

Translate this page into:
Autotransplanted premolars for substituting traumatic maxillary central incisors in a Class II growing patient

*Corresponding author: Armando Montesinos F, Department of Orthodontics, National Autonomous University of Mexico, Circuito Institutos S/N Ciudad Universitaria, Colonia Copilco Universidad, Mexico City, Mexico. amfortod_@hotmail.com
-
Received: ,
Accepted: ,
How to cite this article: Montesinos FA, Robles DA, Nambo D. Autotransplanted premolars for substituting traumatic maxillary central incisors in a Class II growing patient. APOS Trends Orthod. 2025;15:195-204. doi: 10.25259/APOS_261_2023
Abstract
A 10-year-old young Hispanic male patient was referred to the Endodontics Department with the chief complaint of color change of maxillary central incisors. The parents reported trauma one year before and as a result root canal treatment; maxillary central incisors extractions were necessary due to poor prognosis, so he was referred to the Orthodontics Department to evaluate if the patient could be the candidate for orthodontic treatment, as he showed severe crowding. The patient had no medical conditions, and the pretreatment records showed a Class II skeletal relation and vertical pattern. Dental findings were mixed dentition, an Angle Class II molar relationship, moderate upper and lower anterior crowding, 4 mm of overbite, and 7 mm of overjet. The patient underwent autotransplantation of maxillary second premolars into the place of maxillary central incisors that needed to be extracted as stated by the endodontist (premolar extractions were needed to solve the orthodontic problems). The suggested position for the autotransplant teeth was not accomplished by the surgeon, so orthodontic forces were applied to the autotransplant teeth to the ideal position. At the end of orthodontic treatment, the autotransplanted teeth were restored by the prosthodontist. Therefore, the facial balance improved, and the final occlusal relationships were good. COVID-19 global lockdown was a challenging obstacle to overcome during treatment. This case report intends to highlight the potential benefits of tooth autotransplantation and to increase awareness of this treatment protocol.
Keywords
Autotransplantation
Skeletal Class II
Root development
Mixed dentition
Extraction treatment
Esthetic outcome
Short-term
Long-term stability

INTRODUCTION
Traumatic dental injuries (TDIs) are very frequent; children and adolescents suffer trauma from sports activity, unsafe playing, or accidents.[1,2] Andersson reported a prevalence of 20% in this population.[1,2] Glendor concluded that one-third of all children sustained a TDI in the primary dentition, one-fourth in the permanent dentition of all school children, and one-third of all adults.[3] TDI in primary dentition can damage and/or cause disturbances to the germs of permanent teeth;[4-6] On the other hand, permanent dentition can cause complications such as pulp necrosis and internal/or external root resorption and affect craniofacial growth.[6-8] Although traumatized teeth are managed endodontically, sometimes the decision to indicate the extraction of the traumatized tooth is required.[9] Consequently, dental implants or other restorative protocol are treatment options in an adult patient but not alternatives for a growing patient, because growing patients still have the potential for alveolar growth.[10,11]
Autotransplantation is the surgical movement of embedded or erupted teeth in the same patient from one site to another into extraction sites or surgical prepared sockets.[12-16] Autotransplantation of immature premolars is a successful protocol for restoring edentulous areas; it functions as a natural tooth because it has a periodontal ligament (PDL) on the surface of the root, facilitating the physiological movement.[12,16] A successful autotransplanted tooth can maintain and permit continuation of alveolar growth as it erupts with growth and can be moved orthodontically.[17]
This case report presents the autotransplantation of maxillary second premolars to the anterior region and orthodontic treatment of a mixed dentition skeletal Class II growing patient.
CASE REPORT
Diagnosis and etiology
A 10-year-old young Hispanic male patient was referred to the Endodontics Department with the chief complaint of the color change of maxillary central incisors. The patient’s parents reported trauma one year ago and as a result root canal treatment of both. Endodontic diagnosis showed periapical lesions, internal resorption, and grade 1 mobility. Maxillary central incisors extractions were necessary due to the poor prognosis, so he was referred to the orthodontics department to evaluate if the patient could be a candidate for orthodontic treatment as he showed severe crowding [Figure 1]. He had no significant medical history; the pretreatment records showed a Class II skeletal relation and vertical pattern [Table 1 and Figure 2]. The dental findings were mixed dentition, an Angle Class II molar relationship, moderate upper and lower anterior crowding, 4 mm of overbite,and 7 mm of overjet. Cone-beam computed tomography (CBCT) scan and panoramic radiograph confirmed the endodontist diagnosis report [Figure 3].

