

Translate this page into:
The preliminary outcomes of platelet-rich fibrin injection on pain perception following insertion of archwire: A randomized controlled clinical study
 , Hazem Hassan1, Fadi H. Khalil1, Alexander Abdulkader Kheirallah3
, Hazem Hassan1, Fadi H. Khalil1, Alexander Abdulkader Kheirallah3

*Corresponding author: Ali Ghassan Rokia, Department of Orthodontics and Dentofacial Orthopedics, Tishreen University, Latakia, Syria. aliandalus2017@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Rokia AG, Kheirallah M, Hassan H, Khalil FH, Kheirallah AA. The preliminary outcomes of platelet-rich fibrin injection on pain perception following insertion of archwire: A randomized controlled clinical study. APOS Trends Orthod 2023;13:1-7.
Abstract
Objectives:
This study aimed to determine the efficacy of platelet-rich fibrin (PRF) injection on orthodontic pain perception during the 1st week of the alignment and leveling process.
Material and Methods:
The study sample included 18 patients (11 females and 7 males). The patients were randomly divided into two groups, the PRF group (9 patients) and the control group (9 patients). The mean age of the sample members was 21.9 ± 2.5 and 20.8 ± 2.4 in the control and the PRF group, respectively. Conventional brackets were applied for both groups. PRF was injected into the six upper front teeth at a rate of 0.6 mm for each point before starting the primary wire insertion process. The pain parameters of each patient were evaluated for both groups during the 1st week of the alignment and leveling process by application of the Visual Analog Scale (VAS) at the durations of (2 h, 6 h, 1 day, 2 days, and 7 days) and all patients were followed up until the end of the alignment and leveling process.
Results:
PRF injection can reduce pain perception in orthodontic patients, overall (P < 0.05), with an effect size of approx. 53 ± 0.13%. The biggest effect was observed 2 h after exposure (P < 0.1) which showed a 50% reduction in pain in the PRF group. No significant effects were observed at later times (P > 0.1).
Conclusion:
The present study concludes that PRF injection can be an effective alternative for decreasing pain perception levels; however, its efficacy needs to be leveraged immediately after the injection of PRF.
Keywords
Platelet-rich fibrin
Orthodontic pain
Visual analog scale
Alignment process

INTRODUCTION
Orthodontic pain is commonly associated with discomfort during all orthodontic procedures. Immediately, after the implementation of orthodontic forces, inflammatory response stimulates the liberation of bradykinin and prostaglandin to enhance pain sensations.[1] Various factors affect pain perception, such as anxiety, pain sensitivity, gender, and age.[2] Various studies have shown that patients experience pain after the insertion of the initial archwire.[3] Teeth alignment and leveling are considered the first orthodontic curative phase, wherever the teeth are moving to achieve normal occlusal curvature and ideal dental contact points.[4] Despite the extended pain control technology, about 90% of patients experience pain in the initial stages of orthodontic treatment.[5] The pain commonly begins a few hours after fulfillment of an orthodontic force, then progressively decreases and gets back to the norm within 7 days.[6] Lew presented that 30% of patients left orthodontic treatment due to experiencing pain during the early stages of orthodontic treatment.[7] The source of pain during orthodontic tooth movement is not completely understood. Several reasons have been discussed. Some studies suggested that the compression of the periodontal ligament changes the blood flow and generates an immunological response of alveolar bone structures to create a favorable environment for tissue regeneration.[8] Excitation switches on the polarization of pro-inflammatory and anti-inflammatory cells to enhance tissue reconstruction. Moreover, bradykinin, histamine, serotonin, and prostaglandins are released causing inflammatory activation and hypersensitivity of pain receptors to ensue.[9] Consequently, the perception of pain intensity can be influenced by different environmental factors. Nevertheless, the precise mechanism for tissue regeneration is still uncertain, and more studies are needed for the further development of novel strategies to control the inflammatory process.
