

Translate this page into:
The Double-sided Intrusion Spring
Address for correspondence: Dr. Fatih Celebi, Department of Orthodontics, Faculty of Dentistry, University of Gaziosmanpasa, 60100 Tokat, Turkey. E-mail: fatihcelebi5860@gmail.com
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
In deep bite cases, proper planning and practice are important in achieving the successful treatment outcomes. Bite opening is obtained with the aid of incisor intrusion, molar extrusion, or a combination of them. Pure incisor intrusion is a challenge for clinicians because incisor intrusion mechanics generally cause molar extrusion or incisor flaring. In the present article, a new technique that can be used for incisor intrusion without the mentioned handicaps was introduced.
Keywords
Deep bite
incisor protrusion
molar extrusion

Introduction
Deep bite is a malocclusion component that can cause unpleasant gingival display and traumatic ulcers. Furthermore, it can hinder the space closure in upper extraction cases because when intended to the space closure, upper incisors strike against the lower ones.
Various methods have been previously introduced for opening the bite, such as the archwires with the accentuated and reversed curve of Spee (AARCS), utility arch, three-piece intrusion arch, Connecticut intrusion arch, mini screw-supported techniques, and others.[1-3]
Of these methods, the most practical is certainly the AARCS technique. This technique, which does not require any auxiliary apparatus, can solve the problem with only one piece of the archwire.
The most critical problem with the AARCS is the protrusion of the upper and lower incisors. Studies have shown that the center of resistance for the anterior segment, which is composed of lateral and central incisors, is located on a projection line perpendicular to the occlusal plane between the canines and the first premolars.[4,5] Therefore, if the intrusion mechanism is applied at this point, the anterior segment can be moved purely in the apical direction without flaring. With AARCS, since force is applied to the brackets, and they are located more anteriorly according to the center of resistance, flaring of the incisors inevitably occurs.
The three-piece intrusion arch, which was introduced by Burstone, is significantly different from the others in terms of avoiding incisor flaring. The application point of this mechanism is positioned between the lateral and canine teeth to get as close to the center of resistance as possible. Another benefit is that since it is not fully engaged to the bracket slots, force can be adjusted and more gently force can be delivered.
Despite these advantages, the three-piece intrusion arch’s main disadvantage is the reactive force that is exerted on the distal segment, including molar and premolars. While incisors intrude with the aid of the arch, the reactive force causes extrusion of the distal segment. This handicap occurs not only with the three-piece intrusion arch but also with most of the intrusion arches, such as the utility and Connecticut intrusion arches. In patients who were decided to require pure incisor intrusion after the functional evaluation of gingival line about the upper lip line, molar extrusion is a side effect of orthodontic treatment.
The present article introduces a new technique that can be used for incisor intrusion without the aforementioned handicaps such as incisor flaring and molar extrusion. As opposed to extrusion, we even assert that molar intrusion can be achieved due to the nature of the mechanism.
Appliance Design
This intrusion system is composed of three components as follows: a main archwire, a vertical tube, and the double-sided intrusion spring (DIS). Before the intrusion stage, teeth must be well-leveled and aligned. DIS is preferably constructed of 0.017 × 0.025 - inch titanium molybdenum alloy, which can provide a desirable constant force. The main archwire, which engages to the sagittal part of the vertical tube as much as possible, provides stabilization of the spring. Preferably, 0.017 × 0.025-inch stainless steel for 0.018-inch bracket, and 0.019 × 0.025-inch stainless steel for 0.022-inch bracket are inserted as the main archwire [Figure 1].
