

Translate this page into:
Skeletal class III camouflage by mandibular incisor extraction: A case report
Address for Correspondence: Dr. Janardhanan Kumaresan, Department of Orthodontics and Dentofacial Orthopedics, K.S.R Institute of Dental science and research, Tiruchengode, Namakkal district, Tamil Nadu - 637 215, India. E-mail: kumaresan.janardhanan@gmail.com
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Treatment planning in orthodontics plays a key role in determining the successful treatment of any kind of malocclusion. Skeletal class III malocclusions are generally difficult to treat because of the complex nature of the skeletal and dental manifestations they produce. Mild to moderate skeletal class III malocclusions sometimes have an acceptable facial profile where orthodontic camouflage is possible. In this case report, camouflage of a mild skeletal class III is done by the extraction of a single mandibular incisor, which helped in maintaining the profile of the patient and also in the correction of crowding in the mandibular anterior region.
Keywords
Facial profile
Lower incisor extraction
Skeletal Class III

INTRODUCTION
Any deviation from ideal occlusion can be defined as malocclusion. Skeletal class III malocclusions are characterized by a prognathic mandible/retrognathic maxilla or a combination of both. According to James L Ackerman, the severity of the skeletal discrepancy is the key factor in the treatment planning of such cases.[1] Severe class III cases warrants orthognathic surgery, and moderate cases can be attempted with extraction treatment, whereas a mild skeletal class III with a dental class I malocclusion and mild crowding will be a borderline case which requires a careful treatment planning.[2,3] Because in such cases, when the soft tissue profile favors non-extraction, the purpose of orthodontic treatment would be to just resolve the crowding and align the arches. An attempt to camouflage the skeletal class III by maxillary 2nd and mandibular 1st extractions in such cases would result in worsening of the class III profile type. Those are the situations, which favors the extraction of a mandibular incisor, particularly if the discrepancy is in the lower anterior region.[2,3] A diagnostic set up is strongly recommended with this kind of treatment approach.[4-6]
Indications of mandibular incisor extractions
Jackson in 1905 described a case in which two lower incisors were extracted at different times to relieve mandibular crowding.[7] Various authors have proposed the indications and contra indications of mandibular incisor extractions.[2,8-10] The indications include
Angle’s class I malocclusion with severe anterior tooth size discrepancy and excessive mesiodistal width of the mandibular incisors,
Class I malocclusion with normal maxillary dentition adequate posterior inter-cuspation and lower anterior crowding with lack of space approximately for one mandibular incisor,
Dental class I malocclusion with anterior cross bites due to crowding and protrusion of the lower incisors, adequate posterior inter-cuspation, acceptable facial esthetics,
Dental class I malocclusion superimposed on a skeletal class III base with lower anterior crowding, etc.
Advantages and disadvantages of mandibular incisor extractions
Mandibular incisor extractions have many advantages over premolar extractions. When the patient’s soft tissue profile is not favourable for extraction of premolars, then mandibular incisor extraction is the best choice to maintain the profile.[8] Moreover, it reduces the treatment time, and the results achieved with mandibular incisor extractions are more stable when compared with premolar extraction since there is only a mild alteration of the inter-canine width.[11-14]
Mandibular incisor extraction also has some disadvantages. When the Bolton’s discrepancy is too less, it may sometimes result in increased overjet at the end of mandibular incisor extraction therapy. There is also a probability for torque loss of the lower incisors during the closure of the extraction space. The coincidence of maxillary and mandibular midline after mandibular incisor extraction is impossible. Finally, the interproximal papillae may be sacrificed, which may lead to the development of open gingival embrasures or black triangle.[4,6,11,15]
According to Owen,[15] patients who are suitable for single lower incisor extractions usually fit the following diagnostic pattern: Mild skeletal class III with class I molar relationships, moderately crowded mandibular incisors, mild or no crowding in the maxillary arch, acceptable soft tissue profile, minimal to moderate growth potential, and missing or peg-shaped maxillary lateral incisor.
