4.2 | 34.2±2.7 | 34.7±4.6 |
Means and standard deviations are presented. The number of subjects in each group is 10. TTHH: Tongue tip–hard palate height, THH: Tongue–hard palate height, RH: Retroglossal height, TD: Tongue depth, TPD: Tongue tip–posterior pharyngeal wall depth, RD: Retroglossal depth; VD: Velopharyngeal depth
[Table 3] showed the ratios of each stage based on stage A. In the control group, there was a significant difference between the ratios of Stage A/Stage A and Stage B/Stage A in TTHH, THH, and RD. Furthermore, there was a significant difference between the ratios of Stage A/Stage A and Stage C/ Stage A in THH. In open bite group, there were significant differences in all the same items. Further, there was no significant difference between the ratios of Stage C/Stage A in the control group and that in the open bite group.
| Linear measurements | Stage A/Stage A | Stage B/Stage A | Stage C/Stage A | |||
|---|---|---|---|---|---|---|
| Control group | Open bite group | Control group | Open bite group | Control group | Open bite group | |
| TTHH | 1.0 | 1.0 | 1.2±0.15* | 1.2±0.12* | 1.0±0.11 | 0.98±0.09 |
| THH | 1.0 | 1.0 | 1.5±0.32* | 1.5±0.49* | 1.3±0.33* | 1.4±0.57* |
| RH | 1.0 | 1.0 | 1.0±0.07 | 1.0±0.19 | 1.1±0.17 | 1.0±0.15 |
| TD | 1.0 | 1.0 | 1.0±0.06 | 1.0±0.09 | 1.0±0.09 | 1.0±0.10 |
| TPD | 1.0 | 1.0 | 0.97±0.06 | 0.97±0.05 | 1.0±0.07 | 1.0±0.04 |
| RD | 1.0 | 1.0 | 0.61±0.25* | 0.74±0.35* | 0.87±0.25 | 1.1±0.37 |
| VD | 1.0 | 1.0 | 0.97±0.03 | 0.97±0.02 | 0.97±0.02 | 0.97±0.04 |
TTHH: Tongue tip–hard palate height, THH: Tongue–hard palate height, RH: Retroglossal height, TD: Tongue depth, TPD: Tongue tip–posterior pharyngeal wall depth, RD: Retroglossal depth, VD: Velopharyngeal depth. *P<0.05
Speech duration in normal occlusion and open bite
[Table 4] shows representative data on speech duration for the control and open bite groups. There was no significant difference in all pronunciation durations between groups, but individual differences were large irrespective of the occlusion status. Some participants pronounced /a/ longer than /s/, but others pronounced it shorter. There was no significant difference in the ratio of the /a/ to /s/ duration between groups.
| Sounds | Control (n=10) | Open bite (n=10) | Probability |
|---|---|---|---|
| First vowel (ms) | 182.6±41.9 | 151.8±25.4 | NS |
| Consonant (ms) | 149.0±37.0 | 158.5±26.7 | NS |
| Second vowel (ms) | 180.0±42.3 | 152.6±26.5 | NS |
| Consonant/first vowel (ms) | 0.9±0.3 | 1.1±0.2 | NS |
Means and standard deviations are presented. N: Not significant
Difference in tongue position during the pronunciation of /s/
Based on the maxillary incisal edge, the tongue was measured using a line parallel to the hard palate as the X-axis and a line perpendicular to the hard palate as the Y-axis. It was revealed that the tongue tip for the open bite group was located more antero-inferior to the anterior tooth edge than that for the normal occlusion group [Figure 5].
