

Translate this page into:
Class II and anterior open bite malocclusion treated with mini-implants, intermaxillary elastics, speech therapy, and retained with a night-wear palatal crib wraparound


*Corresponding author: Fernando Martinelli, Rua Mariante, 239/306, Porto Alegre, RS, Brazil, 90430-181, Porto Alegre, Brazil. fernando.martinelli74@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Martinelli F. Class II and anterior open bite malocclusion treated with mini-implants, intermaxillary elastics, speech therapy, and retained with a night-wear palatal crib wraparound. APOS Trends Orthod 2023;13:123-32.
Abstract
The teeth position in anterior open bite malocclusion depends on a balance of pressure between the tongue and lips and the treatment planning should include such variables. The objective of this study was to report an orthodontic case of an adult with maxillary protrusion and anterior open bite treated with skeletal anchorage and intermaxillary elastics. The patient presented a Class II malocclusion with anterior open bite, without a history of non-nutritive habits, and mandibular missing teeth at 54 years old. Mini-implants were inserted in the maxillary molars region to produce distal movement of the maxillary dentition while controlling molar extrusion, and in the mandibular anterior region on the left side to produce mesial movement of posterior teeth. Up and down intermaxillary elastics were worn in the area of the incisors to treat the open bite together with Class II intermaxillary elastics. Cleats were bonded in the lingual surface of the anterior teeth as spurs to the tongue posture. However, the best result on the anterior open bite treatment was coincident with the speech therapy. Normal relationships between the maxillary and mandibular occlusal plane of cusps, correct anterior overbite, and adequate proximal relationships were obtained at the end of treatment. The retention modality to the maxillary arch was daily wear of a removable standard wraparound and a night-time wraparound with the palatal crib. The new technology allows for more effective treatment in adults and speech therapy was helpful to achieve balanced pressure between the tongue and lips.
Keywords
Retraction
Anchorage
Neuromuscular
Anterior open bite

INTRODUCTION
Open bite malocclusions can be self-corrected by eliminating sucking habits before children begin the school period.[1] If this malocclusion persists until the permanent dentition, the position of teeth will depend on a balance of pressure between the tongue and lips, specially, in the rest.[1] The traditional concept that tongue thrust and swallow reverse would cause anterior open bite is no longer up-to-date. In addition, the patients with hyperdivergent mandibular plane provide further difficulties,[2] due to the masticatory muscle’s power.[2,3] One important reason to treat an anterior open bite is that the tongue interposition in the incisors increases the risk of root resorption.[4]
In adults, the severity of the open bite is considered to decide between treatment with orthodontic movement or with surgical operation to improve anatomical relationships.[1] On average, there are greater improvements and stability after maxillary surgery than mandibular.[5]
Significant relapse in the open bite is found in non-extraction treatments, contrasting with non-significant relapse occurring in extraction cases.[6] The applications of titanium mini plates for skeletal anchorage were spread to the intrusion of posterior teeth in severe cases of open bite.[7] Elastic threads are the source of orthodontic force to intrude the maxillary and mandibular molars in about 3 mm and no serious side-effects are produced.[7] This way the gingiva display in the incisors is better controlled. Although this is not the only treatment option to correct the open bite, true molar intrusion can be achieved without accurate quantification.[8] Most relapse occurs in the 1st years post-treatment, indicating that the application of an adequate retention modality is needed.[9]
In adults, mini-implants for skeletal anchorage have been an effective new technology to treat Class II malocclusions too.[10,11] Intermaxillary elastics are a mechanic alternative to correct the occlusal relationship between the maxillary and mandibular arch in Class II and open bite malocclusions.[12,13]
Associated with all these mechanical devices and opportunities, oral motor skills must be seriously considered to achieve normal occlusion with stability.[14] The objective of this study was to report an orthodontic case of an adult with Class II, anterior open bite, mutilated teeth, and ankylozed mandibular incisor treated with mini-implants, intermaxillary elastics, and speech therapy.
CASE REPORT
Diagnosis and etiology
An adult woman at 54 years old presented to orthodontic treatment with a chief complaint of correcting the anterior open bite. On the clinical examination, spontaneous lip sealing, with harmonic profile and lips position was observed together with a curved smile resulting from the open bite [Figure 1]. The patient presented a Class II malocclusion with an anterior open bite (5 mm), mandibular missing teeth, extensive restorations, and localized spaces in the mandibular arch [Figure 1]. An exaggerated curve of Spee was detected in the maxillary arch [Figures 1 and 2]. As the treatment progressed, an ankylosed mandibular central incisor was diagnosed.