CASE REPORT
Diagnosis
A 19-year-old female presented with a chief complaint of irregularly placed teeth in the upper and lower front tooth region. Clinical examination revealed competent lips and a straight profile [Figure 1]. On smiling, she displayed 100% of her incisors. There was unilateral anterior cross bite in relation to 21 and 31 and 22 and 32 [Figure 2]. The molar and canine relationships were class I. Model analysis revealed crowding of 5 mm in the upper arch and 7 mm in the lower arch. The patient had a 30% overbite and 1 mm overjet, with the lower midline shifted 2 mm to the right. Good oral hygiene was evident although slight gingival recession was found in the areas of the lower incisors and cuspid. Cephalometric analysis was done using Dolphin Imaging and Management solutions (Patterson dental supply, version 11.0, United States), which revealed the presence of skeletal class III pattern [Figure 3]. Pre treatment orthopantomogram displayed sufficient amount of alveolar bone and no signs of bone loss [Figure 4]. Model analysis showed Bolton’s discrepancy of 2.6 mm of excess in the mandibular anterior region.
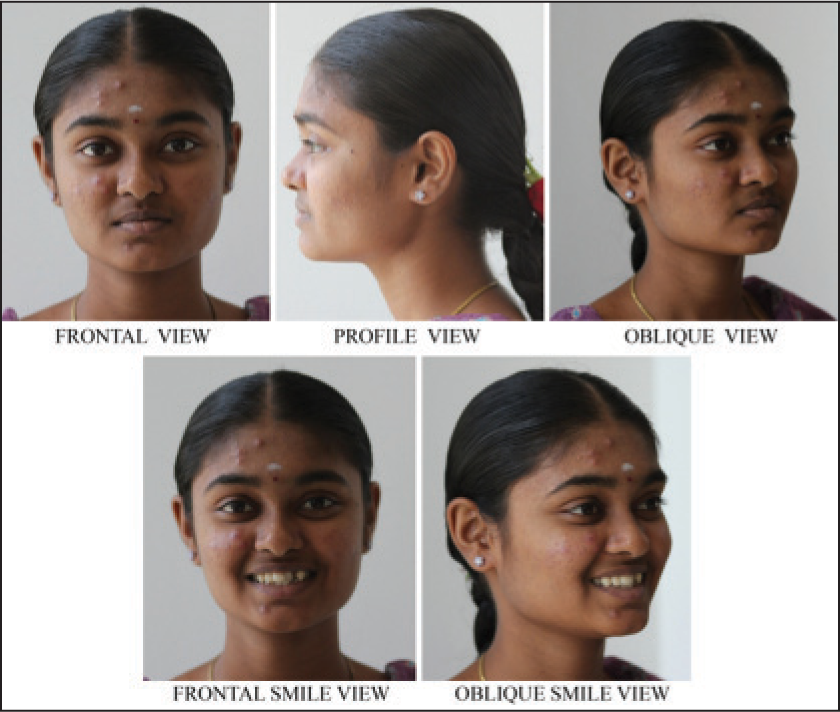
- Pre-treatment extra-oral photographs
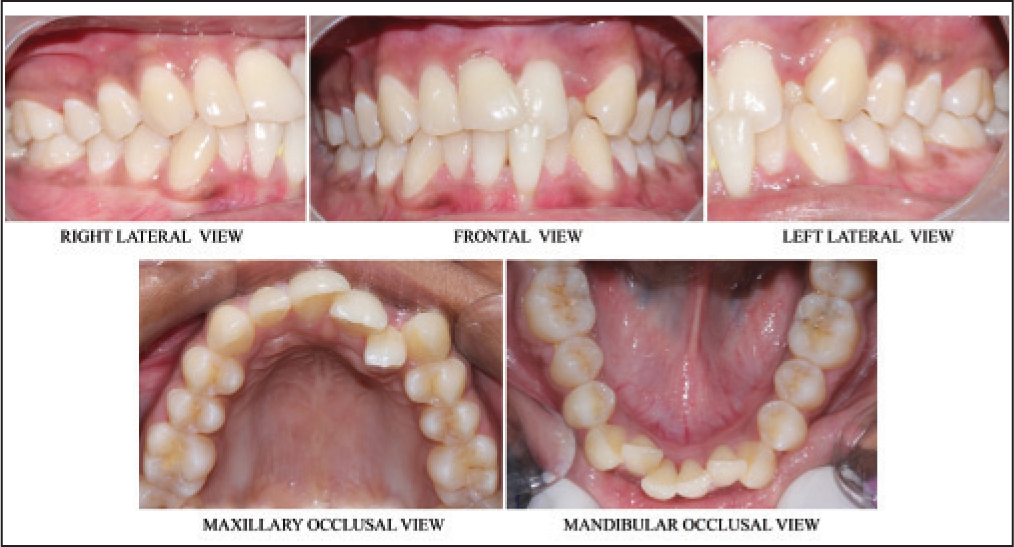
- Pre-treatment intra-oral photographs

- Pre-treatment lateral cephalogram
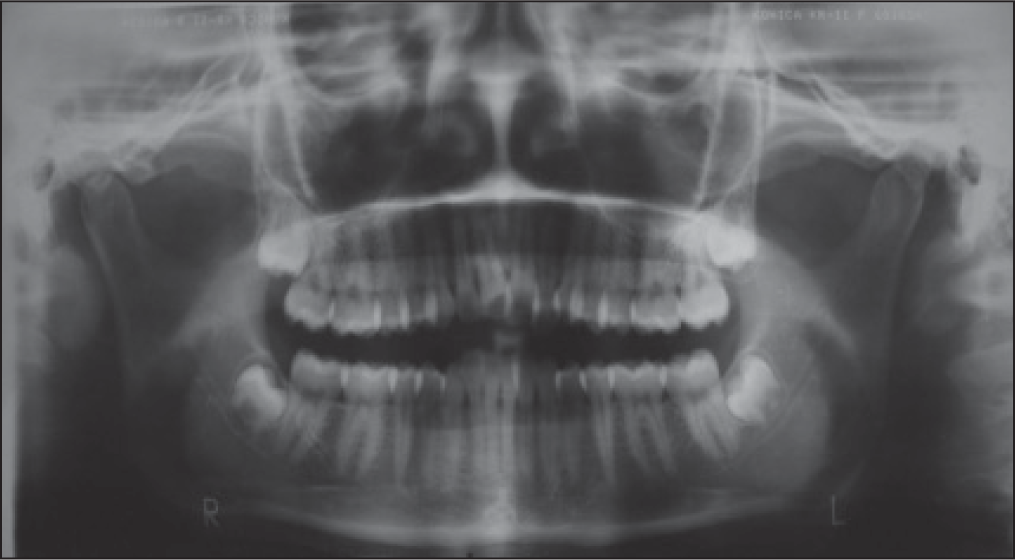
- Pre-treatment OPG
Treatment objectives
Correction of anterior cross bite
Relieving of upper and lower anterior crowding
Maintenance of class I canine and molar relation
To achieve ideal overjet/overbite
Maintenance of good profile
Treatment alternatives
In this case, the mandibular incisor crowding could have been treated with proximal stripping alone in the lower arch if the tooth size discrepancy in the lower arch was less than 2 mm. Since the tooth size discrepancy was more than 2.5 mm, this option was eliminated. The other treatment option would have been extraction of all first premolars to correct the maxillary and mandibular anterior crowding. But this would have resulted in surplus space in the arches, and continuing retraction could worsen the profile making it more concave. A non-extraction treatment plan could have been attempted using a self-ligating appliance, but this could result in excessive proclination of both maxillary and mandibular.
Treatment plan