Various procedures have been utilized for pain control during orthodontic treatment. These contained anesthetic gel, ultrasound laser therapy, non-steroid anti-inflammatory drugs (NSAIDs), and transcutaneous electrical nerve stimulation.[10] However, the pain still cannot be eliminated and there is a need for adequate clinical evidence to determine the rationality of various methods. Platelet-rich fibrin (PRF), derived from human blood, has a wide variety of proteins, cytokines, inherent fibrin framework, and growth factors.[11] PRF injection permits the formation of a fibrin clot, which acts as a scaffold for tissue regeneration and has an influence on the immune response in vivo and in vitro.[12] Thus, PRF added under regenerative circumstances may relieve the immune response.[13] Therefore, it might be a suitable strategy to reduce patient complaints of pain and it may meet clinical needs. PRF injection is a readily autogenous, noninvasive, repeatable, and low-cost procedure. Some studies have evaluated the efficacy of submucosal injection of PRF on pain perception during tooth movement which showed an enhancement of tooth movement.[14] Moreover, PRF was shown to have anti-inflammatory properties after impacted third molar surgery.[15] However, we found no studies that examined the effect of PRF treatment on pain perception, particularly in the case of orthodontic treatment.
Considering the simultaneous positive effect on bone healing and anti-inflammation effects of injectable PRF,[16] we hypothesized that such treatment would produce a reduction in pain following archwire application. Since the pain occurs mostly within the 1st week before going back to its steady-state level, it is particularly important to aim for reducing pain within the window of the first 48 h since the start of treatment.
MATERIAL AND METHODS
Ethical approval
All participants received a detailed explanation of the study objectives and methods before signing an informed consent form. The study protocol was approved by the institutional ethics committee (approval number 3485/5/8/2019), and the investigation protocol was performed according to the Declaration of Helsinki for Medical Studies including human subjects (2013 revision). The data of this analysis are available upon request.
Subjects and study design
A randomized controlled clinical study was conducted, the sample consisted of 18 patients, (7 males and 11 females) who got orthodontic treatment. Documentation and orthodontic procedures were completed by the same orthodontist. The sample size was determined using G*Power software (version 3.1.9.7; Dusseldorf University, Germany) by conducting a pilot study based on the experimental sample where the values of the arithmetic averages of the Little index values were calculated before the alignment process in (mm) in both groups with a mean (M) of 5.83 ± 0.37 and 4.88 ± 0.71 for PRF and control groups, respectively.
Patient selection criteria
An initial clinical examination was conducted for 75 patients. The inclusion criteria involved healthy patients with a plaque and gingival index ≤1, aged (16–24), and moderate crowding between (3 and 6)mm in the maxillary anterior area according to the Little irregularity index,[17] and Class I according to Angle’s classification with normal growth pattern (Bjork 396 ± 6). The exclusion criteria included the presence of bleeding disorders, history of trauma in the anterior teeth, the presence of any systemic disease that affects the orthodontic movement, undergoing past orthodontic treatment and having any dental treatment within the 6 months before the study. Moreover, patients who were taking NSAIDs and pain relievers at least 6 months before the study were excluded from the study. During the study, all patients were asked and assured not to take any anti-inflammatory and pain relievers, and all patients adhered to the instructions. Those who achieved the inclusion criteria were required to fill out a form that qualify for one of two groups. In the end, 18 patients were selected to participate in the study, and informed consent was taken accordingly.
Treatment groups
The patients were randomly assigned to two groups, the injection PRF group, and the control group with an allocation of (1:1) using the sample randomization principle, where each patient was asked to pull out a closed white sheet from a black box containing 18 folded white sheets, nine of which were written on it (I-PRF) and nine written on it (control). Patients did not know which group they have been assigned to since the information about group assignment was hidden and not revealed by the researcher. Conventional MBT (0.022 brackets, Ortho Technology, USA) were fixed for all patients of the two groups, according to the date agreed with each patient. PRF was applied to the test group which comprised nine patients that were aged 16–24, with a male-to-female ratio being 44.4–55.6%.
