

Translate this page into:
Orthodontic camouflage via total arch movement in a Class II with idiopathic condylar resorption
Address for Correspondence: Prof. Kee-Joon Lee, Department of Orthodontics, College of Dentistry, Yonsei University 50 Yonsei-ro, Seodaemun-gu, Seoul 120-752, South Korea. E-mail: orthojn@yuhs.ac
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Idiopathic condylar resorption (ICR), also known as idiopathic condylysis or condylar atrophy, is multifactorial pathology leading to severe mandibular retrognathism. The etiology has been shown to be multifactorial, such as avascular necrosis, traumatic injuries, hormone and autoimmune disease and it is largely difficult to distinguish the exact cause in each individual. In spite of the remarkable morphological alteration, surgical intervention is not readily recruited due to the possibility of recurrence of resorption. In order to restore balanced facial profile and occlusion. In this report, we present a camouflage treatment for skeletal Class II with ICR and facial asymmetry involving total arch movement, for the improvement facial profile and reconstruction of occlusion.
Keywords
Camouflage treatment for skeletal Class II
idiopathic condylar resorption
total arch movement

INTRODUCTION
Idiopathic condylar resorption (ICR), also known as idiopathic condylysis or condylar atrophy, which is known to predominantly affect females aged 15-35 years, results in maxillofacial morphological features such as decrease in mandibular ramus height, loss of overall posterior facial height, mandibular retropositioning and resultant Class II with or without anterior open bite.[1-4] The morphological changes related to longstanding ICR may also lead to functional alterations in mastication, speech articulation, breathing, and lip closure, necessitating the reconstruction of the occlusion within the boundary of functional matrix.[1] The etiology has been shown to be multifactorial, such as avascular necrosis, traumatic injuries, hormone and autoimmune disease[5-9] and it is largely difficult to distinguish the exact cause in each individual.[1,2]
When ICR has occurred after the cessation of growth, remarkable mandibular retrusion, opening of mandibular plane and anterior open bite are typical resultants. In contrast, in the event of ICR during active growth phase, the net effect of normal mandibular growth combined with condylar resorption may resemble decreased mandibular growth, and stable anterior occlusion rather than open bite may result depending on the extent of condylar resorption and host capacity.