In this case, even though there was a crowding of the maxillary and mandibular, the profile of the patient was straight and was highly favorable for non-extraction kind of treatment. Maxillary space requirement was minimal and slight proclination and arch development was sufficient in achieving good result. Mandibular incisor extraction was planned to maintain the straight profile and to relieve the mandibular anterior crowding since there was a tooth size arch length discrepancy of more than 5 mm in the mandibular arch.
Treatment progress
Treatment was started with 0.022” slot pre-adjusted edgewise appliance (Nu Edge Cobalt Chromium Brackets, Roth prescription, TP Orthodontics Inc, Indiana, USA), and maxillary arch was bonded first. Archwires used for the treatment were procured from 3M Unitek Orthodontic products, USA. Correction of cross bite with 21 was done by aligning the upper arch using 0.016” NiTi archwire without the instanding lateral 22 in the first visit. Bilateral fixed posterior bite plane was given to raise the bite. After correction of cross bite with 21, NiTi open coil springs (Rabbit force, USA) were engaged between 21 and 23 to create space for 22 [Figure 5] and 22 was aligned using 0.012” NiTi piggy back archwire. After aligning the upper arch, the patient was subjected to lower incisor (31) extraction. Initial alignment and leveling was done with 0.016” NiTi followed by 0.016” and 0.018” stainless steel (Special plus, A.J. Wilcock Australian stainless steel, Australia). Inversion of upper left lateral incisor (22) bracket was done to achieve good torque correction. After alignment, leveling was done with 0.019” × 0.025” NiTi. After initial alignment and leveling, 0.019” × 0.025” stainless steel was placed in the upper and lower arch for torque expression, and most of the extraction space was closed during the alignment of the lower anterior crowding. Settling of occlusion was done with 0.019 × 0.025” stainless steel wire in upper and lower anterior tooth and vertical settling elastics (Tru-Force Latex Elastics, Red, 3/16”, TP Orthodontics Inc, Indiana, USA) in posterior [Figure 6]. Retention was given with a custom-made removable Hawley’s retainer in the upper arch and canine to canine-bonded fixed retainer custom-made with ligature wire (Ortho organizers, Carlsbad, CA) in the lower arch.
