

Translate this page into:
Two-phase orthodontic treatment in a unilateral cleft lip and palate patient with 1-year follow-up results
Address for Correspondence: Dr. Prashant M. Dhole, Smiles N Faces, 8, Gautam Ashish Society, Junction of VM Road and SV Road, Near Puranmal Hotel, Vile Parle West, Mumbai - 400 056, Maharashtra, India. E-mail: perfectsmilesss@gmail.com
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Treatment of a patient with cleft lip and palate can be challenging. A 10-year and 10-month-old girl presented with uneven and crowded teeth. She had unilateral cleft lip and palate on left side for which she had undergone primary lip repair and palatoplasty when she was younger. On examination, she had concave facial appearance, crossbite of upper arch with reverse overjet of 2 mm, wits appraisal of 6 mm and impacted 23. She was treated with two-phase orthodontic treatment; growth modification appliances followed by fixed mechanotherapy. Total treatment time was 5 years. 1-year follow-up shows that results have been stable with good facial aesthetics and functional occlusion.
Keywords
Rapid maxillary expansion
alveolar cleft
reverse pull headgear
unilateral cleft lip/palate

INTRODUCTION
Orthodontic treatment forms an integral part in the management of cleft patients.[1] The maintenance of orthodontic expansion followed by guidance of eruption of teeth in healthy periodontal support and achievement of acceptable facial aesthetics is the primary aim of orthodontic treatment in cleft cases. The positive changes in terms of expanded maxillary arch are challenging to retain due to the continuous contracture forces exhibited by the repaired palatal scar tissue.[2] The following case report describes the stable positive changes made by orthodontic treatment in a unilateral cleft lip and palate child 1 year after treatment.
CASE REPORT
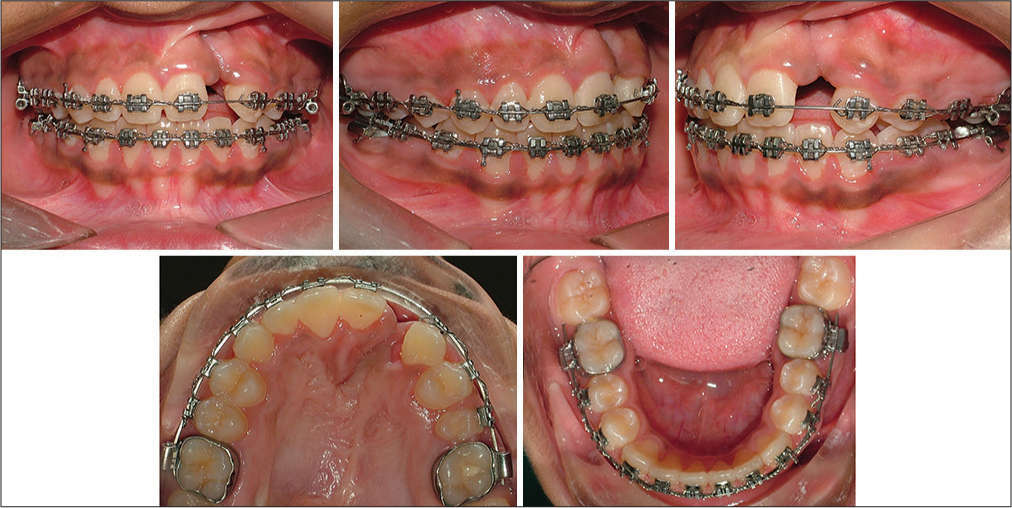
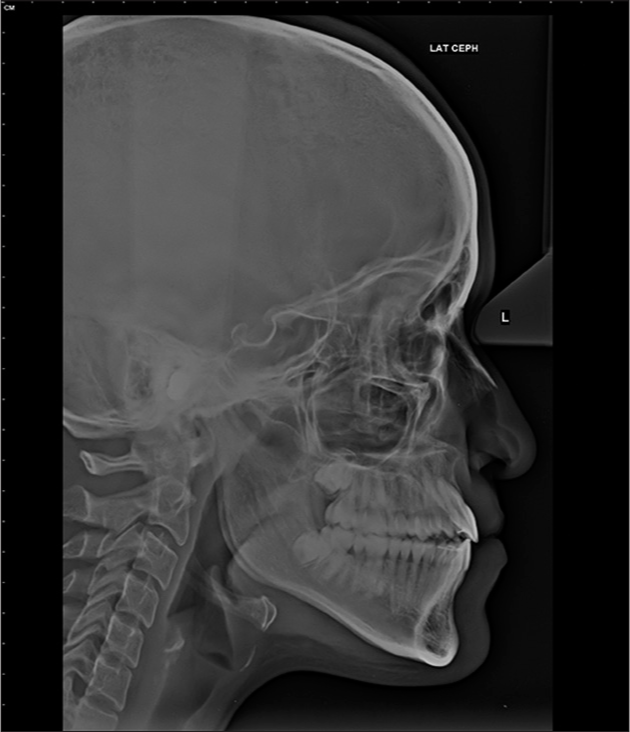
A 10-year, 10-month-old female was concerned of crowded and uneven teeth. She had a history of unilateral complete cleft lip and palate on left side for which she had received primary lip repair and palatoplasty when she was younger. The child presented a dolichofacial pattern, concave facial profile with midface deficiency and steep mandibular plane angle. Lips were incompetent and repaired cleft lip scar on left, depressed nasal bridge and alar cartilage [Figure 1]. The upper arch was V-shaped with repaired scar of cleft palate on left side. The lateral incisor region showed an absence of attached gingiva and an alveolar defect with a malformed lateral incisor in the cleft area. Lower arch was U-shaped with mild crowding. Complete crossbite of maxillary arch except upper right first deciduous molar. Class III incisor relation, reverse overjet 2 mm, overbite 2 mm, right molar in Class III relation and left molar in Class I relation [Figure 2]. Orthopantomogram [Figure 3] showed a full complement of teeth with a mesioangular upper left maxillary canine. Cephalometric examination [Figure 4 and Table 1] revealed skeletal Class III relation with retrognathic maxilla, normally placed mandible, slight vertical growth pattern, and increased lower anterior face height.