- Pretreatment photographs.
| FF | Norm | Pretreatment | Posttreatment |
|---|---|---|---|
| FMA | 25º | 32º | 29º |
| FMIA | 70º | 64º | 52º |
| IMPA | 90º | 85º | 95º |
| 1-SN Autotransplanted teeth-SN | 102º+-2 | 112º | 106º |
| SN/MP | 32º | 34º | 32º |
| OP/MP | 20º +- 5º | 31º | 29º |
| FACIAL AXIS | 90º +- 3.5º | 95º | 93º |
| WITS | 0 A -3 | 4.5º | 4º |
| SNA | 82º | 86.º | 88º |
| SNB | 80º | 80º | 81º |
| ANB | 3º | 6º | 7º |
| POST. FH | 45mm | 38.3mm | 51.3mm |
| ANT. FH | 65mm | 53.3mm | 64.7mm |
FMA: Frankfort mandibular plane angle, FMIA: Frankfort mandibular incisor angle, IMPA: Mandibular incisor to mandibular plane angle, 1-SN: Angle between upper incisors and Sella-Nasion, SN/MP: Angle between sella-nasion to the mandibular plane, OP/MP: Angle between occlusal plane to mandibular plane, SNA: Angle between the sella/nasion plane and the nasion/A plane, SNB: The angle between the sella/nasion plane and nasion/B plane, ANB: Angle formed by point A, Nasion and point B, ANT.FH: Anterior Facial Height, POST.FH: Posterior Facial Height, WITS: The “WITS” appraisal for jaw disharmony.
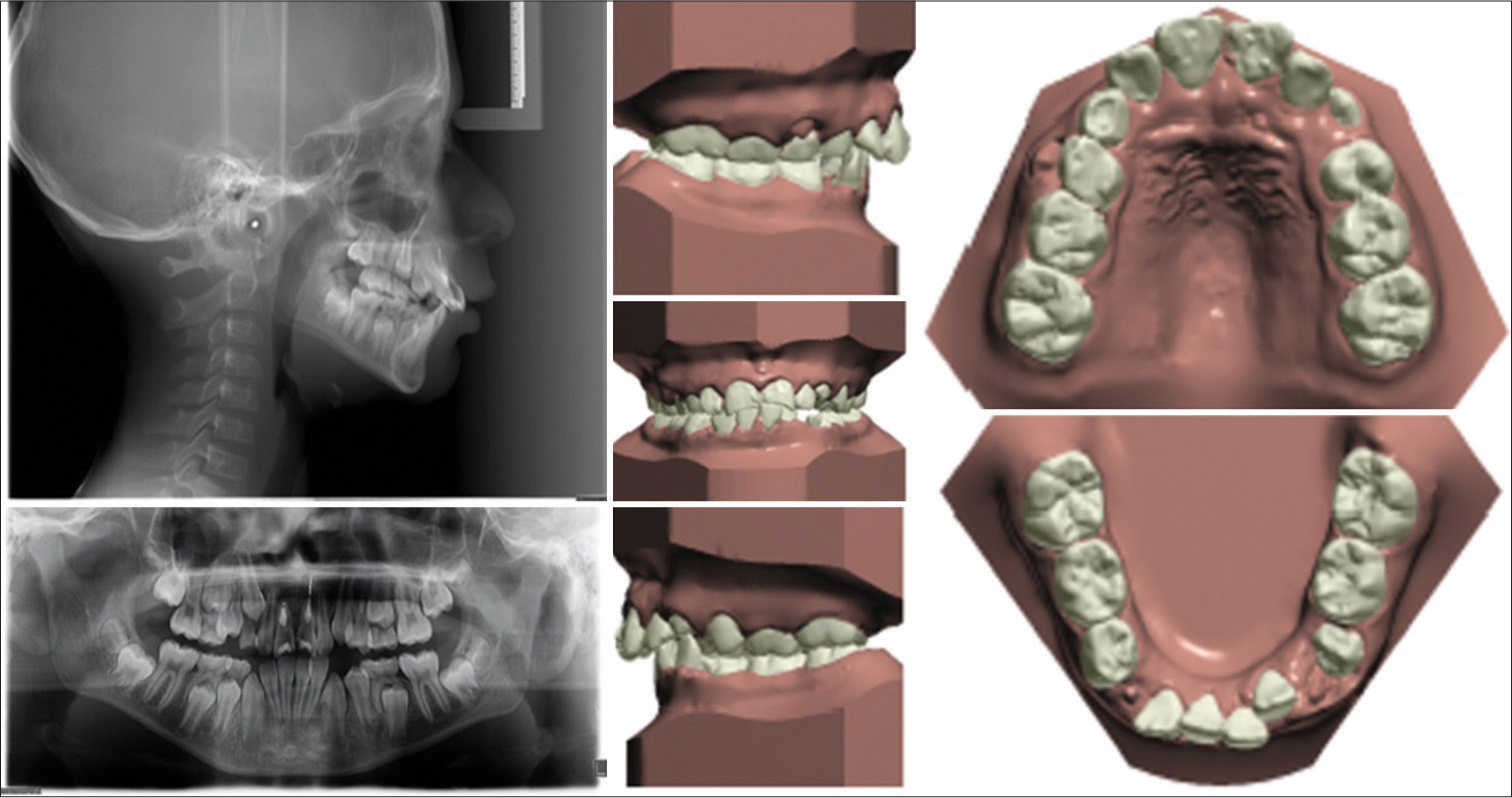
- Pretreatment cephalogram, panoramic radiograph, and study models.