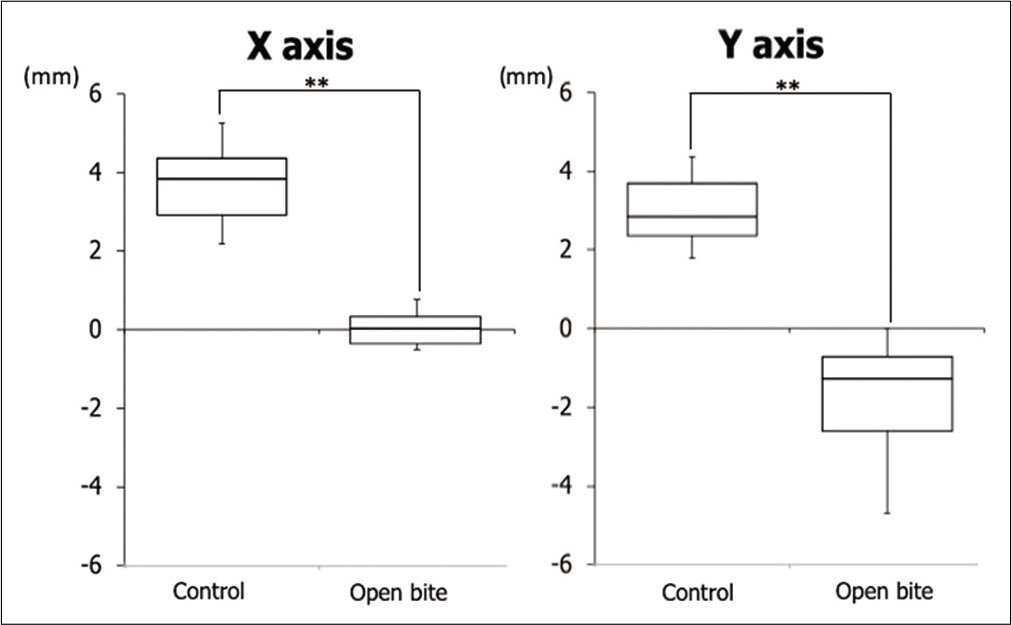
- Tongue tip location based on the maxillary incisal edge. A line parallel to the hard palate is represented by the X-axis and a line vertical to the hard palate is represented by the Y-axis **P<0.01.
Phonetic analysis of /a/ and /s/
In all the sound data, only three cases that each datum was pronounced by a participant with normal occlusion were correctly judged by the three orthodontists. As for open bite cases, three cases were correctly judged. The other cases were judged as false or unknown [Figure 6]. There was no significant difference in the phonetic analysis from the first (F1) to the fourth formant frequency (F4) of /a/ and /s/ between the control and open bite groups. In contrast, there was a significant difference in the transition part from /a/ to /s/ between the two groups [Figure 7].

- Discriminability between the control group and open bite group subjects using a five-grade evaluation.

- Average phonetic analysis of the transition part from /a/ to /s/ on F4 in normal group and open bite group.
DISCUSSION
Tongue position during the pronunciation of /s/
MR movies enabled the evaluation of the positional relationship between the anterior teeth and tongue during pronunciation in control and open bite participants. Many methods have been used for observation during pronunciation, and almost all have used radiographs.[16] Radiographic investigation of the relationship between the tongue and teeth has not been performed for pronunciation in open bite participants. To the best of our knowledge, this is the first MRI study to evaluate the articulatory difference between the participants with open bite and those with normal occlusion. The MR movie image showed that the tongue body in open bite participant was located at the same position and the tongue tip was located more antero-inferior when compared with normal occlusion participant during the pronunciation of /s/. By MRI movie, it is possible to observe the state of pronunciation several times before and after oral myofunctional therapy (MFT) in children and adults. It is said that the anterior tongue position at rest may greater impact on the tooth position rather than the tongue pressure during thrusting.[17] MFT is a therapy not only to correct tongue thrust habit but also to correct tongue position. It starts by muscle training to rest tongue in its normal superior position. MFT in childhood is effective in breaking tongue habits,[18] and it is meaningful to take the movie repeatedly. The evaluation of other pronunciations and swallowing with a tongue habit using MR movies is an a topic for future research.
Difference in pronunciation between normal occlusion and open bite participants
In this study, there were some significant differences in position of tongue tip and the value of F4 in phonetic analysis. However, there was no significant difference, which was actually expected, in the position of tongue body during the pronunciation of /s/ between the normal occlusion and open bite groups. Therefore, the hypothesis was rejected that the tongue body for the open bite group is located more anteriorly than that for the normal occlusion group.
Although an open bite can affect pronunciation, orthodontists could not correctly determine whether the syllable of /asa/ is pronounced correctly or not in participants with and without open bite. In contrast, in phonetic analysis, there could be a significant difference between the two participants. In general, there was no significant difference in phonetic analysis of /a/ and /s/ alone, but was observed during the transition period between sound /a/ and sound /s/ in /asa/. It is assumed that a word is judged by the transition portion of a sound of the character.