PRF preparation
In the test group, the brachial vein was determined and the area was disinfected for drawing blood. Following that, using a 20-mL syringe, an amount of 20 mL of blood was drawn. Then it was placed in sterile dry centrifuge tubes that do not contain anticoagulant and then centrifuged. The centrifuge parameter was carried out in one stage according to the Ghanaati et al. protocol. Therefore they were subject to 600 rotations per minute (rpm) for 8 min at room temperature. Hence, PRF was still liquid for about 15–30 min.[11,12] The product of the centrifugation process was composed of red color stratum, which is the red blood cells located on the floor of the tube, and a stratum of yellow color, which is the PRF present at the top of the tube. A uniform amount of liquid was obtained about 4 mL, given that the sedimentation of 10 mL of blood gives 2 mL of PRF liquid. The PRF fluid was collected and withdrawn from the centrifuge tubes by a G 23 needle.
PRF injection
The patient was asked to rinse with disinfectant before the appointment to reduce the presence of bacteria during the injection process. 1 mL of an anesthetic agent was administered (Lidocaine HCL 2% with Epinephrine 1:80000) for pain control. Both groups were injected with the same amount of anesthetic. Among the PRF group, 0.6 mm of PRF was injected into each of the six front teeth in the area of the adherent gingiva submucosal using a G 27 needle. Normal saline was injected into the control group for blinding the experiment. For all participants, after the injection process was complete, a 0.14-inch wire was placed to start the process of teeth alignment and leveling.
Teeth alignment and leveling stage
In both groups, the process of alignment and leveling commenced with the insertion of a 0.14-inch wire (Nitinol) which was replaced every 3 weeks. The process was followed up until the ribbed wire (NiTi [0.016]*[0.016] – NiTi [0.017]*[0.025]” - S.S. [0.019]*[0.025]” Ortho Technology, USA) were reached sequentially. All patients were informed about the proper way to brush their teeth according to the modified Bass method.[18] All patients were followed up until the completion of orthodontic treatment.
Clinical assessment
To measure the pain variable, a questionnaire was distributed to all patients participating in the study and they were asked to answer a set of questions about the pain they had experienced after the appliance insertion. The intervention occurred by an orthodontist if one of the patients has not understood any option included in the questionnaire. The questionnaire includes a visual analog scale (VAS) which is a popular method for measuring pain intensity.[19,20] VAS uses a straight horizontal line of extent measuring 10 cm. The ends state the maximum limit of pain orientated from the best (right) to the worst (left) so that the patient can indicate the intensity of the pain (0–100). The intensity of pain is made by measuring the dimension from “no pain” to “very severe pain” based on the patient’s signs. The questions about the intensity of pain contained the intensity of pain after (2 h, 6 h, 1 day, 2 days, and 1 week) for each patient included in the study. The scores were used to indicate pain intensity and were in the following ranges: very severe (86–100), severe (65–85 mm), moderate (41–64 mm), mild (5–40 mm), and no pain (0–4 mm). The survey form was demonstrated and given to the patients before the procedure to be applied and brought back during the next visit. Importantly, the evaluation started after 2 h to eliminate the effect of the local anesthetic agent and to prevent biased results.
Statistical analysis
A variety of equations from Rosner[21] were used to run a post hoc power calculation to estimate the study’s ability to examine the impact of PRF on VAS scores. A statistical software package (SPSS, version 16.0, Chicago, IL, USA) was used for the statistical analysis. To verify the distribution of the studied variables, the Kolmogorov-Smirnov test was used. A standard student’s t-test was performed to study the significance of the differences in the average VAS values. Initially, an overall analysis was performed, whereby VAS values were collected per each group, regardless of the time since treatment. In the subsequent analysis, both groups were compared at the different periods following PRF exposure (2 h, 6 h, 1 day, 2 days, and 7 days), also using a pairwise t-test however for each time point separately. The results were evaluated with a 95% confidence interval. The significance level was set as P < 0.05 for statistically significant cases and P < 0.1 for marginally significant cases. A full multivariate statistical model that includes confounders (e.g., sex and age) was not undertaken because, given our experimental nature of the study, a direct comparative analysis using a t-test is appropriate. Moreover, from our initial clinical inclusion and exclusion process, inappropriate confounders were eliminated.