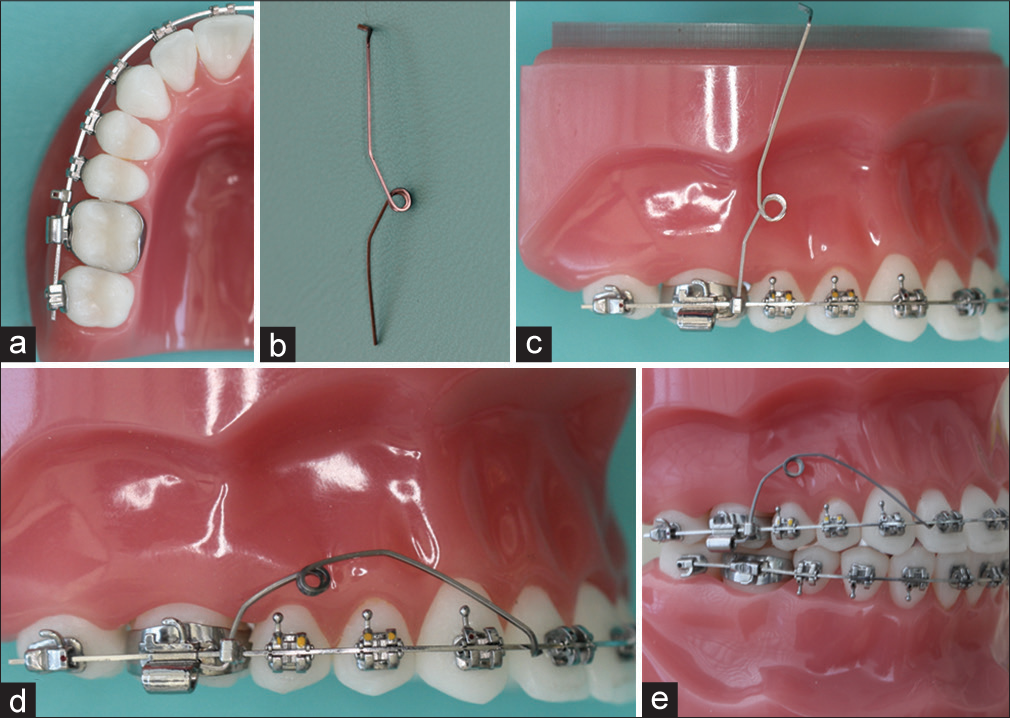
- (a-e) Installation of the double-sided intrusion spring to the fixed treatment system
DIS can be used for both mandibular and maxillary incisor intrusion without any constructional modification. The sole difference between them is the amount of force that is exerted by the spring, and this can be easily adjusted with the aid of the helix. In addition, DIS has the advantage of not requiring the use of a band as compared to the other options. It utilizes from the vertical tube inserted to the archwire.
The application point can be changed according to the desired intrusion type, such as intrusion protrusion or bodily intrusion. The spring is applied between the central and lateral incisors, or the lateral incisor and canine. As another alternative, it can be tied to the canine bracket with a piece of stainless steel ligature wire.
Discussion
The key feature in this system is the use of a vertical tube positioned between the first molar and second premolar teeth. This method ensures that reactive force does not extrude the molar teeth. Moreover, the spring actually makes the posterior segment intrude with the aid of the vertical tube [Figure 2].