[3,4] Facial asymmetry may be present when the pattern of condylar resorption on right and left side was different. Among the known treatment options of ICR such as an orthodontic camouflage, orthognathic surgery, distraction osteogenesis (DO) and total replacement of temporomandibular joint (TMJ),[1] invasive surgical interventions are not readily chosen due to the high recurrence of the resorption procedure.[10] In the case of severe mandibular retrognathism, however, conventional conservative orthodontic treatment within the alveolar housing may not be sufficient to produce satisfactory facial and/or occlusal change. Moreover, use of intermaxillary elastics is largely contraindicated because of the possible trauma to TMJ.[3,11] In this report, we present a camouflage treatment for skeletal Class II with ICR and facial asymmetry involving total arch movement, for the improvement facial profile and reconstruction of occlusion.
CASE REPORT
Diagnosis
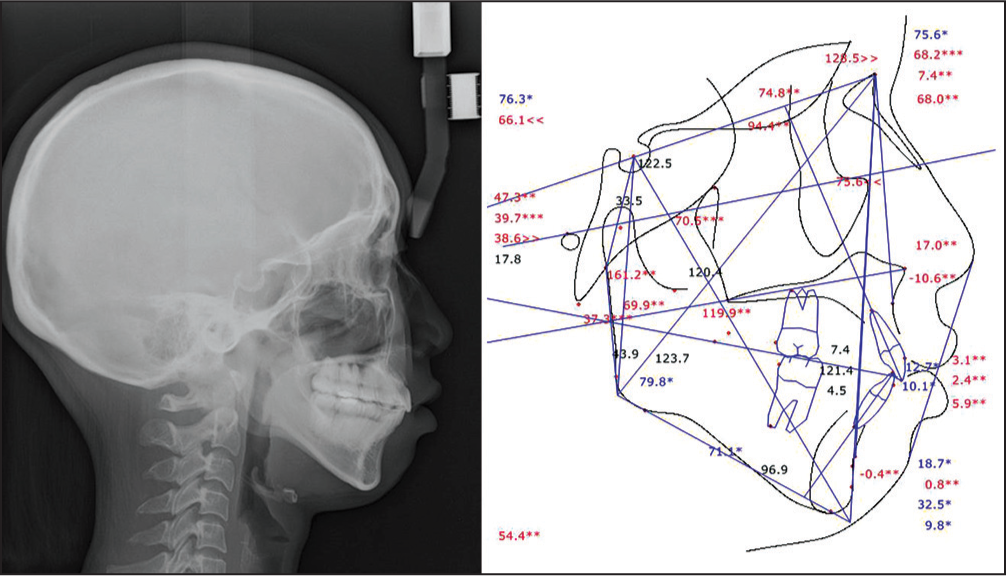
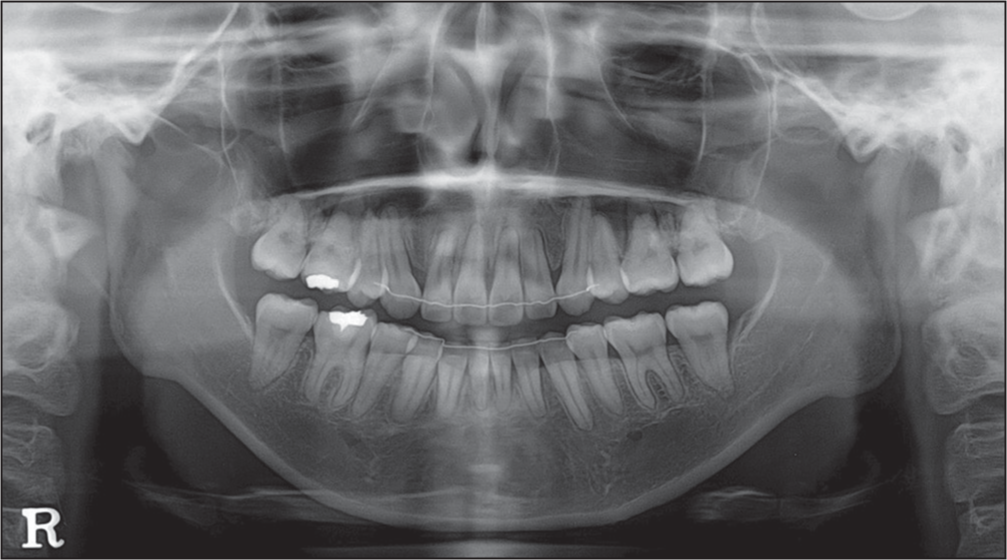
A 19-year-old female presented with incompetent lips and retruded mandible [Figure 1]. In the panoramic view, flattening of the condylar heads were remarkable on both TMJ, which was confirmed in the three-dimensional computed tomography [Figure 2]. Initial intra-oral views exhibited crowding in the upper and lower incisors and Class II molar relationship on the right side [Figure 3]. Arch length discrepancy was 6.0 mm in both arches. The upper denture midline was deviated 1.0 mm to the right, and lower dental midline was deviated 1.5 mm to the left, respectively, relative to the facial midline. Mild soft tissue chin deviation to the left was also noted. Initial cephalometric analysis revealed a Class II skeletal pattern (ANB = 8.9°) with high mandibular plane angle (49.7°) [Figure 4]. Asymmetric molar relation with Class II molar on the right side and incisor flaring (U1 to SN = 112.3°, IMPA = 105.8°) were also found.
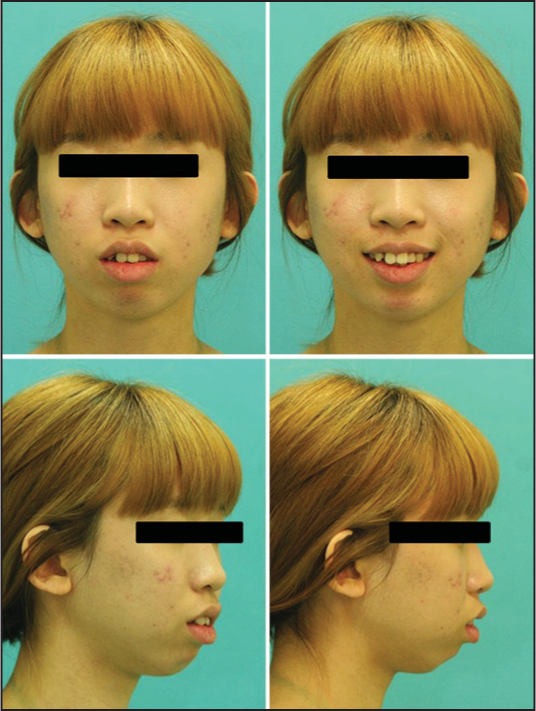
- Pretreatment extra-oral photographs

- (Top) Pretreatment panoramic view. (Bottom) Temporomandibular joint three-dimensional computed tomography

- Pretreatment intra-oral photographs

- Pretreatment lateral cephalogram
Treatment objectives
Reflecting the patients’ demand and the severity of the treatment objectives for this case included:
Improvement of soft tissue profile,
Elimination of lip incompetency,
Relief of upper and lower anterior crowding,
Axes correction of upper and lower incisors,
Establishment of Class I molar and canine key,
Establishment of proper overjet and overbite and
midline correction.
