

Translate this page into:
Periodontally compromised severe skeletal Class III with open bite corrected by orthodontic camouflage using temporary anchorage devices

*Corresponding author: Adith Venugopal, Senior Lecturer, Section of Orthodontics, University of Puthisastra, Phnom Penh, Cambodia. avgorthodontics@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Venugopal A, Srirengalakshmi M, Marya A, Manzano P. Periodontally compromised severe skeletal Class III with open bite corrected by orthodontic camouflage using temporary anchorage devices. APOS Trends Orthod 2020;10(4):253-8.
Abstract
A variety of treatment options may be implemented on a Class III malocclusion associated with skeletal discrepancy ranging from functional orthopedics at an early age to orthognathic surgery in adults. In the current scenario, many Class III malocclusion patients are referred for orthognathic surgery without even considering the options of an orthodontic camouflage, as orthodontists do not want to burden themselves with the tedious treatment planning and risks involved with treating such cases. This case report describes a 27-year-old female diagnosed with a skeletal Class III malocclusion, severe open bite, and periodontally compromised dentition. Although orthognathic surgery was proposed as the best treatment modality, it was denied by the patient due to financial and psychological constraints. She was treated with mild upper arch expansion using archwires and upper premolar intrusion using temporary anchorage devices (TADs) alongside retraction of lower anterior teeth using TADs and intermaxillary elastics. At the end of 18 months of active treatment, a decent result was achieved with good occlusion and facial esthetics. Post-treatment results showed an improved profile and Class I canine relationships, with optimal overjet and overbite. The anterior open bite was corrected, and the overall facial balance was greatly improved. Extraoral photographs displayed a relaxed lip closure and an esthetic smile meeting the patient’s expectations. Two-year follow-up records demonstrated a stable occlusion and optimal facial esthetics.
Keywords
Class III
Orthodontic camouflage
Temporary anchorage devices
Open bite

INTRODUCTION
Class III malocclusion associated with a skeletal discrepancy is always a challenging issue in the realm of orthodontics. The facial profile, esthetics, and severity of the discrepancy could very often have a negative psychological impact on the patient as well have a functional impact on the craniofacial system.[1] A variety of treatment options ranging from functional orthopedics at an early age to orthognathic surgery in adults may be implemented. As an alternative, an orthodontic camouflage may be performed on certain patients to correct the occlusal discrepancy and bring about certain favorable changes in the facial esthetics.[2]
CASE HISTORY AND DIAGNOSIS
A 27-year-old female patient presented to our office with a complaint of a protruding lower jaw, a huge gap between the upper and lower teeth, inability to chew with her front teeth, mobile teeth, and non-coincident midlines. On clinical examination, she showed a severe concave profile with a vertical growth pattern. The patient’s parents presented with features of a skeletal Class III as well [Figure 1].