RESULTS
The data were found to be normally distributed (P < 0.05). Eighteen individuals participated in the present study (61.1% females and 38.9% males). The age range was between 16 and 24 years (mean 20.8, SD = 2.4). PRF was applied in 50% of the patients in the sample (55.6% females and 44.4% males). The average score of pain intensity in the PRF group was 22.44 ± 18.78, whereas in the control group it was 47.78 ± 21.52. Therefore, the effect size of PRF on reducing pain perception was approx. 53 ± 0.13%. From our post hoc power calculation and with the aforementioned averages and variability scores, this study has 75.9% power to detect the impact of PRF on pain (alpha = 0.05). Moreover, assuming an “a priori” power calculation after collecting study data, it appeared that 18 individuals are required to detect the effect of PRF on pain.[21,22]
As far as the temporal group analysis is concerned, the mean values of pain intensity in the PRF group were 17.22 ± 18.89, 29.11 ± 25.56, 30.00 ± 28.17, 31.11 ± 30.90, and 3.89 ± 4.86 for 2 h, 6 h, 1 day, 2 days, and 7 days groups, respectively. On the other hand, the pain intensities in the control group were 34.44 ± 21.42, 40.56 ± 19.76, 47.22 ± 17.16, 33.89 ± 19.17, and 7.89 ± 12.95 for 2 h, 6 h, 1 day, 2 days, and 7 days groups, respectively [Figure 1]. The highest average score of severe pain was noted after 1 day in the control group (M = 47.22 ± 17.16). On the other hand, the lowest average score of pain was noted in the PRF group, 1 week after the treatment (M = 3.89 ± 4.86). Crucially, within the first 3 days of the experiment, the biggest difference between the PRF and control groups was observed 2 h after the treatment, with the PRF group being on average 17.22 units lower than the control group [Figure 1], which represents a roughly 50% reduction [Figure 2]. The pain disappeared completely after 1 week in 55.6% (5 out of 9) of patients in the PRF group and 44.4% (4 out of 9) in the control group. For the rest of the patients in both the PRF and control group (4 out of 9), after 1 week, the pain intensity was “mild.” Two hours after wire insertion, “mild” to “severe” pain was reported by 66.6% of patients (6 out of 9) in the PRF group, whereas the percentage was 88.8% (8 out of 9) of patients in the control group. About 44.4% of patients (4 out of 9) in both groups complained of severe pain after 6 h. Finally, after 1-day moderate pain was reported in 33.3% (3 out of 9) of patients in the PRF group, while the fraction was 55.6% (5 out of 9) in the control group [Table 1].

- Average of pain intensity values in the sample according to the studied periods, with or without platelet-rich fibrin.