Treatment alternatives
Surgical repositioning of the mandible may be the treatment of choice to restructure the severe mandibular retrusion and related anterior protrusion. However, the mandible exposed to invasive surgical relocation may be subject to relapse or recurrence of the condylar resorption.[12] Alternatively, considering the amount of crowding and lip protrusion, nonextraction camouflage treatment was excluded for the possible flaring of incisors creating more protrusive lip profile. However, orthodontic camouflage involving extraction of premolars may also lead to insufficient profile changes, due to the limitation of anterior retraction and Class II molar relation. Therefore, an orthodontic camouflage to address greater profile changes was to be designed.
Treatment plan
Considering the amount of crowding and protrusion, extraction of the upper and lower first premolars was planned. Even with the anterior retraction under maximum anchorage, residual protrusion and lip incompetency was anticipated because of short upper lip and severe mandibular retrusion. Therefore, not only posterior retraction of anterior teeth, but total arch intrusion was needed to induce antero-superior autorotation of the mandible. Taken together, extraction of the upper and lower first premolars and 8 mm retraction of anterior teeth using asymmetric distalization of the upper right, upper left and lower left molars, and additional total arch intrusion were planned. Using dual miniscrews close to the estimated center of resistance of the upper dental arch, simultaneous distalization and intrusion of the total arch was planned,[13] to