- Initial facial and intra-oral photographs.

- Initial dental casts treatment records.
The analysis of the cephalometric radiograph confirmed the anterior open bite, increased overjet and the molars in a super Class II relationship, besides with well-developed upper airways [Figure 3]. The cephalogram revealed normal measures, on average, except for the hyper-divergent (GoGnSN 39°) mandibular plane [Figure 3 and Table 1].
| Cephalometry | Pre-treatment | Post-treatment |
|---|---|---|
| SNA (o) | 82.0 | 86.0 |
| SNB (o) | 78.0 | 80.0 |
| ANB (o) | 4.0 | 6.0 |
| GoGnSN ((o) | 39.0 | 39.0 |
| 1.NA (o) | 22.0 | 3.0 |
| 1-NA (mm) | 6.0 | 0.0 |
| 1.NB (o) | 26.0 | 29.0 |
| 1-NB (mm) | 6.0 | 5.0 |
| 1.1 (o) | 129.0 | 143.0 |
| FMA (o) | 33.0 | 36.0 |
| FMIA (o) | 60.0 | 54.0 |
| IMPA (o) | 87.0 | 90.0 |

- Initial lateral cephalogram and tracing.
In the panoramic radiograph, the mandibular right premolars roots were distant from each other, the mandibular left canine was missing. On the left side, there was a prosthetic bridge at unit 35 and a cantilever at element 33 [Figure 4]. Serial endodontic treatments in the mandibular incisors and composite interproximal restorations in the maxillary incisors were detected, along with endodontic treatment in the maxillary lateral incisors [Figure 4].

- Initial (above) and final (below) panoramic radiographs.
The patient reported a car traffic incident, resulting in a broken mandible and fracturing of maxillary and mandibular incisors. However, she did not report nonnutritive and thumb-sucking habits since the infant ages. Probably, the etiology of the open bite was the tongue interposition in the speech and at rest associated with the hyperdivergent mandibular plane. The resting posture of the tongue and lips is an important etiologic factor in the open bite.[1] The unbalance between opposing pressures of tongue and lips were occurring in the lingual interposition, noted in the speech, rather than by respiratory requirements. The etiology of Class II might have been due to genetic inheritance. Genetic characteristics tend to recur, from either parent or a combination of traits from both parents.[15] In monozygotic twins, there is an overall concordance of having a Class II malocclusion in 68% of cases, contrasting with a concordance of 100% of monozygotic twins having an open bite.[15] Besides that, the etiology of the missing mandibular left canine, the ankylosed mandibular left central incisor, and flattened incisal boards was the car traffic incident. Favorably, no symptoms of the disease were found in the temporomandibular joint.
Speech therapeutic analysis
An anterior lisp of the tongue was diagnosed, characterizing an important anterior projection of the tongue in speech. Although the tongue presented normal morphology, anatomy, and mobility, it was producing unbalanced pressure on the maxillary incisors. Based on this assessment, speech therapy was indicated. Exercises with the tongue were instructed and controlled every 2 weeks in the beginning. After 6 months of speech therapy, consultations were followed once a month until the brain-supported motor skill automation at resting posture.
Treatment objectives
In the maxillary dentition, the initial objective was leveling the curve of Spee with rectangular wires and a slight molar intrusion. This way the open bite was partially corrected, preventing an undesirable gummy smile. The second objective was to promote the distal movement of a maxillary molar, allowing for complete retraction of the maxillary dentition. As the maxillary incisors were retracted and the overjet reduced, the open bite was further corrected.
In the mandibular arch, the main objective was to produce mesial movement of the molars to close anterior spacing on the right side. The second objective was to align the mandibular incisors and establish protrusive excursion and canine guidance. For this reason, a restorative implant was planned to replace the missing mandibular left canine. The planning included no modifications in the fixed prosthesis bridging the area of mandibular premolars on the left side, at least, for the orthodontic objectives.
Even more than, esthetics and function the treatment’s main objective was the normal relationship between maxillary and mandibular dentitions, and between the tooth units within each dental arch. Acquiring normal oral motricity in the speech and balance pressure at rest were other treatment objectives, in respect of requirements for treatment stability.
Treatment alternatives
Complete fixed appliances with mini-implants in the maxillary arch to level the curve of Spee, while retaining excessive eruption of posterior teeth, and promoting the distal movement of molars. Afterward, changing the mini-implant’s position to distalize the remaining dentition. Mini-implants were inserted in the anterior mandibular arch to produce mesial movement of right posterior teeth and wearing intermaxillary elastics to obtain correct overbite and stabilize the Class II correction. Application of restorative implant in the mandibular left canine area
Complete fixed appliances and correct the Class II and anterior open bite with intermaxillary elastics. The remaining spaces in the mandibular arch closed with an elastomeric chain and applying restorative implants in both sides
Complete fixed appliances and extraction of maxillary first premolars to allow correcting the Class II malocclusion, and vertical intermaxillary elastics to obtain correct overbite. Application of one restorative implant on each side of the mandibular arch.
The first option was followed because the skeletal anchorage is safer to attain the planned movement and the normal occlusion would be established with natural teeth. The second option has a risk of losing control of the orthodontic mechanics, due to the great amount of movement to be accomplished with intermaxillary elastics. The third option had the risk of maxillary incisors over-retraction and it may get worse lips position, which was normal at the beginning of treatment.
Treatment progress
A complete standard edgewise appliance (0.022 × 0.028) was bonded on both, maxillary and mandibular, arches. Mini-implants (1.5 mm in diameter) were placed in the interradicular alveolar space and within the attached gingival area mesial to the maxillary first molars and distal to the mandibular right canine.
The maxillary mini-implants were primarily used to anchor the molar intrusion along the leveling of the curve of Spee. The initial archwire was a coaxial 0.0155”, followed by a rounded 0.016” stainless steel archwire and a rectangular archwire. At this stage, the forces anchored in the maxillary mini-implants were changed into a distal vector. The force was produced by an elastomeric chain (200 gf) and mediated by a sliding jig, from the distal of the maxillary canines to the mesial of molars [Figure 5]. This force system was the same until obtaining 4 or 5 mm in distance between the maxillary first molars and the second premolars. At this time, the sliding jig was removed and a compression coil spring was placed between the maxillary first molars and second premolars without resultant force, to maintain the distance for the next movement. The archwire was adjusted to increase the interradicular distance between the maxillary first and second molars. A tip back was bent in the first and a tip forward in the maxillary second molars. This way the risk of mini-implant loss was minimized because the root proximity comprises a risk of mobility and loss.[16] As this premise was reached, the mini implants were relocated to the attached gingiva between the maxillary first and second molars. The mini-implants were therefore used to anchor the retraction of the anterior maxillary segment after removing the springs mesial to molars.