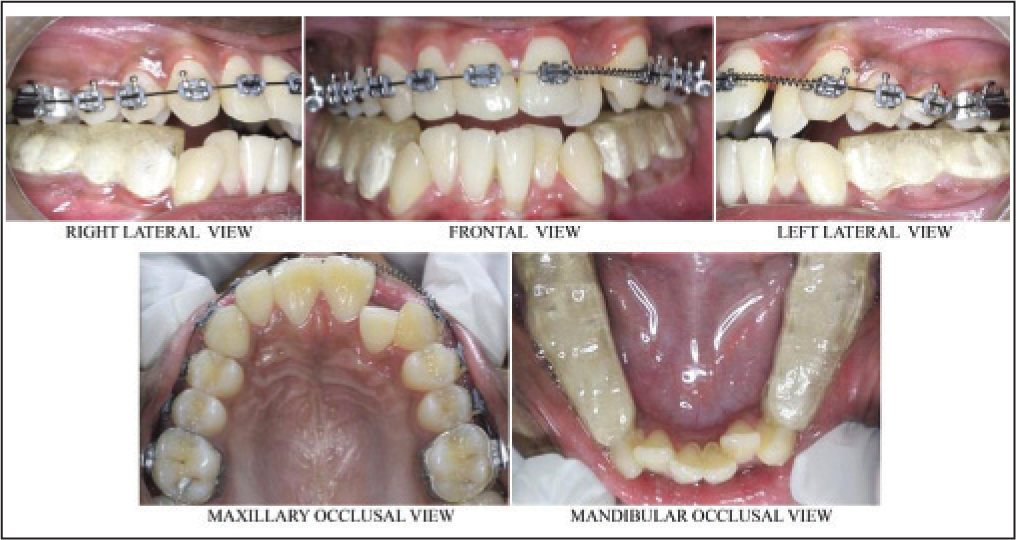
- Mid-treatment photographs
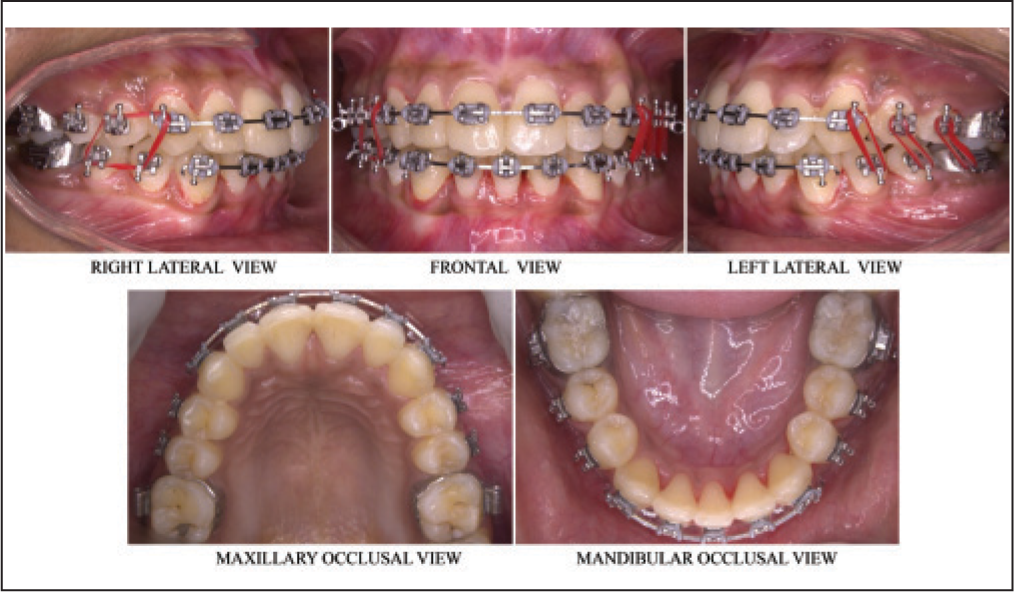
- Settling of occlusion photographs
Treatment results
Facial photographs showed only little changes in the facial profile and a very good improvement in the smile of the patient [Figure 7]. The post-treatment results showed a good occlusion between the upper and lower arches and a good inter-cuspation of the posterior teeth [Figure 8]. There was a pretty good alignment of the upper and lower arches. An esthetically acceptable smile arc was achieved after the correction of the maxillary anterior crossbite. Pre and post treatment cephalometric values are shown in [Table 1].
