

Translate this page into:
Undergraduate orthodontic education: Is there a slip between the cup and the lip?

Address for correspondence: Dr. Nikhilesh R. Vaid, Editor in Chief, APOS Trends, Department of Orthodontics, YMT Dental College, Navi Mumbai, Maharashtra, India. E-mail: orthonik@gmail.com
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Orthodontics is the first specialty of dentistry, and it requires no Newtonian hypothesis to understand that, in the 21st century for all specialties of dentistry, interdisciplinary protocols are the mantra for Quality Oral Health Care. The law of dependent origination is one of the most important teachings of the Buddha, and it is also a very profound fundamental principle at work in dependent originations. The sequelae of the principle is that of “cause and effect”. This is a realistic way of understanding the universe and is the Buddhist equivalent of Einstein’s theory of relativity.[1]
To illustrate the nature of dependent origination of the things around us, let us consider an oil lamp. The flame in an oil lamp burns dependent upon the oil and the wick. When the oil and the wick are present, the flame in an oil lamp burns. If either of these is absent, the flame will cease to burn. This example illustrates the principle of dependent origination with respect to a flame in an oil lamp.
We are witness to flickering lamps in the profession at various levels. Ask a young orthodontic specialist the biggest threat to his/her professional success or what is that one thing that is a roadblock to the growth of the profession, the answer you get more often than not in the Asia Pacific region is “general dentists” practicing orthodontics! Our colleagues imparting weekend courses to them are also the subject for great ire. It’s also disappointing that the orthodontic manufacturers whose products have made it easier for general dentists to promote and deliver orthodontic care, are driving the market perception of orthodontic care! The key issue for deliberation here is, are really the products stimulating dentists to provide orthodontic services? Or is the knowledge that these dentists innately have about orthodontics, due to archaic Undergraduate Orthodontic Education protocols, which make them gullible to advertising?
THE GOALS OF UNDERGRADUATE ORTHODONTIC EDUCATION
Let’s answer a question honestly. What do students learn in undergraduate orthodontic education? Practically very little, almost nothing! and theoretically, Concepts that are most often, not contemporary. The real information on the conceptual realities of tooth movement and its possibilities is considered the classified information to be discussed only with residents and specialists. There is no denying that fact that, orthodontics as a specialty, its vastness and time related treatment changes, do pose a challenge for didactic dissemination in an undergraduate setting; but do we really have the intent to teach it? Did we ever, as a specialty have it? The goals of most UG syllabi have been to teach dental students about diagnosing developing malocclusions in growing patients and the appropriate age of referral to an orthodontist. This helps the patient partially and is ideally aimed at helping the orthodontist. Prof. Kokich refers to this phenomenon as “self-serving”![2]
All dependent organizations can never ignore the What’s in it for me? (WIIFM) principle for interdependent fellows. Any intelligent and curious professional who has received such an exposure to orthodontics is obviously going to flirt with weekend courses and try a few cases themselves! What should we actually focus on, when we plan a syllabus for undergraduate students? The role orthodontics can play, in helping general dentists, toward achieving ideal results for comprehensive dental restorative cases.
This will probably get them into the WIIFM Zone and benefit the orthodontist, the general dentist and the patient population, at large!
THE PROBLEM COMPOUNDED!
When residents of mine(the co-authors), said they wanted to carry out a small survey for presenting at a general dental interdisciplinary convention at the school, I suggested we track referrals of patients checking into the institutions Out Patient Department.[3] The aim of the exercise was to assess and evaluate orthodontic treatment needs in adult patients visiting general dental clinics for concerns other than orthodontics, and the general dentist referral pattern to the Department of Orthodontics.
This prospective clinical study was conducted on 200 randomly selected adult patients (age >18 years). All the patients were subjected to an intra-oral examination by a panel of experienced orthodontists.
After intra-oral examination, these patients were categorized into three groups:
Patients not requiring orthodontic treatment
Patients requiring comprehensive orthodontic treatment
Patients requiring adjunctive orthodontic treatment.