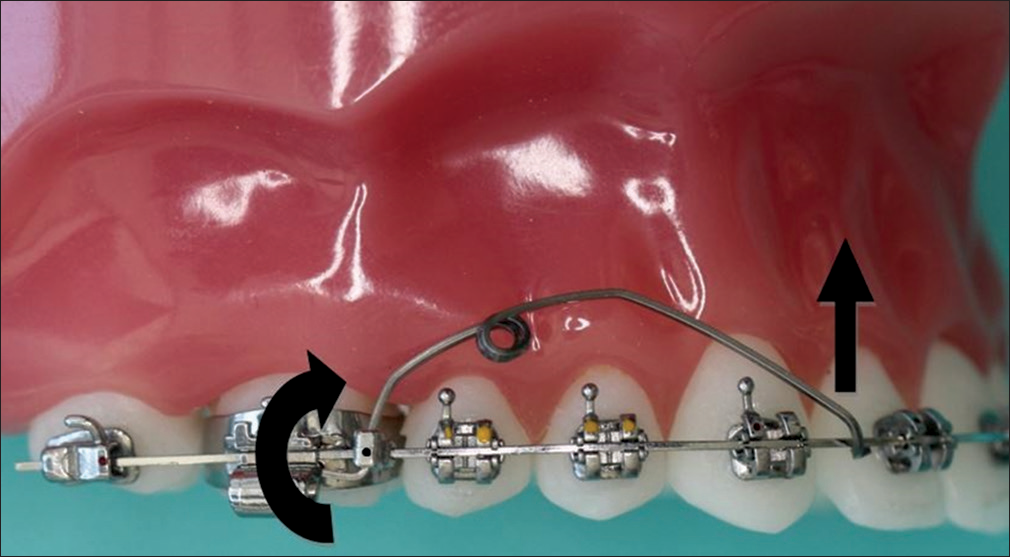
- Illustration of the force and momentum generated by the double-sided intrusion spring
Conventional intrusion arches such as the utility, three-piece, and Connecticut intrusion arches have the same basic technique; using tip-back bends at the molars to supply intrusive forces to the incisors. This technique results in desirable incisor intrusion, but the same time, undesirable molar extrusion inevitably occurs. The main difference between DIS and the others is that the direction of the anchorage unit is rotated from the sagittal to the vertical plane. This rotation causes significant changes, including molar intrusion rather than extrusion [Figures 3-5].

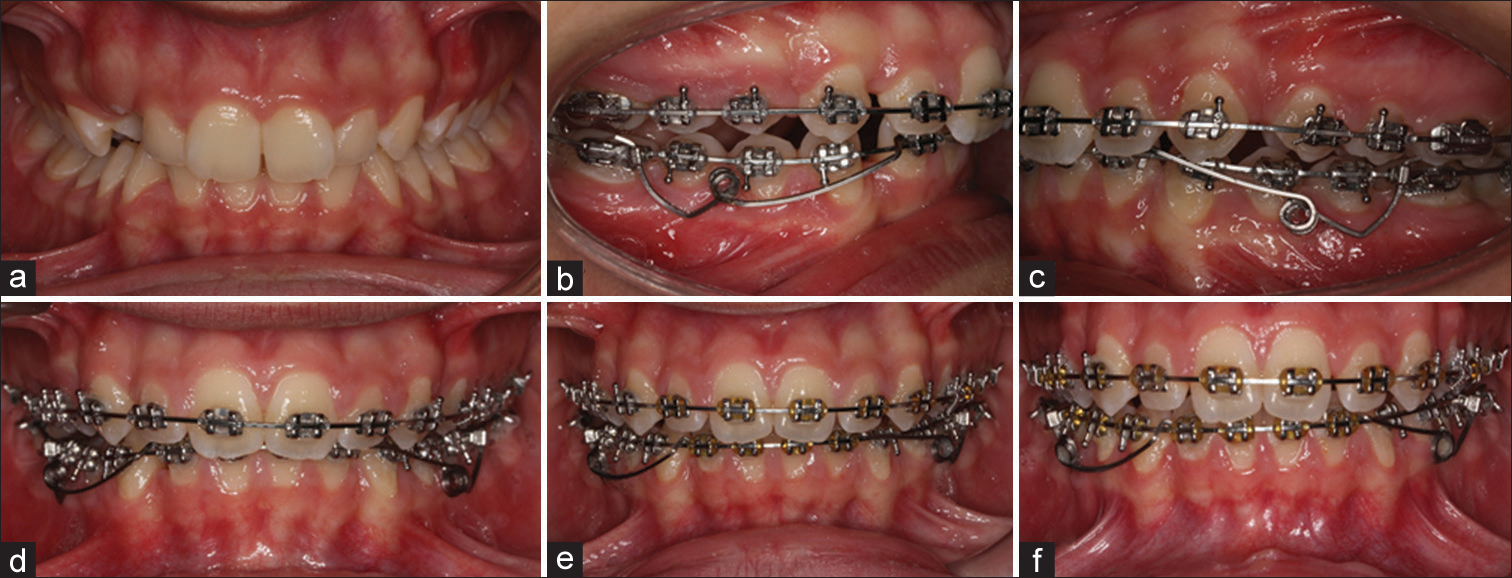
- (a) A 16-year-old female patient with proclined upper incisors, lower incisors in contacted with palatal mucosa and deep bite. (b-d) Application of the double-sided intrusion spring at the 8th month of the fixed orthodontic treatment. (e-g) Treatment sequences at the 2nd, 3rd, and 7th month after the application of the double-sided intrusion spring. (h-j). After 24 months of total treatment time

- (a) A 12-year-old male patient with class II dental and skeletal relationships, lower incisors in contacted with palatal mucosa and deep bite. (b-d) After the functional appliance therapy, application of the double-sided intrusion spring at the 3rd month of the fixed orthodontic treatment. (e-g) Treatment sequences at the 2nd, 4th, and 5th month after the initiation of lower incisors intrusion. (h-j) Treatment was completed after the 12 months of total fixed treatment time