- Diagram illustrating the system of force to the molars distal movement anchored on mini-implants, associated with sliding jig and elastomeric chain.
In the mandibular arch, a restorative implant insertion in the left canine area was recommended and performed by the general dentist. The sequence of archwires was a coaxial wire “0.0155 and a rounded “0.016 wire was maintained and readjusted until achieving correct alignment of the mandibular incisors when a rectangular archwire was placed. Although the mandibular left central incisor expressed some mobility, sufficient alignment was not achieved with the continuous arches. Thus, a binary system of force was applied by using an elastomeric chain in the lingual cleats anchored in the continuous arch [Figure 6]. Probably, there was partial ankylosis in this tooth, which was positioned as aligned as possible at the end of treatment. On the right side, the anterior mini-implant was the anchorage to move forward the molars with an elastomeric chain [Figure 4].

- System of force to produce mesial movement of the mandibular posterior segment with a mini-implant and elastomeric chain; and the intermaxillary elastics to correct the Class II and anterior open bite.
Intermaxillary elastics (100 gf, nonlatex 3/16 medium) were employed full-time wear for 15 months to close the open bite anchored in compression hooks attached in the rectangular wires between maxillary central and lateral incisors, and between mandibular lateral incisors and canines in both sides [Figure 6]. This system of force was insufficient to attain normal overbite. Active cleats were bonded as tongue spurs in the lingual surface of the mandibular canine and incisors [Figure 6] to stimulate a balanced position of the tongue in direction of the papilla incisive. However, this attempt did not reach successful changes in the open bite and a speech therapist was consulted. The treatment was followed and coincided with desirable improvements in the overbite. When the open bite was corrected, the elastics were removed gradually: Two months with nighttime wear and 2 months alternating elastics wearing one night and without elastics in the other [Figure 7].