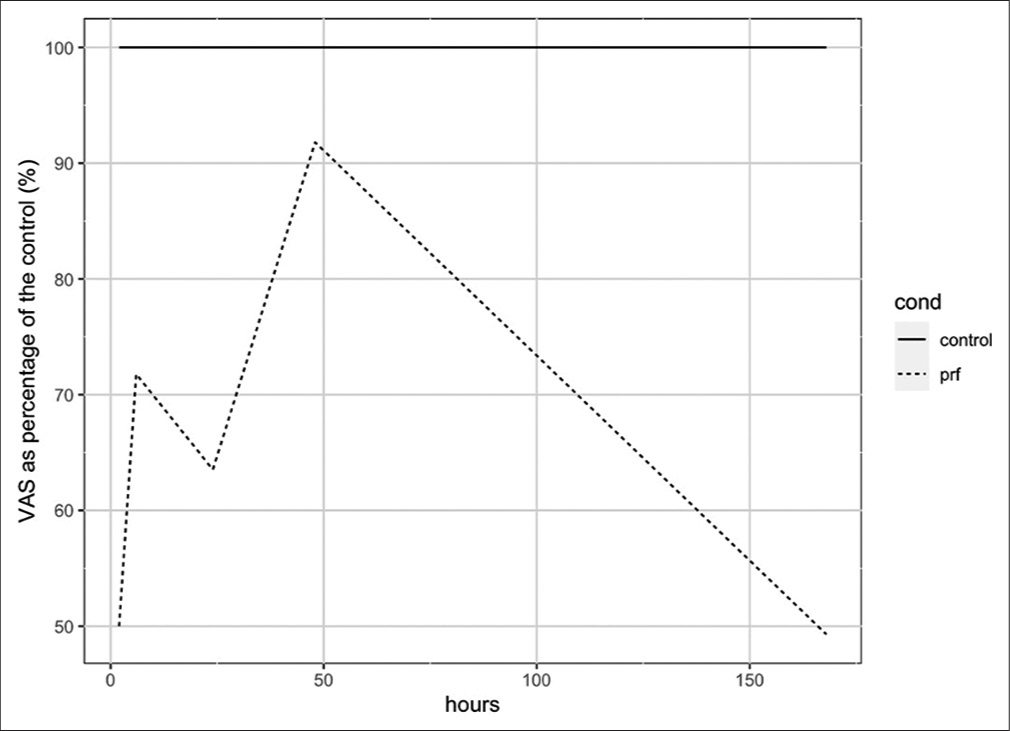
- Visual analog scale pain scores as a percentage relative to the control.
| Periods | Applied methods | Patients no and % | |||||
|---|---|---|---|---|---|---|---|
| No pain | Mild | Moderate | Severe | Very severe | Total | ||
| After 2 h | Conventional brackets with PRF | 3 (33.3) | 3 (33.3) | 2 (22.2) | 1 (11.1) | 0 (0) | 9 (100) |
| Conventional brackets without PRF | 1 (11.1) | 2 (22.2) | 2 (22.2) | 4 (44.4) | 0 (0) | 9 (100) | |
| After 6 h | Conventional brackets with PRF | 0 (0) | 5 (55.6) | 0 (0) | 4 (44.4) | 0 (0) | 9 (100) |
| Conventional brackets without PRF | 0 (0) | 2 (22.2) | 3 (33.3) | 4 (44.4) | 0 (0) | 9 (100) | |
| After 1 day | Conventional brackets with PRF | 1 (11.1) | 3 (33.3) | 3 (33.3) | 1 (11.1) | 1 (11.1) | 9 (100) |
| Conventional brackets without PRF | 0 (0) | 0 (0) | 5 (55.6) | 3 (33.3) | 1 (11.1) | 9 (100) | |
| After 2 days | Conventional brackets with PRF | 0 (0) | 5 (55.6) | 2 (22.2) | 1 (11.1) | 1 (11.1) | 9 (100) |
| Conventional brackets without PRF | 0 (0) | 2 (22.2) | 5 (55.6) | 1 (11.1) | 1 (11.1) | 9 (100) | |
| After 1 week | Conventional brackets with PRF | 5 (55.6) | 4 (44.4) | 0 (0) | 0 (0) | 0 (0) | 9 (100) |
| Conventional brackets without PRF | 4 (44.4) | 4 (44.4) | 1 (11.1) | 0 (0) | 0 (0) | 9 (100) | |
PRF: Platelet-rich fibrin, VAS: Visual analog scale
The initial analysis whereby the VAS values were obtained from the entirety of the experiment and split into two groups revealed that there is a statistically significant difference in pain perception between PRF and control groups [Table 2]. The difference between the PRF and control groups was 25.33 VAS units which corresponds to approx. 53% reduction in pain (P < 0.05). To discern the time dynamics of PRF treatment, a pairwise comparison between the PRF and control groups, revealed that the biggest impact occurs immediately after the exposure (i.e., after 2 h); however, this result was marginally significant (P < 0.1). There have been roughly 50%, 28%, 36%, 8%, and 51% reductions in VAS units after 2 h, 6 h, 1 day, 2 days, and 7 days, respectively [Table 3]. Therefore, it is possible to say; that even though there has been a gradual decline in the effect of PRF on the perception of pain since the beginning of the experiment, the suppression of the pain was consistent throughout it. This has a probability of observing such data given a null hypothesis equal to 3.1% (non-parametric estimation), providing support to the importance of PRF in reducing pain continuously. However, it is important to note that, despite observing such a reduction in pain perception, the observed effects were not always statistically significant in a pairwise time-by-time analysis [Table 4, P > 0.1].