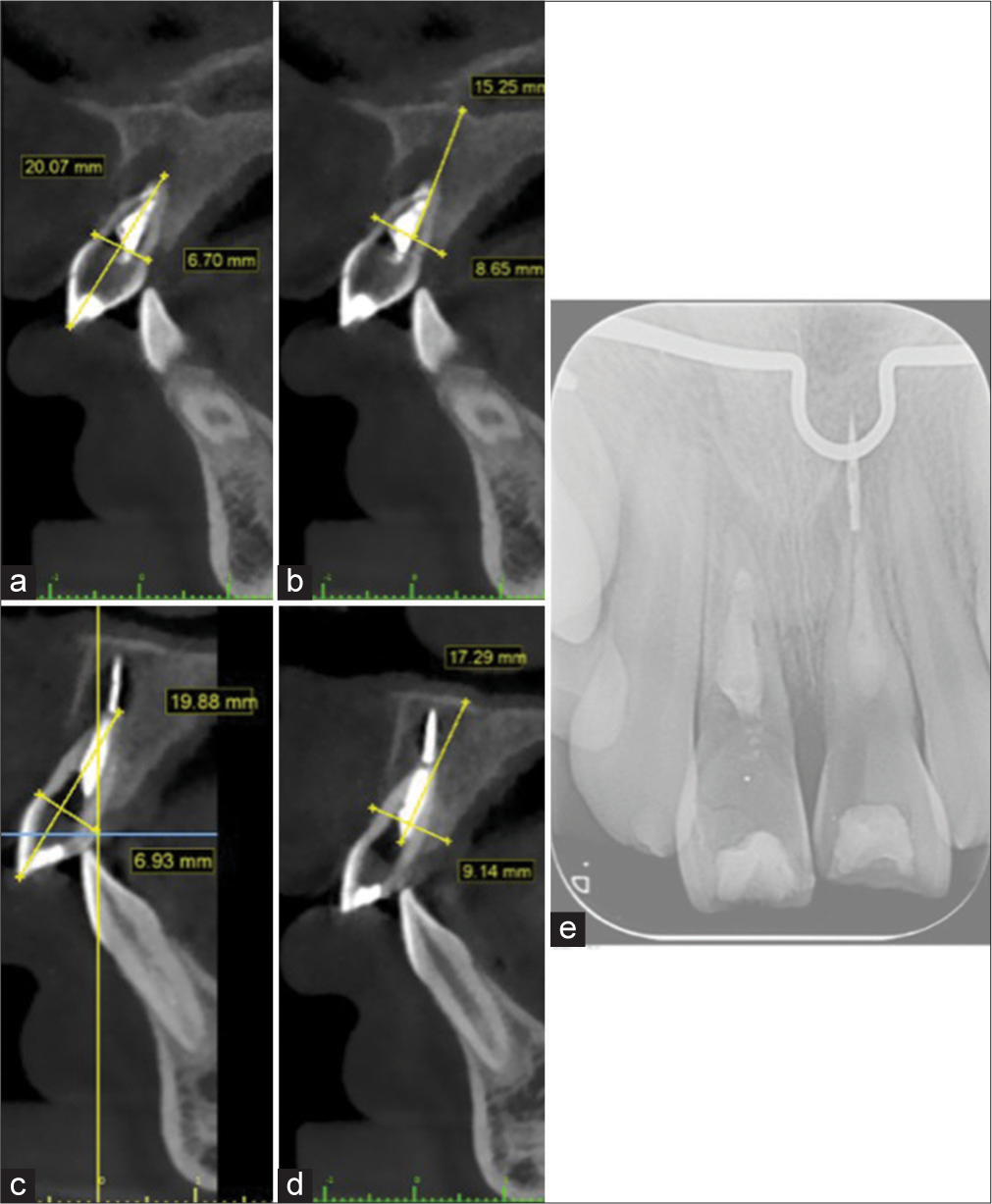
- Sagittal clipping view (a and b) Left maxillary central incisor. (c and d) Right maxillary central incisor. (e) Periapical radiograph. The green lines indicates a reference ruler in milimeters.