- Facial analysis and the edgewise system in the treatment finishing.
Class II intermaxillary elastics (200 gf,[17] nonlatex 3/16 medium) were applied full-time wear for 1 year and anchored on movable compression hooks attached in the mesial of maxillary canines and the tubes of terminal mandibular molars [Figure 4]. As the elastic force was activated that the movable hooks dislocated in a distal direction, similar to a sliding jig [Figure 4]. At this time, the maxillary mini-implants were removed to allow the improvement of teeth position and the occlusal relationships between the antagonist archs. The mandibular mini-implant was removed when the premolars were closely approximated.
All the intermaxillary elastics were removed 2 months before debonding and the overall treatment time was 30 months. After debonding appliances, fixed lingual retention was bonded in the mandibular arch, while removable wraparound retention was applied full-time for 1 year with nighttime wear of the palatal crib.
RESULTS
The post-treatment images revealed that lips and facial muscles remained balanced, while the smile was greatly improved in the facial assemblies [Figure 8]. The anterior open bite was corrected and the normal overbite was reached [Figures 8 and 9]. Normal anteroposterior relationship of the occlusal inclined planes of teeth was obtained as well [Figures 8 and 9], except for the area with a fixed prosthetic restoration bridging the premolars on the left side [Figure 9]. Ideally, a new prosthesis should be made to provide adaptation to the new occlusal relations. Canines’ guidance and the anterior excursion were established.

- Final treatment facial and intra-oral photographs.

- Final treatment dental casts.
In the maxillary arch, the curve of Spee was normalized to increase the overbite. The maxillary dentition was moved distally [Figure 9] and the incisors were inclined lingually toward the mandibular incisors [Figure 10]. In the mandibular arch, the posterior teeth at the right side moved forward and the spaces were closed. The incisors were as aligned as possible due to the ankylosis in the left central incisor [Figure 8].

- Final treatment lateral cephalogram and tracing.
The maxillary incisors protrusion (1. NA and 1-NA) was 3°and 0 mm [Table 1] and the molars were in key of occlusion in the post-treatment cephalogram [Figure 10]. The mandibular incisor protrusion (1.NB and 1-NB) and the lips protrusion (S-line) did not change with treatment [Figure 10]. The modality of retention in the maxillary arch included a standard removable wraparound plate for daytime wear and a modified wraparound with a palatal crib and a relief in the acrylic plate for night-time wear [Figure 11]. No occlusal retention was planned for the intrusion of about 1 mm in the maxillary molars demonstrated at the superimposition (SN), [Figure 12]. The results for the open bite treatment were stable 2 years post-treatment [Figure 13].

- (a) The removable wraparound retention, in the maxillary arch, (b) for day-time wearing and (c) modified with palatal crib and palatal relief in the acrylic plate to the night-time wearing.
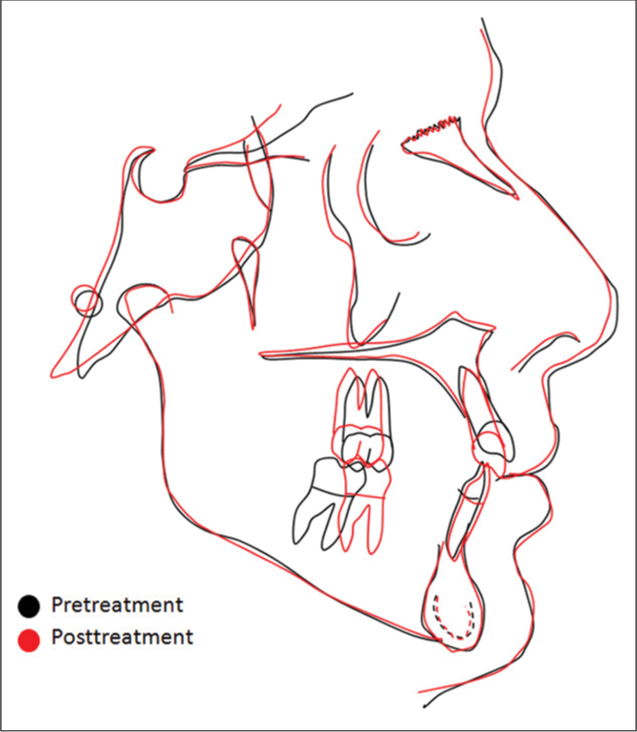
- Superimposition between the pre- and post-treatment cephalometric tracings.