| Group | N | M | SD | Min. | Max. | Mean difference | P-value | t-value |
|---|---|---|---|---|---|---|---|---|
| PRF group | 9 | 22.44 | 18.78 | 2 | 50 | −25.33 | 0.017 | −2.661 |
| Control group | 9 | 47.78 | 21.52 | 15 | 80 |
PRF: Platelet-rich fibrin, VAS: Visual analog scale
| Time since exposure | % Decrease in average VAS |
|---|---|
| 2 h | 50 |
| 6 h | 28 |
| 1 day | 36 |
| 2 days | 8 |
| 7 days | 51 |
VAS: Visual analog scale
| Periods | Methods | N | M | SD | Min. | Max. | Diff. | t-value | P-value |
|---|---|---|---|---|---|---|---|---|---|
| 2 h | PRF group | 9 | 17.22 | 18.89 | 0 | 50 | −17.22 | −1.809 | 0.089 |
| Control group | 9 | 34.44 | 21.42 | 0 | 60 | ||||
| 6 h | PRF group | 9 | 29.11 | 25.56 | 2 | 70 | −11.44 | −1.063 | 0.304 |
| Control group | 9 | 40.56 | 19.76 | 10 | 70 | ||||
| 1 day | PRF group | 9 | 30.00 | 28.17 | 0 | 90 | −17.22 | −1.566 | 0.137 |
| Control group | 9 | 47.22 | 17.16 | 25 | 80 | ||||
| 2 days | PRF group | 9 | 31.11 | 30.90 | 5 | 100 | −2.78 | −0.229 | 0.822 |
| Control group | 9 | 33.89 | 19.17 | 10 | 75 | ||||
| 1 week | PRF group | 9 | 3.89 | 4.86 | 0 | 10 | −4.00 | −0.868 | 0.398 |
| Control group | 9 | 7.89 | 12.95 | 0 | 40 |
PRF: Platelet-rich fibrin, VAS: Visual analog scale
DISCUSSION
Various methods have been applied to evaluate pain after archwire placement.[20,23] VAS is a valid test and many studies have used it to measure pain intensity, especially when expecting a large variance between individuals.[19,20] Moreover, other studies have evaluated the disability of VAS from moderate to good because of a weak correlation with other disability instruments and a strong correlation with the VAS for pain, however, its validity is questionable.[24] This study has inspected the pain intensity, using the VAS metric, during the 1st week after the archwires placement. Many factors may affect pain during orthodontic procedures. Several investigations have demonstrated that pain intensity is higher when superelastic nickel-titanium archwires are used than multistranded stainless steel archwires. On the other hand, using analgesic drugs could increase pain tolerance during the first stage of orthodontic treatment.[25,26] Moreover, not enough evidence patronize variations in pain levels between self-ligating and conventional brackets.[27] For these reasons, in our study standardized procedures and materials were used by one researcher.
Pain and discomfort are frequently experienced during orthodontic treatment. Pain is one of the causes of discomfort and could be recognized by self-report, but not every instance of discomfort could be linked to pain.[28] Pain frequently starts 4 h after archwire placement and maxes out at 24 h, then gradually decreases in its intensity by the 5th or 6th day.[23] Therefore, it is advantageous to discover a pain reduction method that reduces pain shortly after the archwire application.