produce posterosuperior force vector(s) using dual miniscrews at each quadrant. To obtain maximum rotation of the mandible, application of the posteroinferior force vector was also decided using additional miniscrews in the mandible [Figure 5].
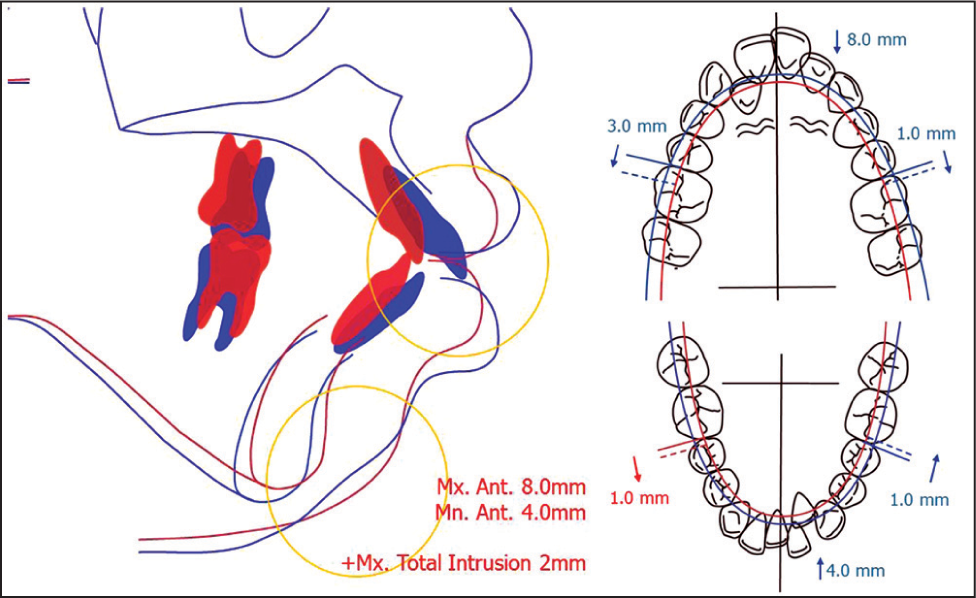
- Visual treatment objective and occlusogram
Treatment progress
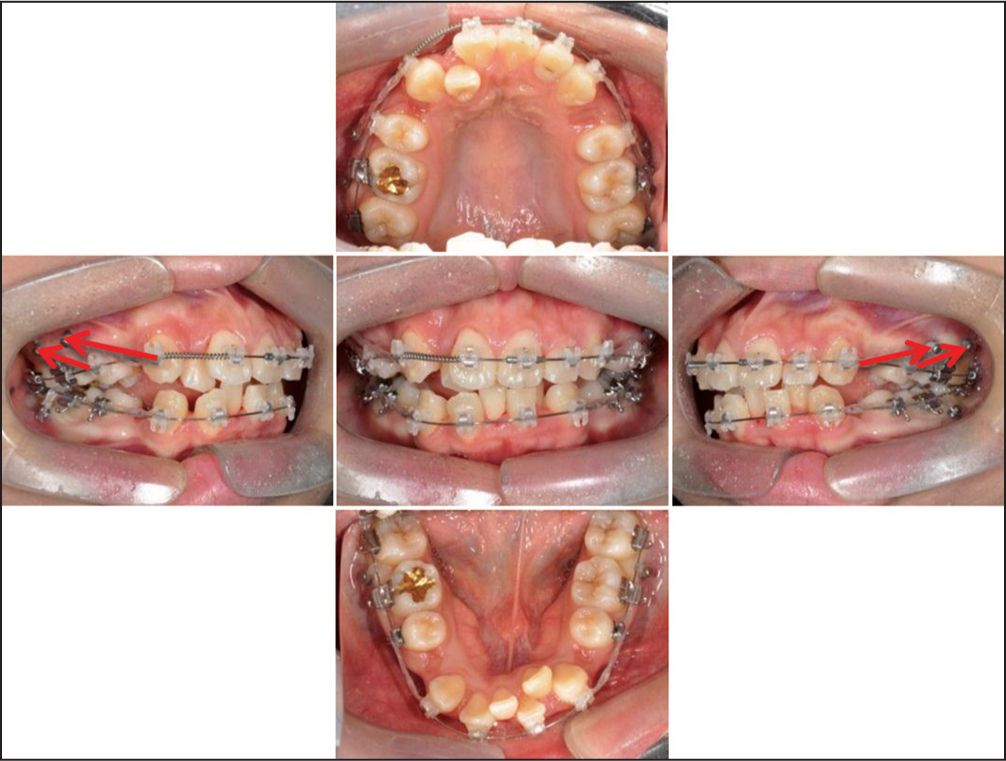
Extraction of 4 bicuspids (all first premolars) and all the third molars was performed for anterior teeth retraction. From the initial stage, four miniscrews were placed on buccal interproximal area between maxillary second premolar, maxillary first molar and second molar, bilaterally. Using these miniscrews, intrusive distalization of maxillary posterior segment and canine separate retraction were done using round 0.016˝ stainless steel archwire. Additional two miniscrews were placed on buccal interproximal area between mandibular first molar and second molar, bilaterally for intrusive buccal uprighting of mandibular molars [Figure 6]. Following the overall leveling and alignment at 8 months, maxillary and mandibular total arch intrusion was commenced with posterior-superior force vector using four miniscrews placed in each arch and 0.016˝ × 0.022˝ stainless steel with 10° palatal root torque on anterior teeth. Additional mandibular miniscrews were also inserted on the mesial side of the second premolar [Figure 7]. Occlusal settling was done with 0.016˝ stainless steel archwire and vertical elastics [Figure 8]. After bracket removal, lingual fixed retainer and circumferential removable appliance was delivered for retention.