- Intraoral photographs in the 2 years post-treatment record.
DISCUSSION
Even more than the biomechanics planned with mini-implants and intermaxillary elastics, speech therapy was essential for correcting the anterior open bite. Great improvement was noted in the oral motor skills of the patient’s speech. It has been reported that sleep is necessary to the brain supporting motor skill consolidation.[18] This is the basis to employ a night-time palatal crib at the removable wraparound retention.
A different night-time modality of retention to the treatment of anterior open bite cases has been reported, by employing a posterior bite plane.[19] The anterior open bite treated with skeletal anchorage to molars intrusion presented a 10.20% of relapse in the 1st year and remained relatively stable 4 years after.[19] 2-year-post-treatment stability has been reported by the use of a modified spur-implanted Essix retainer, after traditional non-surgical orthodontic treatment.[20]
In the present case report, mini-implants were applied in the maxillary to prevent over-eruption of the posterior segment and producing distal forces to treat the Class II malocclusion. In addition to the system of force based on mini-implants, Class II intermaxillary elastics were used. Movable hooks were attached mesial to the maxillary canines and turned in an occlusal direction [Figure 6], to work as jigs. This allows the application of distal force in the canines, rather than in the incisors, with minimal extrusion vector.[13]
In severe cases, orthognathic surgeries are useful to overcome difficulties in the treatment of anterior open bites in adults. Accurately planned on CBCT imaging, a 3-piece LeFort maxillary advancement osteotomy with differential impaction and bilateral sagittal mandibular split osteotomy (to correct the open bite, mandibular asymmetry, and midline shift) was applied to treat a Class III with anterior open bite.[21] A speech pathologist was consulted in association with the 2-jaw surgery.[21] Conversely, a twice relapsed anterior open bite is reported after traditional orthodontic treatment in adolescence and some years later, with other professionals from another country, when the orthodontics was combined with a LeFort maxillary impaction and a mandibular bilateral sagittal split osteotomy (for mandibular advancement).[22] In the definite orthodontic treatment, the skeletal anchorage was applied to the intrusion of the maxillary teeth from decreasing gummy smiles in association with a 6-month myofunctional therapy program to improve tongue posture.[22]
Mini-plates make it possible to achieve the exact treatment goals with simplified biomechanics, by the intrusion of the maxillary and mandibular molars and consequent counterclockwise rotation of the occlusal plane.[7,23] This way, the overbite increases significantly too with posterior segment intrusion.[23] Mini-implants and intermaxillary elastics have been effective to treat Class II cases with an anterior open bite in association with the premolar extraction.[24] When mini-implant failure has been experienced to the intrusion of the maxillary molars in adolescents, the high-pull headgear is successfully employed, together with lingual cleats working as habit spurs to control tongue thrusting.[25]
The speech therapy appeared to be very important to accomplish the treatment planning in the present case, as well as, the night-wear retention with a palatal crib. However, randomized clinical trials[26] or well-designed prospective studies with an adequate control group and sample selection are necessary to support the advantages of specific treatment and retention modalities.[26,27] The available scientific database on the stability of open bite treatment does not strongly support advantageous clinical choices to obtain treatment stability.[26] Although vertical relapse has been experienced in a certain number of cases after surgical treatment, regardless of the type of orthognathic surgery,[27] This approach may allow for improved facial esthetics as dentofacial deformities were corrected.[26] On the other hand, the treatment effectiveness of Class II malocclusion is already well-recognized.[28]
CONCLUSION
The treatment of Class II and anterior open bite malocclusions in adults had advanced by the applications of the mini-implants, as far as, extractions and part of orthognathic surgeries can be avoided. The biomechanics of intermaxillary elastics should be carefully planned to prevent undesirable canine extrusion or over-duty on the incisors. However, the stability of a treated anterior open bite is still a challenge due to the neuromuscular environmental etiology. Because the teeth’s position depends upon the balance of pressure between the tongue and lips in the rest, a night-wear modality of retention must be seriously considered, as well as, speech therapy.
Acknowledgment