Treatment objectives
The treatment objectives for this case were as follows: (1) to achieve better facial balance, (2) to substitute the maxillary central incisors (autotransplantation of maxillary second premolars into the place of maxillary central incisors that needed to be extracted as stated by the endodontist and premolar extractions were needed to solve the orthodontic problems), (3) to achieve a canine Class I, (4) to establish a Class II molar functional relationship, (5) to correct excessive overbite and overjet, (6) to eliminate dental crowding, and (7) to maintain the root length of the teeth.
Treatment alternatives
Various treatment modalities were available for the effective solution of the clinical situation; the presented alternatives presented were as follows: A. Extraction of the poor prognosis maxillary central incisors, orthodontic reposition of maxillary lateral incisors into the extracted maxillary central incisors site, canines eruption guidance, and orthodontic reposition of canines into maxillary lateral incisors site, first bicuspids guidance and orthodontic repositioning into canines site (reshaping of palatal cuspid to avoid occlusal interferences), and guidance and orthodontic repositioning of the second premolars and molars to obtain a Class II functional occlusion. Prosthodontics department consultation to evaluate and restore anterior teeth as recommended. B. Extraction of the poor prognosis maxillary central incisors, extraction of the upper first premolars (required to solve the orthodontic problems) to achieve canine Class I and Class II molar functional relationship, space maintenance of the maxillary central incisors extracted into adulthood, when growth is completed replacement with dental implants.
Treatment progress
Treatment plan was explained to the patient and parents, risks, limitations, and possible complications of orthodontic and surgical procedures were also detailed. The Maxillofacial and Oral Surgery Department extracted the upper maxillary central incisors, upper second primary molars and performed the autotransplantation of the maxillary second premolars into the maxillary central incisors site. A rotated 90° of the autotransplant teeth during surgery was suggested to provide a suitable mesiodistal surface for prosthodontic treatment of the teeth and to resemble the central incisor root anatomy. Unfortunately, a complication occurred, the surgeon positioned the teeth in a labiolingual position (later with orthodontic appliances needed to be corrected). Fertilization was accomplished with a bonded 0.016” × 0.022” SS archwire, including the maxillary lateral incisors and the transplanted second premolars into the upper central incisors site [Figure 4]. The Endodontics Department kept monitoring vitality and had radiographic control every month for six months [Figure 5]. After “greenlight” from the endodontists, the 0.022” × 0.028” McLaughlin, Bennet and Trevisi (MBT) (3M Unitek, Monrovia, CA) appliance was bonded, nickel-titanium (Niti) 0.012” archwires were engaged, and appointments were scheduled every month [Figure 6]. The level and aligning phase was obtained with Niti archwires (0.014”, 0.016”, 0.016” × 0.022” and 0.017” × 0.025”), 0.017” × 0.025” SS archwires were engaged,and a Niti open coil was inserted between the autotransplanted teeth to generate a couple force system using the open coil between the teeth and an elastic chain attached to bonded palatal buttons. Additionally the Niti open coil facilitated the 90° rotation of the autotransplanted teeth, provided a suitable mesiodistal surface for prosthodontic treatment of the teeth and was used to resemble the central incisor root anatomy (condition not fulfilled by the surgical procedure). This mechanics continued for seven months, but unfortunately the treatment was suspended from March 2020 to October 2021 during COVID-19 pandemic. Patient’s assessment after global lockdown showed several missing brackets, no archwires,and relapse of the corrected rotation of the autotransplanted teeth [Figure 7]; Therefore, a panoramic radiograph was taken to check root parallelism, bracket repositioning, and replacement of the missing ones. The following archwires were used in posterior appointments for one month: Niti 0.014” upper and lower, Niti 0.016”, Niti 0.017” × 0.025”, and coordinated upper and lower 0.017” × 0.025” SS. The autotransplanted teeth were rotated 90 degrees by a couple force system using an open coil between the teeth and an elastic chain attached to bonded palatal buttons as described before. Crimpable hooks were attached, and tiebacks activated in the upper arch to close posterior remaining spaces. The prosthodontist made a space assessment before debonding; as this milestone was achieved, the recommended space management, finishing, and detailing was accomplished, and brackets were debonded [Figure 8]. The autotransplanted teeth were restored with the anatomy of maxillary central incisors and the prosthodontist also included the restoration of the maxillary lateral incisors to achieve an optimal esthetic result. A Direct Composite Resin Injection technique was the procedure of choice (Tetric Evoflow A2, Ivoclar Vivadent); as a young patient, a minimal invasive procedure was recommended. Notably, in adulthood a more aggressive indirect restoration can be selected if required. The retention protocol was a bonded fixed retainer to maxillary upper incisors and autotransplanted teeth, plus upper and lower circumferential retainers 24 h a day for six months and later it was only during the night hours.