Then the list of treatment recommendations on these patients case files were assessed to see whether any orthodontic opinion was recommended by the general dentist. The general dentist assessing the patients for their chief complaints, and recommending treatment options was unaware of the survey, thus making it a single blinded study attempting to eliminate any biases.
Patients included in the study had to meet the following criteria: They had to be adult patients (age >18 years), have a permanent dentition, their chief complaint did not relate to orthodontics, they approached a general dentist for dental concerns. Patients were excluded if they were: Children and adolescents (age <18 years), were seeking orthodontic treatment, had any history of orthodontic treatment, were totally edentulous, and required emergency dental treatment (presence of swelling, abscess, trauma etc.)
After statistical analysis, we results we got are summarized in Figures 1 and 2.
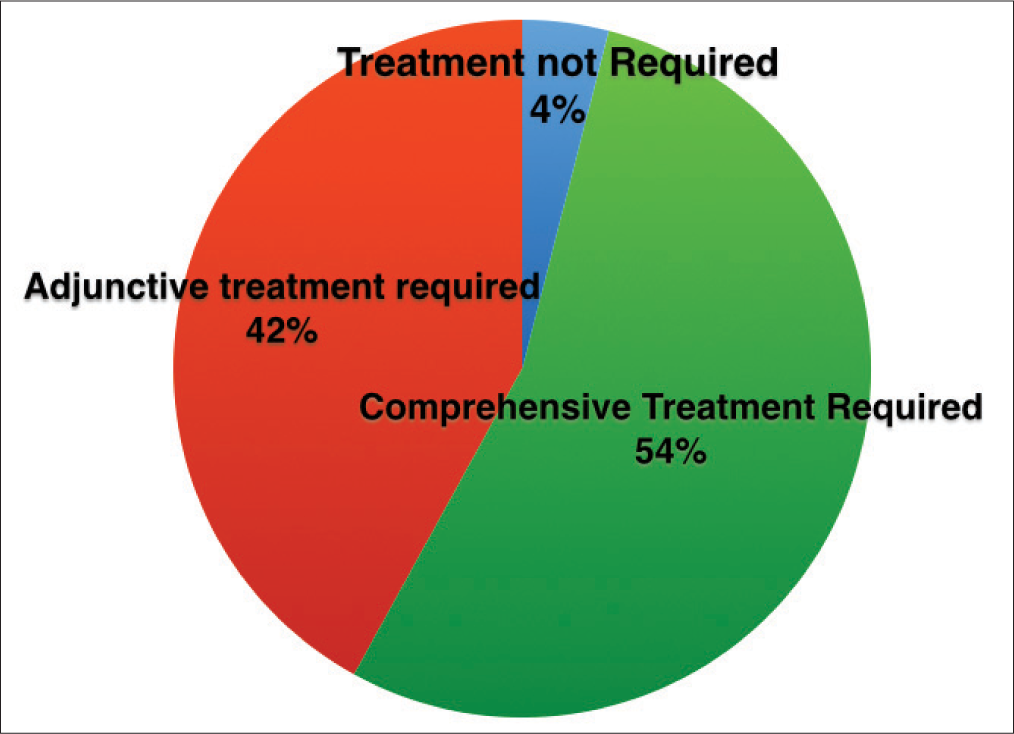
- Orthodontic treatment needs of the screened patients as assessed by the orthodontic panel. (4% patients didn’t need any treatment, 54% would actually benefit from full bonded comprehensive orthodontics, and 42% patients would benefit from adjunctive orthodontic therapy)
![Comparing patient’s actually needing orthodontics as per orthodontists recommendation, with treatment recommendations made by general dentists. (Only 16.67% patients [18 patients out of 108] needing comprehensive orthodontics were actually referred for treatment by the general dentists. Only 4.76% patients [4 patients out of 84] needing adjunctive orthodontics were actually referred for treatment by the general dentists)](/content/9/2015/5/3/img/APOS-5-091-g002.png)
- Comparing patient’s actually needing orthodontics as per orthodontists recommendation, with treatment recommendations made by general dentists. (Only 16.67% patients [18 patients out of 108] needing comprehensive orthodontics were actually referred for treatment by the general dentists. Only 4.76% patients [4 patients out of 84] needing adjunctive orthodontics were actually referred for treatment by the general dentists)
Orthodontic literature tells us that even when adults are self-motivated to undergo orthodontic therapy, one-half to two-thirds actually rely on their general dentist to provide the necessary referral.[4] Thus, general practitioners do play an integral role in identifying adult patients who might benefit from orthodontic treatment, as well as in arranging orthodontic consultation for patients who have decided on their own to seek treatment. If, as per our survey <20% dentists refer adults needing comprehensive therapy, for it; and <5% for adjunctive therapy to adults who need it, we’re looking at a serious problem here!