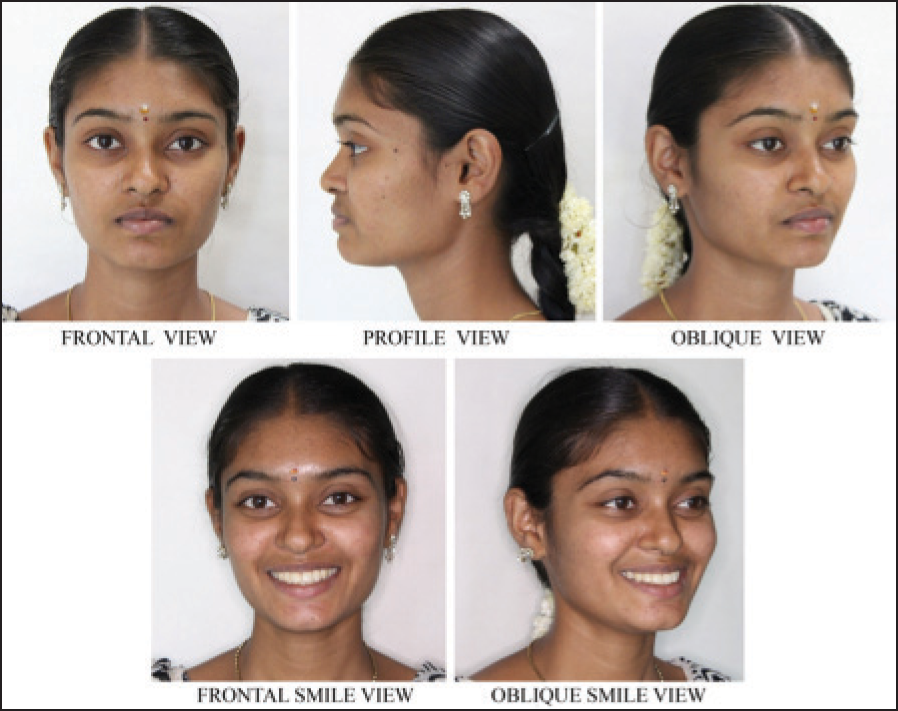
- Post-treatment extra oral photographs
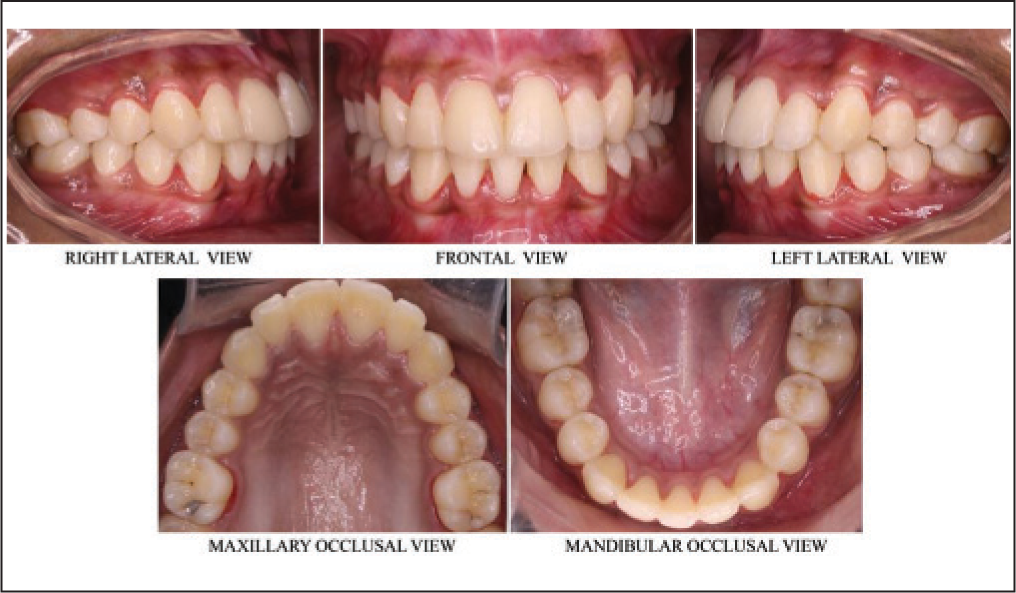
- Post-treatment intra oral photographs
| Parameters | Pre-treatment | Post-treatment |
|---|---|---|
| SNA angle | 82° | 83.8° |
| SNB angle | 85° | 85° |
| ANB angle | –3° | -1.6° |
| GoGn to SN | 15° | 14.5° |
| Lower anterior face height (mm) | 61 mm | 61 mm |
| U1 to NA angle | 46° | 40.9° |
| U1 to NA (Linear) | 13 mm | 10 mm |
| L1 to NB angle | 21° | 28.6° |
| L1 to NB (Linear) | 10 mm | 4.1 mm |
| L1 to Mand. Plane angle | 100° | 102° |
DISCUSSION
Extraction of mandibular incisor for orthodontic treatment has long been discussed by many authors. Extraction of mandibular incisor is generally done in patients with Bolton’s discrepancy of more than 2.0 mm. The case described here is a skeletal class III patient with good facial profile and crowding of the arches and crossbite only in relation to the anterior region of the upper and lower arches. The treatment plan was to extract the lower incisor (31). The extraction of lower incisor in this case is highly favorable because it helps in maintaining the facial profile and also in the correction of lower anterior crowding. The correction of upper anterior crowding could be achieved by mild proclination of the upper anteriors [Figure 9] and passive expansion of the arch, which is an acceptable compromise in the camouflage of skeletal class III malocclusions. The post treatment orthopantomogram showed good alignment of the roots and good amount of inter-dental bone present [Figure 10]. Daniel J Grob[16] has described a similar case in which mandibular incisor extraction was done in order to maintain the acceptable facial profile and to compromise for a skeletal class III tendency and showed stable results. Prakash et al.[10] published a similar case treated with mandibular incisor extraction for the correction of lower anterior crowding. Since the extractions of premolars were avoided, the maintenance of posterior occlusion was not a concern and it also reduces the treatment time.

- Post-treatment lateral cephalogram
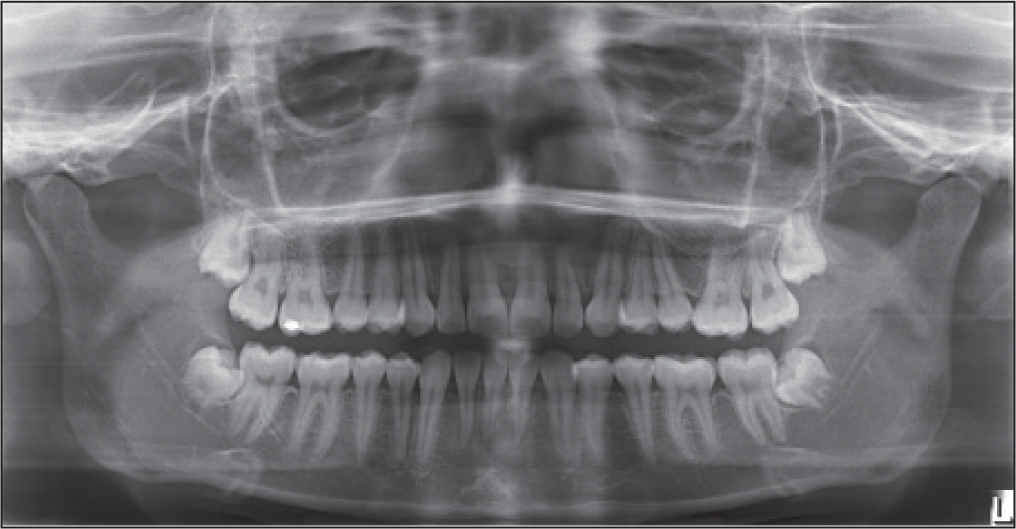