- Autotransplantation surgery.

- Control cone-beam computed tomography. (a) Sagittal view left maxillary second premolar. (b) Sagittal view right maxillary second premolar. (c) Frontal view. (d) Ferulization.

- Bonded orthodontic appliance MBT 0.022” × 0.028” (3M Unitek).

- Extraoral and intraoral photographs after COVID-19 global lockdown.

- Debonding appointment.
Treatment results
The overall treatment time lasted for seven years., One year and seven months of treatment was interrupted during the COVID-19 pandemic. Facial balance was improved, and the final occlusal relationships were good [Figure 9]. The autotransplantation of the maxillary second premolars into the maxillary central incisors site was successfully accomplished. Autotransplanted teeth showed a positive response to pulp vitality tests, and normal root development continued. The prosthodontic treatment restored the esthetic and function of upper anterior teeth;. The autotransplanted teeth were restored to maxillary central incisor morphology, and lateral incisors were restored to enhance the esthetic and functional outcome. Dental crowding was relieved, and good parallelism of roots was also achieved [Table 1 and Figure 10].

- Posttreatment photographs.

- Post-treatment cephalogram, panoramic radiograph, and study models.
DISCUSSION
Several treatment options are available for growing patients with congenitally missing teeth, including orthodontic closure of the space, replacing the teeth with an implant after growth is completed, fixed prostheses, removable partial dentures, or autotransplantation.[12,18-20]
Autotransplantation protocol is a widely performed and validated treatment alternative. There can be multiple and specific clinical situations where autotransplantation can be performed, but three indications are the most common, they are, multiple agenesis, mandibular second premolar agenesis in hyperdivergent patients and congenitally or traumatically missing maxillary central and lateral incisors as described by Zachrisson.[14,19] High survival success rates are reported when developing teeth, especially premolars are used as donors;[21-24] Another specific clinical situation where autotransplantation should be considered is when two incisors on the cleft side are missing in patients with alveolar clefts.[25]
The stage of the donor root development is one critical factor in determining success after autotransplantation.[14,26] Northway suggested that the preferred stage of root development is between the third and three fourths complete[14,27] and more precise Tsukiboshi suggested that the donor tooth should have at least three-quarters of its root formed and an apical opening more than 1 mm at the time of surgery.[14,28] Other authors recommend an ideal root of the premolar one- half to three-fourths of the final root length.[10,20,29,30] This way, pulp revascularization, and vitality can be preserved, and the tooth retains the potential to erupt and induce alveolar growth.[21,23,31] The donor upper premolars of the case illustrated had three-quarters of their root, ideal length for autotransplantation [Figure 11]. Complete development will not be achieved in all autotransplanted teeth. Total arrest indicates no development after autotransplantation, whereas partial arrest indicates some development,and non-arrest indicates complete development of roots.[14,32-35]

- Cone beam computed tomography sagittal view. (a and b) Right maxillary second premolar axis measurement. (c and d) Left maxillary second premolar long axis measurement. The green lines indicates a reference ruler in millimeters.