- Treatment progress: Leveling and alignment stage

- Treatment progress: Total distalization and intrusion using multiple miniscrews
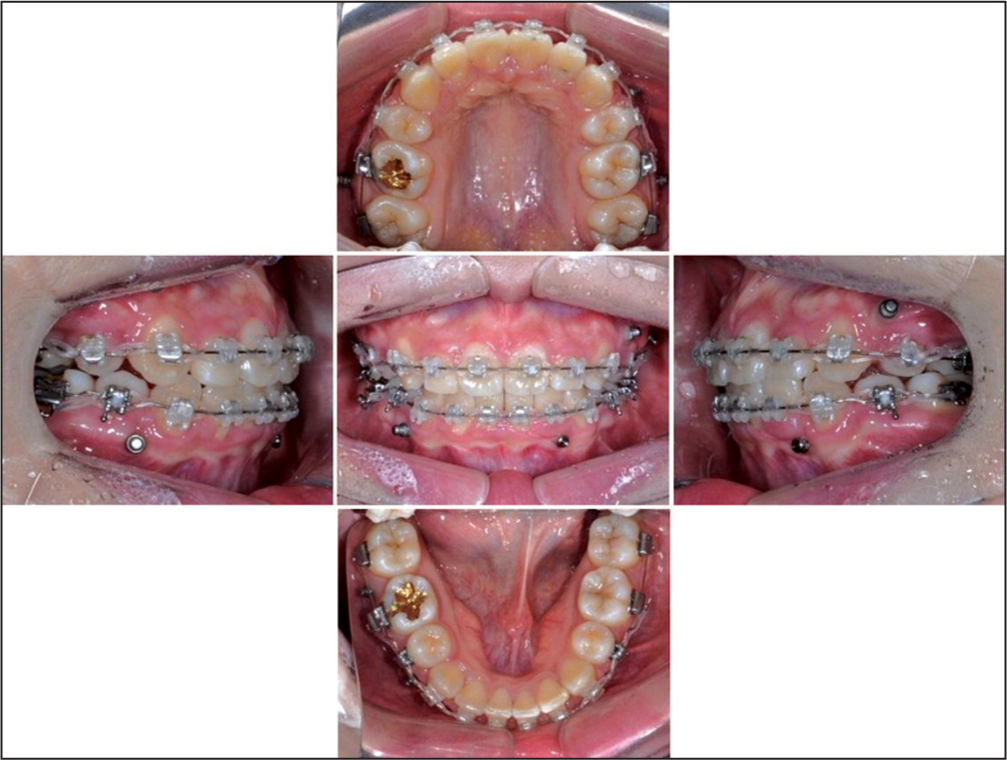
- Treatment progress: Settling of occlusion
Treatment results
Lip protrusion and incompetency were relieved [Figures 9-13]. In the cephalometric assessment, the upper and lower incisors were retracted by 10 mm and 8 mm, respectively through controlled tipping (U1 to SN angle reduced 17.9°, IMPA reduced 8.9°) [Table 1]. The upper molars were distalized and intruded by 2 mm, resulting in a counter-clockwise rotation of mandible. The SN to mandibular plane angle was reduced by 2.4° and soft tissue profile at chin area was improved. The roots were parallel except upper canines, and slight root blunting of incisors was observed.
| Measurements | Pretreatmet | Posttreatment |
|---|---|---|
| SNA (°) | 76.9 | 75.6 |
| SNB (°) | 68.0 | 68.2 |
| ANB (°) | 8.9 | 7.4 |
| Mandibular plane angle (°) (SN to GoMe) | 49.7 | 47.3 |
| Anterior facial height (mm) | 130.8 | 128.5 |
| U1 to SN angle (°) | 112.3 | 94.4 |
| L1 to mandibular plane angle (°) | 105.8 | 96.9 |
| U1 to NA (angular) (°) | 35.4 | 18.7 |
| U1 to NA (linear) (mm) | 10.7 | 0.8 |
| L1 to NB (angular) (°) | 43.5 | 32.5 |
| L1 to NB (linear) (mm) | 17.7 | 9.8 |
| Upper lip to E-plane (mm) | 7.2 | 3.1 |
| Lower lip to E-plane (mm) | 9.2 | 5.9 |

- Posttreatment extra-oral photographs

- Posttreatment intra-oral photographs
- Posttreatment lateral cephalogram
- Posttreatment panoramic view

- Superimposition of lateral cephalogram (Blue: Pretreatment, Red: Posttreatment)
DISCUSSION
Majority of the treatment options for ICR patients have been invasive surgical procedures, but very few of them are readily chosen due to the uncertainty of disease progress and the possible recurrence of ICR. According to the previous study, only 56% of patients with progressive condylar resorption treated by orthognathic surgery were asymptomatic and stable postoperatively, and the remainders (44%) have either TMJ symptoms or continued condylar resorption.[10] Arnett el al. stated that medial or lateral condylar compression associated with sagittal osteotomy creates possibility for late condylar resorption and B point relapse from 9 to 18 months after surgery.[4] Cutbirth et al. stated that patients with preoperative TMJ symptoms appeared to be a risk factor for condylar resorption.[14] DO can be effective in bone elongation for the deficient mandible, but is highly technique sensitive and is subject to the possibility of infection, scar, discomfort and paresthesia during the distraction process.[15] TMJ total replacement has recently been introduced as a radical procedure but has shown some limitations such as material wear and failure, lack of long-term stability report.[16]
In the same context, even in the pursuit of noninvasive camouflage treatment, procedures that can cause trauma to the existing TMJ such as the use of intermaxillary elastics needs to be avoided.[3,11] In summary, the present case requested not only the denture correction, but also maximum possible improvement of the facial profile, for which a three-dimensional manipulation of the denture including total arch intrusion was indispensible. Appropriate recruitment of intrusive mechanics to eliminate bite opening and posterior rotation of the mandible, multiple miniscrews alongside the dental arch were effectively incorporated. Considering the possible center of resistance of overall arch near the premolars, multiple intrusive distal force vectors were produced to displace respective upper and lower arches.