- Post-treatment OPG
A very good amount of posterior occlusion and inter-cuspation was easily achievable with the lower incisor extraction. Reidel et al.[17] undertook a study to compare the overall stability of patients treated with premolar extractions and those treated with extraction of single mandibular incisor and found more acceptable mandibular incisor alignment with single incisor extraction at post-retention. Vincent O Kokich[18] demonstrated a case treated with carious mandibular incisor extraction and presented a good maintenance of profile and satisfactory outcomes at the end of treatment. Canut[2] also found there is a better stability in patients treated with a single mandibular incisor extraction when compared with patients requiring premolar extraction. The present case was finished with a proper overjet of 2 mm, and the overbite was purposefully left at 3 mm in order to maintain the correction of anterior cross bite. In this case, the extraction of lower incisor lead to mismatched maxillary and mandibular arch midlines and a loss of interdental papilla in the lower anterior region resulting in a small black triangle. But, this is acceptable in order to maintain the esthetic facial profile and moreover, the lower midline and the black triangle are absolutely not visible during smile or speech and are not going to affect the esthetics of the patient in any sense. Previous case reports have also shown good results after lower incisor extraction treatment, which is in concordance with the case presented here.[15,17,19,20,21]
CONCLUSION
Camouflage of skeletal class III malocclusions when the patient has an acceptable profile and lower anterior crowding need a meticulous effort in order to avoid unesthetic changes of the profile and to have a stable result. Mandibular incisor extraction may be a good choice of treatment in such case for the correction of lower incisor crowding and also to maintain the facial profile. A proper diagnosis and treatment planning is the key factor in determining the success of treatment outcomes in orthodontic patients.
Source of Support:
Nil.