- Pre-treatment facial and intraoral photographs. A 27-year-old female with severe skeletal Class III discrepancy and severe anterior open bite before treatment.
Clinical intraoral examination revealed an anterior open bite of 6 mm, overjet of −2 mm with projected mandibular and maxillary incisors, Class III canines on the left, and Class II canines on the right. She was missing both lower first molars with a unilateral crossbite on the right posterior region. Upper curve of Spee was +5 mm and lower dentition had generalized spaces [Figure 1]. Grade 2 mobility was noticed in the lower anterior teeth region and lower posteriors exhibited Grade 1 mobility.
Lateral cephalogram showed a Class III jaw-base relationship (ANB = −6.34°) with a retrognathic maxilla (SNA, 78.7°) and prognathic mandible (SNB, 85°). Radiographic evaluation also revealed a very steep mandibular plane angle (Frankfort mandibular plane angle [FMA], 31.74°) with labially inclined upper incisors (U1-SN, 119.09°) and lingually inclined lower incisors (incisor mandibular plane angle [IMPA], 75.70°). Reduced bone levels were seen throughout the dentition but more prominent in the lower anterior area. Tooth number #16, #34, and #47 had undergone prior root canal therapy [Figure 1 and Table 1].
| Pre-treatment | Post-treatment | |
|---|---|---|
| SNA | 78.73 | 77.84° |
| SNB | 85.08 | 84.02° |
| ANB | −6.34 | −6.18° |
| FMIA | 72.56° | 74.02° |
| FMA | 31.74° | 33.96° |
| IMPA | 75.70° | 72.02° |
| U1-SN | 119.09° | 107.78° |
| E LINE-LOWER LIP | 6.30 mm | 3.96 mm |
FMIA: Frankfurt mandibular incisal angle, FMA: Frankfurt mandibular plane angle, IMPA: Incisor mandibular plane angle
Treatment objectives
The treatment objectives were to correct the severe anterior open bite, correct the anterior and posterior crossbite, establish positive overjet and overbite, achieve Class I canine relationships, close all residual spaces, and achieve a pleasant profile.
Treatment alternatives
Due to the severe Class III skeletal deformity and open bite, orthognathic surgery was the first treatment option. This option was discussed in detail with the patient, but the patient refused any surgical intervention due to monetary and psychological constraints.
The second treatment option was to consider orthodontic camouflage. Temporary anchorage devices (TADs) were to be placed on the upper posterior region to intrude the upper posterior teeth to alleviate the severe open bite. Very low forces would be used to level the lower arch and derotate the teeth. Furthermore, TADs were to be placed on the lower arch to retract the lower dentition into the space gained after arch consolidation.
After carefully considering all treatment options, the second plan was finalized. The final plan was explained to the patient and it was repeatedly emphasized that this would just be a camouflage treatment and perfect results could be obtained only by orthognathic surgery.
On initial evaluation, it was noticed that the patient had generalized bone loss on the upper and lower arch with Grade 2 mobility on the lower anterior. Hence, the patient was referred to the periodontist for a deep scaling and further evaluation before starting with fixed appliance therapy.
Treatment progress
This case was treated using 0.022” by 0.028” slot pre-adjusted edgewise appliances with MBT prescription. Due to poor periodontal conditions, it was decided to use two archwires on the lower arch for rotation control and alignment. A regular 0.014’’ thermal Ni–Ti wire was used on marginally aligned and already well-aligned teeth, but a 0.014” SS with multiloops was used for heavily rotated teeth to control the load deflection and deliver controlled forces [Figure 2a].

- (a) Progress pictures from leveling and alignment. ( b) Progress pictures from closure of open bite. ( c) Progress pictures from space closure. ( d) Progress pictures from finishing and midline approximation.
CORRECTION OF OPEN BITE
TADs of dimensions 1.6 mm × 8 mm were inserted between the upper second premolar and first molar bilaterally and an intrusive force was applied from the TADs to the archwire. Once sufficient intrusion was achieved on the molars, the TADs were repositioned between the upper first and second premolars bilaterally as the curve of Spee and preliminary premature contact was at this region. The intrusive force was used through 5 months as the wires on the upper arch transitioned through 0. 016” × 0.025” Ni–Ti, 0. 017” × 0.025” SS, and 0.019” × 0.025” SS. Once sufficient intrusion was achieved at the premolar area, the open bite was corrected [Figure 2b-d].
SPACE CLOSURE
Once the lower arch was leveled, 0.018” × 0.025” SS with hooks on the wire between lower lateral incisors and canines was placed along with a TAD sized 1.8 mm × 10 mm on the buccal shelf on the 4th quadrant. The lower midline was off to the left by more than 4 mm. Initially, a unilateral force was applied from the mini screw to the right lower hook on the archwire to correct the midline. Subsequently, long interarch elastics were used to retract as well as correct the midlines. Class III elastics with a horizontal vector were used from the upper second molars to lower anterior hooks. Midline elastics, 1/4 3.5 Oz were applied toward the end from the tooth number #13 to the left lower hook on the wire. Since the lower TAD failed, it was repositioned to between tooth number #44 and #45 and a simultaneous retraction force using power chain was used on the right side along with the inter maxillary Class III elastics that were already being used [Figure 2c].
0.019” × 0.025” Ni–Ti with Kobayashi hooks on tooth number #12 and #32 along with midline elastics (3/16, 3.5Oz) was used to approximate the midlines. Class I canines, ideal overjet, and overbite were achieved in about 18 months. Bone levels remained mostly unchanged throughout the dentition post-treatment [Figure 2d]. Wrap-around retainers were fabricated and provided to the patient for full-time wear till instructed otherwise.
TREATMENT RESULTS
Post-treatment results showed an improved profile and Class I canine relationships, with optimal overjet and overbite. The anterior open bite was corrected, and the overall facial balance was greatly improved. Extraoral photographs displayed a relaxed lip closure and an esthetic smile meeting the patient’s expectations. The post-treatment panoramic radiograph demonstrated proper root parallelism with some apical resorption [Figure 3].