In this study, there was no significant difference between the normal occlusion and open bite participants. It might be because most participants (i.e., 14 participants) were not correctly judged by listening. In three normal participants and three open bite participants, phonetic analysis showed an objective difference between the two groups. Moreover, the frequency of open bite was higher than that of normal occlusion. We are planning to clarify the reason in future studies. Nonetheless, the 3T MRI movie method is able to observe the change in pronunciation during orthodontic treatment.
Application of findings in the treatment of tongue thrust
Harmony between the teeth and peri-oral muscles is important to maintain proper occlusion, proper occlusal force, and dentition.[19,20] It is also known that the muscles around the mouth influence craniofacial growth and development.[21] Recently, the relationship between sleep apnea syndrome and craniofacial growth and development of dentition in children has been reported.[22,23] Today, MFT, which is performed for muscle training, is said to be useful for open bite cases.[24,25] Furthermore, it is reported that tongue thrust is the cause of malocclusion,[17] and a significant correlation with mouth breathing is also reported.[26] Tongue thrust interferes with orthodontic treatment and causes malocclusion of the dentition after orthodontic treatment.[27,28] Moreover, tongue control is also important in orthodontic treatment; hence, its objective analysis is important. MR movies are suitable for the evaluation of tongue movement. According to a study of patients with orthodontic appliances,[29] it is difficult to analyze the state during orthodontic treatment using MR movies. However, to perform an MR movie before, during, and after MFT will be meaningful to improve patient motivation.
Study limitation
Although the sample size in the previous studies of analysis of tongue habits with MRI was the same,[30,31] the sample size was small (i.e., 10 each). The mean age was significantly different in the two groups – the control and open bite groups. There is a study that compared the tongue habits between children and young adults,[32] but there was no comparative study between those in their early or late 20s. In addition, there are no anatomical or physiological differences between them regarding growth.[17] Therefore, the significant difference in age does not affect the results of this study.
In this study, the participants comprised only females because the differences in velopharyngeal structures with regard to sex are well-known.[13,14] Since no reports have discussed the differences in tongue habits between male and female participants, future research on this topic is necessary.
CONCLUSION
A 3-T MRI movie is an efficient method for observing tongue movements. Using this method, we found that there are differences in tongue movements during pronunciation between those with a normal occlusion and those with an open bite with tongue thrust. The tongue movement of an open bite patient with a tongue thrust adversely affects occlusion and the retention of the dentition; however, it has little influence on pronunciation.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Japan Society for Promotion Science [Grant numbers 15K11361 and 18K09761].
Conflicts of interest
There are no conflicts of interest.
Video available on:
References
- Articulation and oromyofunctional behavior in children seeking orthodontic treatment. Oral Dis. 2015;21:483-92.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of a rapid expander on speech articulation. Am J Orthod Dentofacial Orthop. 2011;140:e67-75.
- [CrossRef] [PubMed] [Google Scholar]
- The application of electropalatography (EPG) to the remediation of speech disorders in school-aged children and young adults. Eur J Disord Commun. 1995;30:264-77.
- [CrossRef] [PubMed] [Google Scholar]
- Premature infant swallowing: Patterns of tongue-soft palate coordination based upon videofluoroscopy. Infant Behav Dev. 2010;33:209-18.
- [CrossRef] [PubMed] [Google Scholar]
- Cineradiography of monkey lip-smacking reveals putative precursors of speech dynamics. Curr Biol. 2012;22:1176-82.
- [CrossRef] [PubMed] [Google Scholar]
- Vocal tract area function estimation from midsagittal dimensions with CT scans and a vocal tract cast: Modeling the transition with two sets of coefficients. J Speech Hear Res. 1992;35:53-67.
- [CrossRef] [PubMed] [Google Scholar]
- Application of MRI movie for observation of articulatory movement during a fricative/s/and a plosive/t/. Angle Orthod. 2011;81:237-44.
- [CrossRef] [PubMed] [Google Scholar]
- A pilot study on characterization of articulatory movements during fricative/s/sound in an anterior open-bite subject: A tooth-visualized 3-T magnetic resonance imaging video evaluation. J World Fed Orthod. 2015;4:71-7.