Orthodontic forces can be applied to autotransplanted teeth, however, the timing for such treatment is still controversial. Andreasen et al.,[33] Tsukiboshi[28] and Tankittiwat et al. suggest initiating active orthodontic treatment 3–9 months after periodontal healing.[20] Zachrisson et al. and Czochrowska et al. recommend delaying orthodontic treatment until six months after the surgical procedure.[19,20,23,36] Varying degrees of pulp obliteration after autotransplantation of developing teeth is regarded as a normal healing phenomenon and a sign of pulp revascularization and preservation of pulp vitality. Pulp obliteration does not result in an unfavorable prognosis of autotransplanted teeth with developing roots long-term.[23,37-39] Failures such as ankylosis or progressive root resorption of the donor’s tooth are strongly correlated with the damage to the root surface during surgery.[23,40,41]
It is recommended to start orthodontic mechanics of fully developed autotransplanted teeth within 4–8 weeks after surgery.[16,34] Kokai et al. based on a retrospective study suggested that early orthodontic movement may accelerate PDL healing of autotransplanted teeth that have complete root formation.[16,42] However, orthodontic forces are known to result in the root shortening of autotransplanted developing premolars.[16,43] Therefore, delaying orthodontic tooth movement is suggested for autotransplanted teeth until root growth is complete or the apex closed.[16,44] In this case report, orthodontic treatment started six months after the autotransplantation when the endodontist gave the greenlight; root length continued growing to normal size [Figure 10]. The overall treatment time was seven years, including one year and seven months that treatment was interrupted during COVID-19 global lockdown, the patient returned with no archwires, missing brackets, and relapse; the orthodontic rotation to 90° of the autotransplanted premolars due to surgical complication (a rotated 90° of the autotransplanted teeth during surgery was suggested but oral surgeon positioned the teeth in a labiolingual position) lengthened treatment time. Patient’s compliance and motivation were key determinants of treatment success.
Comparing treatment alternatives, orthodontic space closure with movement of teeth toward the midline can be performed successfully with missing maxillary incisors;[45-48] The case reported had the ideal conditions for autotransplantation, so it was discussed as an option and the treatment plan was accepted by the parents. Autotransplantation and implant protocols are effective treatment modalities in the long-term, but periodontal tissues around implants show progressive signs of recession, where the status of periodontal tissues around autotransplanted teeth do not differ from those of natural teeth. In the anterior maxilla natural tooth, substitutions are recommended whenever possible, as stated by Plakwicz et al.[49]
The success of autotransplanted teeth is associated with PDL healing, no root resorption, bone and gingiva healing, and pulp and root development.[19] In Scandinavian countries, autotransplantation of premolars to replace missing incisors is a common method that has been used for over 40 years.[11,50] In recent times, orthodontists around the world are implementing this technique as result of the spread of knowledge, as shown in the orthodontic literature with patient cases from North America, South America, and Asia.
The substitute tooth should have the potential for long-term, even lifelong survival. The replacement should adapt to growth and development changes in the oral region.[22] Multidisciplinary participation is necessary to allow for a functional and esthetic restoration as stated by Zachrisson.[19] Czochrowska et al. demonstrated in a study that autotransplantation of premolars to the maxillary region may be a realistic treatment alternative for replacement of missing maxillary incisors.[23] Therefore, this case report confirms that statement.
CONCLUSION
The success of autotransplantation depends on case selection, well-planned and well-executed treatment, patient compliance and biological factors such as the age of the patient, stage of the root development of the donor tooth, surgical factors such as the amount of trauma perceived by the PDL of the donor tooth, surgical technique and meticulous management of soft and hard tissues, splinting method, monitoring healing process, and good timing and proper orthodontic tooth movement.
This case report demonstrates that autotransplantation of developing premolars in children has high survival and successful outcome. This treatment modality offers the patient great short-term as well as long-term esthetic and functional outcomes.
Acknowledgments
We thank the collaboration of Professor Luis Celis, at the time chairman of the Prosthodontics Department for being part of the team involved in the patient treatment. Professor Ricardo González-Plata for the patient referral, Professor Raymundo Ramirez Lugo for performing the surgical procedure and residents César Garrigós and Humberto Fosado who were also part of the orthodontic team.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Epidemiology of traumatic dental injuries. J Endod. 2013;39:S2-5.
- [CrossRef] [PubMed] [Google Scholar]
- Traumatic dental injuries, treatment, and complications in children and adolescents: A register-based study. Eur J Dent. 2021;15:557-62.
- [CrossRef] [PubMed] [Google Scholar]
- Aetiology and risk factors related to traumatic dental injuries--a review of the literature. Dent Traumatol. 2009;25:19-31.