This study examined the effect of PRF on pain perception among patients subject to archwire application, using a randomized controlled experiment. PRF is widely used in medicine and dentistry. Most studies have reported that PRF hastens orthodontic tooth movement and elicits an anti-inflammatory response.[13,14,29] Pain resulting from orthodontic forces is a sign of the subordinated mechanism of the inflammatory process which is a defensive response containing immune cells, blood vessels, and molecular mediators. Many in vitro studies and clinical trials deduced that platelet concentrates may effectively reduce the biological response of periodontal tissues and enhance bone regeneration.[30] Many surgical investigations concluded that PRF reduces pain, swelling, and trismus,[31] while no studies have demonstrated the leverage of PRF on the level of pain perception during the first phase of orthodontic treatment.
Regardless of the time since PRF injection, overall we do see a statistically significant effect of PRF application on pain perception among orthodontic patients that undertook archwire application. This initial analysis revealed an approximate halving of pain when comparing the PRF group to a control group (P < 0.05). Crucially our discovery is congruent with most studies that have unanimously concluded that injected PRF has anti-inflammatory efficacy and relieves pain.[13,14,29] The novelty of our experiment involved the use of PRF specifically in archwire application and providing evidence of the aforementioned effect. Given this initial finding, we hypothesized that the perceived pain reduction would vary as the time since injection progresses, and indeed we observe a gradual decline in pain reduction. Moreover, throughout the experiment, the average pain of the PRF group has always been lower than the control group. However, while the biggest difference was seen immediately after the PRF exposure and was marginally significant (P < 0.1), none of the differences observed subsequently were statistically significant (P > 0.1). Moreover, the limitation of our study is a relatively small sample size (n = 18). Given our data, it is possible to say that the biggest potential effect that PRF can have, is 2 h after its application. A possible explanation for that could be that the PRF mixture starts concentrated and subsequently gets diffused in the body as time progresses, thus weakening the observed differences in pain perception between the PRF and control groups. Given the experimental nature of our study, it is possible to say that pain reduction can be attributed to the injection of PRF. Finally, given the fact that the cost of the procedure is negligible in conjunction with the fact that there is a 50% reduction in pain, especially within the first 48 h, our findings point toward meaningful clinical relevance and application.
CONCLUSION
The present study concludes that PRF injection can be an effective alternative for decreasing pain perception overall (P < 0.05). The biggest effect was detected 2 h after the PRF injection (P < 0.1); however, it decreased in the subsequent time points during the 1st week of the alignment and leveling process. Studies with a larger sample than ours are needed to obtain more statistically meaningful results.
Acknowledgments
The authors would like to kindly thank the staff of the university clinics for their valuable technical support on this project.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Acceleration of tooth movement during orthodontic treatment-a frontier in orthodontics. Prog Orthod. 2013;14:42.
- [CrossRef] [PubMed] [Google Scholar]
- Individual differences in pain sensitivity: Measurement, causation, and consequences. J Pain. 2009;10:231-7.
- [CrossRef] [PubMed] [Google Scholar]
- The gliding path of the mandible along the skull. J Am Dent Assoc. 1980;100:670-5.
- [CrossRef] [Google Scholar]
- Perception of pain during orthodontic treatment with fixed appliances. Eur J Orthod. 2004;26(1):79-85.
- [CrossRef] [PubMed] [Google Scholar]
- The effect of low-level laser therapy during orthodontic movement: A preliminary study. Lasers Med Sci. 2008;23:27-33.
- [CrossRef] [PubMed] [Google Scholar]
- Attitudes and perceptions of adults towards orthodontic treatment in an Asian community. Community Dent Oral Epidemiol. 1993;21:31-5.
- [CrossRef] [PubMed] [Google Scholar]
- Pain in its environmental context: Implications for designing environments to enhance pain control. Pain. 2008;134:241-4.
- [CrossRef] [PubMed] [Google Scholar]
- Delivery strategies to control inflammatory response: Modulating M1-M2 polarization in tissue engineering applications. J Control Release. 2016;240:349-63.