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Surgical Correction of Dentofacial Deformities Philadelphia, PA: WB Saunders; 1980.
- [Google Scholar]
- The influence of growth pattern in open bite correction. Rev Bras Odontol. 2005;62:177-79.
- [Google Scholar]
- Mandibular muscle morphology in children with different vertical facial patterns: A 3-dimensional computed tomography study. Am J Orthod Dentofacial Orthop. 2008;133:10.e1-13.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontics In: Current Principles and Techniques (4th ed). St Louis, Mo, USA: Elsevier Inc; 2005.
- [Google Scholar]
- A comparison of Class II open bite correction by maxillary or mandibular surgery. Am J Orthod Dentofacial Orthop. 2020;157:631-40.
- [CrossRef] [PubMed] [Google Scholar]
- Stability of anterior open bite in permanent dentition treated using extraction or non-extraction methods: A systematic review and meta-analysis of each method. Orthod Waves. 2019;78:1-10.
- [CrossRef] [Google Scholar]
- Skeletal anchorage system for open-bite correction. Am J Orthod Dentofacial Orthop. 1999;115:166-74.
- [CrossRef] [PubMed] [Google Scholar]
- True molar intrusion attained during orthodontic treatment: A systematic review. Am J Orthod Dentofacial Orthop. 2006;130:709-14.
- [CrossRef] [PubMed] [Google Scholar]
- Long-term stability of anterior open-bite treatment by intrusion of maxillary posterior teeth. Am J Orthod Dentofacial Orthop. 2010;138:396.e1-9.
- [CrossRef] [PubMed] [Google Scholar]
- Nonsurgical treatment of severe Class II malocclusion with anterior open bite using mini-implants and maxillary lateral incisor and mandibular first molar extraction. Am J Orthod Dentofacial Orthop. 2017;151:964-77.
- [CrossRef] [PubMed] [Google Scholar]
- Anatomic variability in alveolar sites for skeletal anchorage. Am J Orthod Dentofacial Orthop. 2010;138:252-e1-9. discussion 252-3
- [CrossRef] [PubMed] [Google Scholar]
- Three-dimensional evaluation of open-bite patients treated with anterior elastics and curved archwires. Am J Orthod Dentofacial Orthop. 2018;154:693-701.
- [CrossRef] [PubMed] [Google Scholar]
- Correction of anterior open bite deformity: A study of tongue function, speech changes, and stability. J Maxillofac Surg. 1976;4:93-101.
- [CrossRef] [PubMed] [Google Scholar]
- Class II malocclusion: Diagnostic and clinical considerations with and without treatment. Semin Orthod. 2006;11:11-24.
- [CrossRef] [Google Scholar]
- Root proximity is a major factor for screw failure in orthodontic anchorage. Am J Orthod Dentofacial Orthop. 2007;131:S68-73.
- [CrossRef] [PubMed] [Google Scholar]
- Technique and Treatment with Light-wire Edgewise Appliances (2nd ed). St Louis: Mosby Co; 1972.
- [Google Scholar]
- Sleep spindles: A physiological marker of age-related changes in gray matter in brain regions supporting motor skill memory consolidation. Neurobiol Aging. 2017;49:154-64.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of long-term stability of skeletal anterior open bite correction in adults treated with maxillary posterior segment intrusion using zygomatic miniplates. Am J Orthod Dentofacial Orthop. 2016;150:78-88.
- [CrossRef] [PubMed] [Google Scholar]
- A new type of modified Essix retainer for anterior open bite retention. Prog Orthod. 2010;11:45-52.
- [CrossRef] [PubMed] [Google Scholar]
- Anterior open bite correction with 2-jaw orthognathic surgery. Am J Orthod Dentofacial Orthop. 2019;155:108-16.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of a twice-relapsed anterior open bite using temporary anchorage devices, myofunctional therapy, and fixed passive self-ligated appliances. Am J Orthod Dentofacial Orthop. 2020;157:832-42.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of anterior open bite in patients treated with maxillary posterior segment intrusion using zygomatic anchorage. Am J Orthod Dentofacial Orthop. 2020;158:547-54.
- [CrossRef] [PubMed] [Google Scholar]
- Mini-implants for the treatment of severe Class II division 1 with anterior open bite and tongue thrusting habit. Orthod Waves. 2011;70:71-9.
- [CrossRef] [Google Scholar]
- Camouflage of a high-angle skeletal Class II open-bite malocclusion in an adult after mini-implant failure during treatment. Am J Orthod Dentofacial Orthop. 2017;151:583-97.
- [CrossRef] [PubMed] [Google Scholar]
- Stability of open bite treatment in adult patients: A systematic review. J World Fed Orthod. 2012;1:e97-101.
- [CrossRef] [Google Scholar]
- Combined orthodontic and orthognathic surgical treatment for the correction of skeletal anterior open bite malocclusion: A systematic review on vertical stability. J Oral Maxillofac Surg. 2013;71:98-109.
- [CrossRef] [PubMed] [Google Scholar]
- Distal movement of maxillary molars in nongrowing patients with the skeletal anchorage system. Am J Orthod Dentofacial Orthop. 2006;129:723-33.
- [CrossRef] [PubMed] [Google Scholar]