- [CrossRef] [PubMed] [Google Scholar]
- Children's dental health in the United Kingdom 1993 London, UK: Her Majesty's Stationery Office; 1994.
- [Google Scholar]
- Epidemiology of traumatic dental injuries--a 12 year review of the literature. Dent Traumatol. 2008;24:603-11.
- [CrossRef] [PubMed] [Google Scholar]
- World traumatic dental injury prevalence and incidence, a meta-analysis-one billion living people have had traumatic dental injuries. Dent Traumatol. 2018;34:71-86.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiology of traumatic dental injuries to primary and permanent teeth in a Danish population sample. Int J Oral Surg. 1972;1:235-9.
- [CrossRef] [PubMed] [Google Scholar]
- Incidence of dental trauma in the Western Australian school dental service. Community Dent Oral Epidemiology. 1988;16:294-8.
- [CrossRef] [PubMed] [Google Scholar]
- Dental autotransplantation as a alternative treatment for the loss of permanent anterior teeth in children. Dental Press J Orthod. 2022;27:e22spe4.
- [CrossRef] [PubMed] [Google Scholar]
- Autotransplantation of teeth in cases with agenesis or traumatic loss of maxillary incisors. Eur J Orthod. 1991;13:486-92.
- [CrossRef] [PubMed] [Google Scholar]
- Premolar transplantation to replace a missing central incisor. Am J Orthod Dentofacial Orthop. 2015;147:394-401.
- [CrossRef] [PubMed] [Google Scholar]
- Tooth autotransplantation as a treatment option: A review. J Clin Pediatr Dent. 2010;35:129-35.
- [CrossRef] [PubMed] [Google Scholar]
- Autotransplantation of premolars in a patient with multiple congenitally missing teeth. J Clin Orthod. 2011;45:399-407.
- [Google Scholar]
- Multiple congenitally missing teeth treated with autotransplantation and orthodontics. Am J Orthod Dentofacial Orthop. 2012;141:641-51.
- [CrossRef] [PubMed] [Google Scholar]
- Autotransplantation of a fully developed maxillary premolar to a missing mandibular premolar site. J Clin Orthod. 2013;47:199-206.
- [Google Scholar]
- Autotransplanted premolars with incomplete root formation in a growing patient with multiple missing teeth. Am J Orthod Dentofacial Orthop. 2020;158:587-98.
- [CrossRef] [PubMed] [Google Scholar]
- Autotransplantation: A viable treatment option for adolescent patients with significantly compromised teeth. Aust Dent J. 2016;61:396-407.
- [CrossRef] [PubMed] [Google Scholar]
- Management of missing maxillary anterior teeth with emphasis on autotransplantation. Am J Orthod Dentofacial Orthop. 2004;126:284-8.
- [CrossRef] [PubMed] [Google Scholar]
- Planning esthetic treatment after avulsion of maxillary incisors. J Am Dent Assoc. 2008;139:1484-90.
- [CrossRef] [PubMed] [Google Scholar]
- Mandibular premolar transplantation to replace missing maxillary anterior teeth: A multidisciplinary approach. Am J Orthod Dentofacial Orthop. 2021;160:459-72.
- [CrossRef] [PubMed] [Google Scholar]
- Applicability of autotransplantation in cases of missing upper anterior teeth. Am J Orthod. 1978;74:410-21.
- [CrossRef] [PubMed] [Google Scholar]
- Outcome of tooth transplantation: Survival and success rates 17-41 years post-treatment. Am J Orthod Dentofacial Orthop. 2002;121:110-9.
- [CrossRef] [PubMed] [Google Scholar]
- Autotransplantation of premolars to replace maxillary incisors: A comparison with natural incisors. Am J Orthod Dentofacial Orthop. 2000;118:592-600.
- [CrossRef] [PubMed] [Google Scholar]
- Survival and success rates of autotransplanted premolars: A prospective study of the protocol for developing teeth. Am J Orthod Dentofacial Orthop. 2013;144:229-37.
- [CrossRef] [PubMed] [Google Scholar]
- Nonprosthodontic management of alveolar clefts with 2 incisors missing on the cleft side: A report of 5 patients. Am J Orthod Dentofacial Orthop. 2002;122:587-92.
- [CrossRef] [PubMed] [Google Scholar]
- Resorption of autotransplanted human teeth: A retrospective study of 291 transplantations over a period of 25 years. Int Endod J. 1985;18:119-31.
- [CrossRef] [PubMed] [Google Scholar]
- Autogenic dental transplants. Am J Orthod Dentofacial Orthop. 2002;121:592-3.