- [CrossRef] [Google Scholar]
- Differential articulatory movements during Japanese/s/and /t/as revealed by MR image sequences with tooth visualization. Arch Oral Biol. 2012;57:749-59.
- [CrossRef] [PubMed] [Google Scholar]
- Use of an advanced 3-T MRI movie to investigate articulation. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015;119:684-94.
- [CrossRef] [PubMed] [Google Scholar]
- Differences in velopharyngeal structure during speech among Asians revealed by 3-Tesla magnetic resonance imaging movie mode. Biomed Res Int. 2015;2015:126264.
- [CrossRef] [PubMed] [Google Scholar]
- Principles of the magnetic resonance imaging movie method for articulatory movement. Oral Radiol. 2019;35:91-100.
- [CrossRef] [PubMed] [Google Scholar]
- Sexual dimorphism of the levator veli palatini muscle: An imaging study. Cleft Palate Craniofac J. 2014;51:544-52.
- [CrossRef] [PubMed] [Google Scholar]
- Three-dimensional magnetic resonance imaging of velopharyngeal structures. J Speech Lang Hear Res. 2011;54:1538-45.
- [CrossRef] [Google Scholar]
- The interception of the open bite in the early growth period. Angle Orthod. 1971;41:24-44.
- [Google Scholar]
- Articulatory movements during vowels in speakers with dysarthria and healthy controls. J Speech Lang Hear Res. 2008;51:596-611.
- [CrossRef] [Google Scholar]
- The effect of orofacial myofunctional treatment in children with anterior open bite and tongue dysfunction: A pilot study. Eur J Orthod. 2016;38:227-34.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of the relationship between the anterior component of occlusal force and postretention crowding. Am J Orthod Dentofacial Orthop. 2002;122:366-70.
- [CrossRef] [PubMed] [Google Scholar]
- Patterns of dental crowding in the lower arch and contributing factors. A statistical study. Angle Orthod. 2007;77:303-10.
- [CrossRef] [Google Scholar]
- Effects of food processing on masticatory strain and craniofacial growth in a retrognathic face. J Hum Evol. 2004;46:655-77.
- [CrossRef] [PubMed] [Google Scholar]
- Development of craniofacial and dental arch morphology in relation to sleep disordered breathing from 4 to 12 years. Effects of adenotonsillar surgery. Int J Pediatr Otorhinolaryngol. 2010;74:137-43.
- [CrossRef] [PubMed] [Google Scholar]
- Associations between sleep-disordered breathing symptoms and facial and dental morphometry, assessed with screening examinations. Am J Orthod Dentofacial Orthop. 2011;140:762-70.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontic treatment and masticatory muscle exercises to correct a Class I open bite in an adult patient. Am J Orthod Dentofacial Orthop. 2003;124:91-8.
- [CrossRef] [Google Scholar]
- Relapse of anterior open bites treated with orthodontic appliances with and without orofacial myofunctional therapy. Am J Orthod Dentofacial Orthop. 2010;137:605-14.
- [CrossRef] [PubMed] [Google Scholar]
- Stability of treatment for anterior open-bite malocclusion: A meta-analysis. Am J Orthod Dentofacial Orthop. 2011;139:154-69.
- [CrossRef] [PubMed] [Google Scholar]
- Is tongue thrust that develops during orthodontic treatment an unrecognized potential road block? J Indian Soc Pedod Prev Dent. 2006;24:80-3.
- [CrossRef] [PubMed] [Google Scholar]
- Causal relationship between malocclusion and oral muscles dysfunction: A model of approach. Eur J Paediatr Dent. 2012;13:321-3.
- [Google Scholar]
- Influence of orthodontic appliance-derived artifacts on 3-T MRI movies. Prog Orthod. 2018;19:7.
- [CrossRef] [PubMed] [Google Scholar]
- Initial effects on the tongue crib on tongue movements during deglutition: A cine-magnetic resonance imaging study. Angle Orthod. 2006;76:400-5.
- [Google Scholar]
- Visualization and quantification of tongue movement during articulation: Is ultrasound a valid alternative to magnetic resonance imaging? J Craniomaxillofac Surg. 2018;46:1924-33.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of masticatory performance and tongue pressure between children and young adults. Clin Exp Dent Res. 2018;4:52-8.
- [CrossRef] [PubMed] [Google Scholar]