- (a) A 16-year-old female patient with class II molar relationship, increased curve of Spee at the lower arch and deep bite. (b-d) Application of the double-sided intrusion spring at the 6th month of the fixed orthodontic treatment. (e and f) Treatment sequences at the 2nd and 4th month after the application of the double-sided intrusion spring
In addition, since the force application point can be carried to the posterior part of the dental arch, unlike the other alternatives such as AARCS and utility arch, incisor intrusion can be successfully accomplished through DIS without flaring [Figure 6].
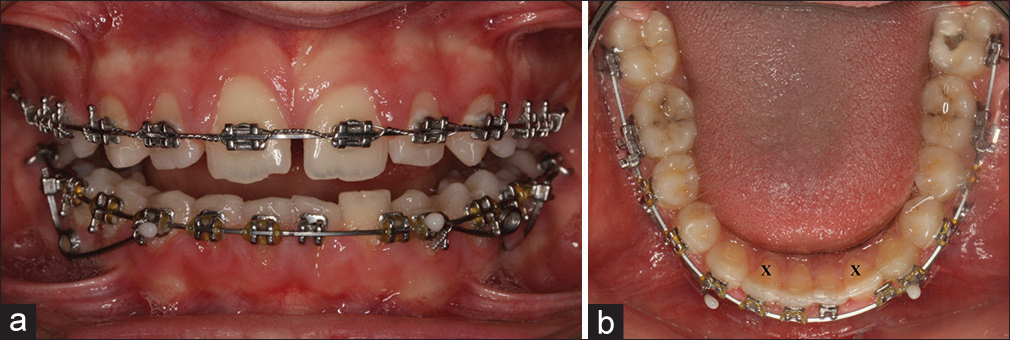
- (a and b) Patient who was applied intrusion spring, had lower left lateral incisor bracket failure between the consecutive appointments. Intrusion of the teeth adjacent to the lower left lateral tooth can be observed. In addition, it cannot be said remarkable tooth protrusion when two lateral incisors are compared with each others
Conclusion
DIS is a new spring design that can be used for incisor intrusion. The major advantage of this system over other options is that it also achieves molar intrusion while incisor intrusion is happening.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Bioprogressive therapy as an answer to orthodontic needs. Part II. Am J Orthod. 1976;70:359-97.
- [CrossRef] [Google Scholar]
- The center of resistance of anterior teeth during intrusion using the laser reflection technique and holographic interferometry. Am J Orthod Dentofacial Orthop. 1986;90:211-20.
- [Google Scholar]
- Evaluation of intrusive mechanics of the type “segmented arch” on a macerated human skull using the laser reflection technique and holographic interferometry. Am J Orthod. 1986;89:251-63.
- [CrossRef] [Google Scholar]