- [CrossRef] [PubMed] [Google Scholar]
- Autotransplantation of teeth: Requirements for predictable success. Dent Traumatol. 2002;18:157-80.
- [CrossRef] [PubMed] [Google Scholar]
- Autotransplantation of teeth with incomplete root formation: A systematic review and meta-analysis. Clin Oral Investig. 2018;22:1613-24.
- [CrossRef] [PubMed] [Google Scholar]
- Dental auto-transplantation to anterior maxillary sites. Dent Traumatol. 2011;27:23-9.
- [CrossRef] [PubMed] [Google Scholar]
- Induction of jaw bone formation by tooth autotransplantation. Nor Tannlaegeforenings Tid. 1978;88:319-22.
- [Google Scholar]
- A long-term study of 370 autotransplanted premolars. Part I Surgical procedures and standardized techniques for monitoring healing. Eur J Orthod. 1990;12:3-13.
- [CrossRef] [PubMed] [Google Scholar]
- A long-term study of 370 autotransplanted premolars. Part II Tooth survival and pulp healing subsequent to transplantation. Eur J Orthod. 1990;12:14-24.
- [CrossRef] [PubMed] [Google Scholar]
- A long-term study of 370 autotransplanted premolars. Part III Periodontal healing subsequent to transplantation. Eur J Orthod. 1990;12:25-37.
- [CrossRef] [PubMed] [Google Scholar]
- A long-term study of 370 autotransplanted premolars. Part IV Root development subsequent to transplantation. Eur J Orthod. 1990;12:38-50.
- [CrossRef] [PubMed] [Google Scholar]
- The esthetic outcome of autotransplanted premolars replacing maxillary incisors. Dent Traumatol. 2002;18:237-45.
- [CrossRef] [PubMed] [Google Scholar]
- Autotransplantation of premolars with partly formed roots. A radiographic study of root growth. Am J Orthod. 1974;66:355-66.
- [CrossRef] [PubMed] [Google Scholar]
- Indications for autotransplantation in cases of missing premolars. Am J Orthod. 1978;74:241-57.
- [CrossRef] [PubMed] [Google Scholar]
- Autotransplantation and healing. Am J Orthod Dentofacial Orthop. 2019;156:299-300.
- [CrossRef] [PubMed] [Google Scholar]
- Eruption of premolars subsequent to autotransplantation. A longitudinal radiographic study. Eur J Orthod. 1998;20:45-55.
- [CrossRef] [PubMed] [Google Scholar]
- The effect of limited drying or removal of the periodontal ligament. Periodontal healing after replantation of mature permanent incisors in monkeys. Acta Odontol Scand. 1981;39:1-13.
- [CrossRef] [PubMed] [Google Scholar]
- Retrospective study of 100 autotransplanted teeth with complete root formation and subsequent orthodontic treatment. Am J Orthod Dentofacial Orthop. 2015;148:982-9.
- [CrossRef] [PubMed] [Google Scholar]
- Influence of orthodontic treatment on root development of autotransplanted premolars. Am J Orthod. 1986;89:146-50.
- [CrossRef] [PubMed] [Google Scholar]
- Recognizing and correcting developing malocclusions: A problem-oriented approach to orthodontics. (1st ed). Hoboken: Wiley-Blackwell; 2016.
- [CrossRef] [Google Scholar]
- Outcome of orthodontic space closure with a missing maxillary central incisor. Am J Orthod Dentofacial Orthop. 2003;123:597-603.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontic treatment using canines in place of missing maxillary lateral incisors. Am J Orthod. 1970;58:109-27.
- [CrossRef] [PubMed] [Google Scholar]
- Improving orthodontic results in cases with maxillary incisors missing. Am J Orthod. 1978;73:274-89.
- [CrossRef] [PubMed] [Google Scholar]
- Bilateral congenital absence of maxillary lateral incisors: A craniofacial and dental cast analysis. Am J Orthod. 1985;87:280-93.
- [CrossRef] [PubMed] [Google Scholar]
- Transplant vs implant in a patient with agenesis of both maxillary lateral incisors: A 9-year follow-up. Am J Orthod Dentofacial Orthop. 2016;149:751-6.
- [CrossRef] [PubMed] [Google Scholar]
- Autotransplantion of a displaced mandibular second premolar to its normal position. Am J Orthod Dentofacial Orthop. 2013;143:274-80.
- [CrossRef] [PubMed] [Google Scholar]