- [CrossRef] [PubMed] [Google Scholar]
- The pain management in orthodontics. J Clin Diagn Res. 2013;7:1258-60.
- [CrossRef] [PubMed] [Google Scholar]
- Application of liquid plateletrich fibrin for treating hyaluronic acidrelated complications: A case report with 2 years of followup. Int J Growth Factors Stem Cells Dent. 2018;1:74-7.
- [CrossRef] [Google Scholar]
- Reduction of the relative centrifugal force influences cell number and growth factor release within injectable PRF-based matrices. J Mater Sci Mater Med. 2017;28:188.
- [CrossRef] [PubMed] [Google Scholar]
- Platelet-rich fibrin elicits an anti-inflammatory response in macrophages in vitro. J Periodontol. 2020;91:244-52.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of injectable platelet-rich fibrin (i-PRF) in accelerating orthodontic tooth movement: A randomized split-mouth-controlled trial. J Orofac Orthop. 2021;82:268-77.
- [CrossRef] [PubMed] [Google Scholar]
- Efficacy of platelet-rich fibrin in the reduction of the pain and swelling after impacted third molar surgery: Randomized multicenter split-mouth clinical trial. Head Face Med. 2015;11:37.
- [CrossRef] [PubMed] [Google Scholar]
- Anti-inflammation effects of injectable platelet-rich fibrin via macrophages and dendritic cells. J Biomed Mater Res A. 2020;108:61-8.
- [CrossRef] [PubMed] [Google Scholar]
- The irregularity index: A quantitative score of mandibular anterior alignment. Am J Orthod. 1975;68:554-63.
- [CrossRef] [PubMed] [Google Scholar]
- Pain Assessment, in Essentials of Pain Medicine. (4th ed). Netherlands: Elsevier Inc.; 2018. p. :39-46.
- [CrossRef] [Google Scholar]
- Experience of pain during an orthodontic procedure. Eur J Oral Sci. 2002;110:92-8.
- [CrossRef] [PubMed] [Google Scholar]
- Post hoc power analysis: An idea whose time has passed? Pharmacotherapy. 2001;21:405-9.
- [CrossRef] [PubMed] [Google Scholar]
- The pain and discomfort experienced during orthodontic treatment: A randomized controlled clinical trial of two aligning arch wires. Am J Orthod Dentofacial Orthop. 1992;102:373-81.
- [CrossRef] [PubMed] [Google Scholar]
- Reliability and validity of the visual analogue scale for disability in patients with chronic musculoskeletal pain. Int J Rehabil Res. 2008;31:165-9.
- [CrossRef] [Google Scholar]
- Perception of pain as a result of orthodontic treatment with fixed appliances. Eur J Orthod. 1996;18:349-57.
- [CrossRef] [PubMed] [Google Scholar]
- A randomized clinical trial investigating pain associated with superelastic nickel-titanium and multistranded stainless steel archwires during the initial leveling and aligning phase of orthodontic treatment. J Orthod. 2013;40:276-85.
- [CrossRef] [PubMed] [Google Scholar]
- Self-ligating brackets in orthodontics. A systematic review. Angle Orthod. 2010;80:575-84.
- [CrossRef] [PubMed] [Google Scholar]
- The differentiation between pain and discomfort: A concept analysis of discomfort. Pain Manag Nurs. 2019;20:556-62.
- [CrossRef] [PubMed] [Google Scholar]
- Platelet-rich fibrin in bone regenerative strategies in orthodontics: A systematic review. Materials (Basel). 2020;13:1866.
- [CrossRef] [PubMed] [Google Scholar]
- Platelet-rich fibrin (PRF): A second generation platelet concentrate, Part IV: Clinical effects on tissue healing. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101:e56-60.
- [CrossRef] [PubMed] [Google Scholar]
- Regenerative surgery performed with platelet-rich plasma used in sinus lift elevation before dental implant surgery: An useful aid in healing and regeneration of bone tissue. Eur Rev Med Pharmacol Sci. 2012;16:1222-6.
- [Google Scholar]