Conflict of Interest:
None declared.
References
- The decision making process in orthodontics In: Graber X, Vanarsdall V, eds. Orthodontics — Current principles and techniques (5th ed). St. Louis: Mosby; 2012. p. :15-7.
- [Google Scholar]
- Mandibular incisor extraction: Indications and long-term evaluation. Eur J Orthod. 1996;18:485-9.
- [Google Scholar]
- Effects of mandibular incisor extraction on anterior occlusion in adults with Class III malocclusion and reduced overbite. Am J Orthod Dentofac Orthop. 1996;115:113-24.
- [Google Scholar]
- Lower incisor extraction in orthodontic treatment: Four clinical reports. Angle Orthod. 1984;54:139-53.
- [Google Scholar]
- Considerations in mandibular incisor extraction cases. J Clin Orthod. 2009;1:45-51.
- [Google Scholar]
- Lower incisor extraction: An orthodontic treatment option. Dental Press J Orthod. 2010;15:143-61.
- [Google Scholar]
- The mandibular central incisor, an extraction option. Am J Orthod Dentofacial Orthop. 1997;111:253-9.
- [Google Scholar]
- Retention In: Graber TM, Swain BF, eds. Current orthodontic concepts and techniques (2nd ed). Philadelphia: WB Saunders Co; 1975. p. :1095-136.
- [Google Scholar]
- Retention In: Graber TM, Swain BF, eds. Orthodontics - Current principles and techniques (3rd ed). St. Louis: Mosby; 1985. p. :857.
- [Google Scholar]
- Extraction of a mandibular incisor in a class I malocclusion. Am J Orthod Dentofac Orthop. 1995;108:533-41.
- [Google Scholar]
- Mandibular incisor extraction: Post-retention evaluation of stability and relapse. Angle Orthod. 1992;62:103-16.
- [Google Scholar]
- Treatment of a class I malocclusion with a carious mandibular incisor and no Bolton discrepancy. Am J Orthod Dentofacial Orthop. 2000;118:107-13.
- [Google Scholar]
- The long term effects of one lower incisor extraction. Eur J Orthod. 1985;53:706-13.
- [Google Scholar]
- Retention and relapse In: Graber TM, Vanarsdall RL Jr, eds. Orthodontics: Current principles and techniques (2nd ed). St. Louis: Mosby; 1994. p. :908-50.
- [Google Scholar]
- Mandibular incisor extraction therapy — A case report. J Oral Res Rev. 2012;4:11-5.
- [Google Scholar]