These are figures from a teaching institution in Asia, where nobody benefits out of not referring a patient to the appropriate specialist! So the reason for not referring on the GDPs part, primarily can be attributed to a failure to identify the need for treatment, in the first place itself. Undergraduate orthodontic education is staring at a major revamp in the specialty of orthodontics, if it is to provide its services to the fullest potential!
CLINICAL POSSIBILITIES
I happened to attend a symposium on “full mouth rehabilitation” for dentists, where a leading global specialist on TMDs and was discussing treatment protocols for various cases, after deprogramming them. In a specific case, where an upper molar had extruded due to extraction of the lower tooth in the same arch, opinions on treatment plans were sought. We’ve intruded such teeth with micro-implants a plenty, to facilitate vertical space for implants in the opposing arch. However, none of the non orthodontic audience, even suggested this as a treatment alternative. When I explained it, none had even heard about it, and were surprised that they never read about such simple mechanics, that would prevent intentional root canals and crowns for patients. Neither had their orthodontists ever mentioned about it to them. That moment was the stimulus for this editorial!
Whether its attrited teeth, that can be intruded to provide space to the dentist to restore them, or incisal inclinations causing trauma, or space redistributions and uprighting teeth to aid restorations and prosthesis; or even forced eruptions to develop implant sites, undergraduate orthodontic education, doesn’t even address these extremely critical areas.
This poses a huge problem for the future of orthodontics! The undergraduate orthodontic program needs to look beyond technique and theory bombardment, and focus on a restoratively centered and an interdisciplinary treatment planning driven program.[2] The supposed risk of exposing undergraduates to “fixed appliance orthodontics” is much smaller than losing referrals for cases, that can benefit from orthodontics, and thus increase the scope of the specialty, manifold!
ADDRESSING THE SLIP!
“It is the long history of humankind (and animal kind, too) those who learned to collaborate and improvise most effectively have prevailed.”
- Charles Darwin
Collaboration is the only way forward for the 21st century professional. Restructuring goals and allowing the spirit of creating a “value and a stake” in orthodontic care, to the undergraduate dental student is nonnegotiable for the tomorrow of orthodontics! If we do not “wake up and smell the coffee” on this pivotal aspect of orthodontic care, the “slips from cups to the lip,” I’m afraid, will be an exponential reality in holistic oral health care!
Nikhilesh R. Vaid, Jhanvi Ganatra, Dhaval Fadia, Meghna Vandekar
Department of Orthodontics, YMT Dental College, Navi Mumbai, Maharashtra, India
Address for correspondence: Dr. Nikhilesh R. Vaid, Editor in Chief, APOS Trends, Department of Orthodontics, YMT Dental College, Navi Mumbai, Maharashtra, India. E-mail: orthonik@gmail.com
References
- Available from: http://www.buddhism.about.com/od/basicbuddhistteachings/a/genesis.htm (Last accesed on 9 April 2015)
- The problem with predoctoral orthodontic education. Am J Orthod Dentofacial Orthop. 2013;143:595.
- [Google Scholar]
- Paper Presented at Sci-Clave 2015. YMT Dental College, Navi Mumbai, India: Orthodontic Intervention in Adult Dental Care; 2015.