- Post-treatment facial and intraoral photographs patient after 18 months of treatment.
Maxillary and mandibular cephalometric superimpositions confirmed clockwise rotation of the maxillary occlusal plane, slight steepening of the mandibular plane (FMA, 33.96°), intrusion of the upper posterior segment, slight extrusion and uprighting of the upper anteriors (U1-SN, 107.78°), and retraction of the lower incisors (IMPA, 72.02°) with marginal steepening of the mandibular plane by 2° (FMA, 33.96°) [Figure 4 and Table 1]. Two-year follow-up records demonstrated a stable occlusion and optimal facial esthetics [Figure 5].
DISCUSSION
In the case described, the patient presented with a complex skeletal and dental Class III discrepancy. In spite of being informed about the benefits of combined orthodontic surgical treatment, she and her parents opted for orthodontic camouflage [Figure 1 and Table 1]. Although surgical orthodontic treatment such as maxillomandibular osteotomy is usually indicated in severe skeletal open bite cases, patients do not readily accept surgical orthodontics due to the surgical invasion and accompanying risks.[3]
An important factor which complicated the treatment planning was the periodontal condition of the patient with <50% bone support on most of her teeth [Figure 1]. The treatment had to be planned in such a way that the bone levels were to be maintained to the pre-levels and not further deteriorated.
A very deep curve of Spee on the upper arch caused premature contacts of the upper posteriors, especially premolars with the lower counterparts, leading to the severe open bite. The upper posteriors were intruded with minimum forces from the TADs placed in the upper posterior region to the archwire directly to minimize the intrusive forces on the teeth and to distribute the intrusive forces more evenly. No transpalatal arch was used as the slight buccal tipping would alleviate the posterior crossbite during intrusion [Figure 2b].
The advantages of using TADs as anchorage, in contrast to extraoral appliances are that the patient compliance is not necessary and less undesirable reciprocal force occurs with tooth movement.[4] However, molar intrusion in adults is difficult and when anterior open bite patients are treated by the conventional mechanics, using intermaxillary box elastics, and multiloop edgewise archwires, it is not molar intrusion, but anterior tooth extrusion that frequently results. This yields poor esthetics, functionality, and stability.[5]
Buccal shelf implants were placed on the lower arch instead of the conventional interradicular implants as the interradicular bone levels were very low. Spaces were consolidated and midlines were approximated as much as possible before retraction [Figure 2c and d].