In spite of initial crowding, the eventual profile change at the end of treatment is very inspiring. The result is attributed by the combined anterior retraction, distalization of maxillary posterior segment and total intrusion causing autorotation of the mandible. Similarly, it can be addressed that the soft tissue incompetency even in the absence of anterior open bite can demand intrusion of total arch, for the improvement of the profile. Another advantage of the intra-arch mechanics using miniscrews is that it does not need intermaxillary elastics causing constant load on the TMJ.
Taken together, a camouflage treatment can be designed to induce desirable modification of the profile in a severe sequence of ICR. Intrusive total arch movement using multiple miniscrews can be effectively incorporated to have a predictable outcome, without the need of patient’s compliance.
CONCLUSION
For nonsurgical treatment of ICR patients with severe mandibular retrognathism, the maximum amount of tooth movement including retraction of incisors, distalization of the posterior segment and total arch intrusion may be effective for the improvement of denture and facial profile. According to the contact pattern of the occlusion, selective intrusion of a specific segment or total arch intrusion is required.
Source of Support:
Nil.
Conflict of Interest:
None declared.
References
- Idiopathic condylar resorption: Current clinical perspectives. J Oral Maxillofac Surg. 2007;65:1617-23.
- [Google Scholar]
- Idiopathic condylar resorption: Diagnosis, treatment protocol, and outcomes. Am J Orthod Dentofacial Orthop. 1999;116:667-77.
- [Google Scholar]
- Progressive mandibular retrusion — Idiopathic condylar resorption. Part I. Am J Orthod Dentofacial Orthop. 1996;110:8-15.
- [Google Scholar]
- Progressive mandibular retrusion — Idiopathic condylar resorption. Part II. Am J Orthod Dentofacial Orthop. 1996;110:117-27.
- [Google Scholar]
- MR of osteochondritis dissecans and avascular necrosis of the mandibular condyle. AJR Am J Roentgenol. 1989;152:551-60.
- [Google Scholar]
- Avascular necrosis of the mandibular condyle-pathogenesis and concepts of management. Oral Surg Oral Med Oral Pathol. 1993;75:428-32.
- [Google Scholar]
- Bilateral absorption of the capitulum mandibulae in rheumatoid arthritis. Acta Odontol Scand. 1961;19:247-57.
- [Google Scholar]
- Mandibular condylosis and apertognathia as presenting symptoms in progressive systemic sclerosis (scleroderma). Pattern of mandibular bony lesions and atrophy of masticatory muscles in PSS, presumably caused by affected muscular arteries. Oral Surg Oral Med Oral Pathol. 1987;63:269-74.
- [Google Scholar]
- Estrogen receptors in the temporomandibular joint of the baboon (Papio cynocephalus): An autoradiographic study. Oral Surg Oral Med Oral Pathol. 1986;61:307-14.
- [Google Scholar]
- Diagnosis and management of condylar resorption. J Oral Maxillofac Surg. 1997;55:114-9.
- [Google Scholar]
- The effect of intermaxillary elastic force on the temporomandibular articulation in the growing macaque monkey. Am J Orthod. 1971;60:491-504.
- [Google Scholar]
- Stability after reoperation for progressive condylar resorption after orthognathic surgery: Report of seven cases. J Oral Maxillofac Surg. 1994;52:460-6.
- [Google Scholar]
- Distalization pattern of the maxillary arch depending on the number of orthodontic miniscrews. Angle Orthod. 2013;83:266-73.
- [Google Scholar]
- Condylar resorption after bicortical screw fixation of mandibular advancement. J Oral Maxillofac Surg. 1998;56:178-82.
- [Google Scholar]
- Distraction osteogenesis in adult obstructive sleep apnea surgery: A preliminary report. J Oral Maxillofac Surg. 2002;60:6-10.
- [Google Scholar]
- The use of alloplastic prostheses for temporomandibular joint reconstruction. J Oral Maxillofac Surg. 2000;58:70-5.
- [Google Scholar]