To summarize, the treatment was performed with mild expansion of the maxillary arch with regular archwires and slight buccal tipping of posterior teeth while intruding them. Low force using TADs and interarch elastics was used on the mandibular arch, with the purpose of retracting the lower anterior, correcting the Class III malocclusion, and establishing adequate intercuspation.
In cases of skeletal Class III open bite, counterclockwise rotation of the mandible by molar intrusion may increase the protrusion of the chin, resulting in deterioration of the facial profile. Therefore, molar intrusion can be inappropriate in such cases.[3] Although the present patient was a case of skeletal Class III, the facial profile was carefully monitored at every appointment so as to not deteriorate it further [Table 1 and Figure 4].
With the correction of the severe anterior open bite, and retraction of mandibular incisors, there was a significant improvement in the facial esthetics [Figure 3]. It was paramount to advise the patient to use the retainer provided regularly to prevent relapse after active treatment. There was a possibility of relapse even if the patient practiced strict retainer wear. Hence, regular follow-ups were recommended as a must to avoid chances of relapse.
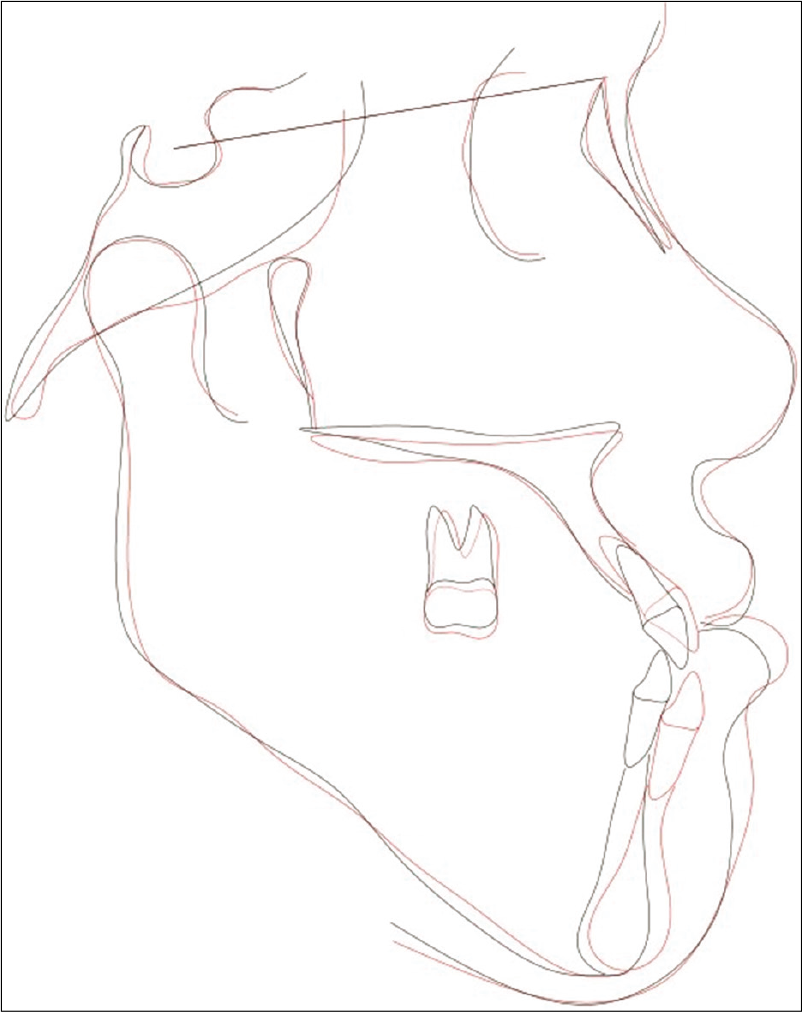
- Superimposition of pre- and post-treatment cephalometric tracings cephalometric superimpositions showing clockwise rotation of the maxillary occlusal plane, slight steepening of the mandibular plane, intrusion of the upper posterior segment, slight extrusion and uprighting of the upper anterior, and retraction of the lower incisors with marginal steepening of the mandibular plane.

- Two-year follow-up records.
CONCLUSION
Orthodontic camouflage proved to be a good substitute for orthognathic surgery for this patient. All the treatment objectives, namely, correcting the severe anterior open bite, correcting the anterior and posterior crossbite, establishing positive overjet and overbite, not further deteriorating the already compromised periodontium, and providing the patient with a pleasant profile were all achieved by the use of good biomechanics, patient compliance, and continuous monitoring.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Orthodontic-surgical treatment of class III malocclusion with mandibular asymmetry. Braz Dent J. 2011;22:151-6.
- [CrossRef] [PubMed] [Google Scholar]
- Vertical control in the class III compensatory treatment. Dental Press J Orthod. 2013;18:141-59.
- [CrossRef] [PubMed] [Google Scholar]
- Skeletal class lll severe openbite treatment using implant anchorage. Angle Orthod. 2008;78:157-66.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical outcome of mini-screws used as orthodontic anchorage. Clin Implant Dent Relat Res. 2008;10:174-80.
- [CrossRef] [PubMed] [Google Scholar]
- A simplified approach to true molar intrusion. Head Face Med. 2012;8:30.
- [CrossRef] [PubMed] [Google Scholar]