- Pretreatment extraoral photos

- Pretreatment intraoral photos

- Pretreatment orthopantomogram

- Pretreatment lateral cephalogram
| Parameters | Pretreatment | Posttreatment | 1-year follow-up |
|---|---|---|---|
| SNA | 80 | 78.5 | 80.5 |
| SNB | 82 | 80 | 82 |
| ANB | −2 | −1.5 | −1.5 |
| Wits appraisal | −6mm | −7 | −7 |
| Upper incisor to NA (mm/degree) | 2/26 | 9/36 | 9/37 |
| Lower incisor to NB (mm/degree) | 3/23 | 4/21 | 4/23 |
| Upper incisor to SN Plane | 106 | 115 | 116 |
| Lower IMPA | 90 | 83 | 83 |
| Interincisal angle | 132 | 124 | 124 |
| Lower incisor to APog line | 4 | 4 | 5 |
| Overbite | 2 | 2 | 1.5 |
| Overjet | −3 | 2 | 1.5 |
| Maxillary-mandibular plane angle | 23 | 30 | 30 |
| SN plane - mand plane | 31 | 38 | 37 |
| Upper anterior face height | 40 | 46 | 51 |
| Lower anterior face height | 55 | 64 | 70 |
| Face height ratio | 0.72 | 0.71 | 0.72 |
| Jarabak ratio | 0.67 | 0.64 | 0.64 |
| Maxillary length | 74 | 81 | 93 |
| Mandibular length | 100 | 113 | 129 |
| Lower lip to Ricketts E-plane | 0 | −1 | −1 |
| Nasolabial angle | 76 | 96 | 80 |
IMPA – Incisor to mandibular plane angle
Treatment objectives
Expansion of upper arch to correct the posterior crossbite
Obtain a positive overjet to allow unrestricted growth of maxilla
Alignment of the dentition and guide eruption of upper left lateral incisor and canine with bone grafting
Improve profile, smile aesthetics with good functional occlusion
Long-term stability of occlusion.
Treatment alternatives
Maxillary expansion, presurgical orthodontics and orthognathic surgery for maxillary advancement
Maxillary expansion, distraction osteogenesis, and comprehensive orthodontics with fixed appliances
Maxillary expansion, reverse pull headgear, and comprehensive orthodontics with fixed appliances.
The last treatment option was chosen to utilize the remaining growth potential of the patient since she was prepubertal. Furthermore, the parents and the patient wanted to avoid any surgical procedure and were ready to accept the treatment outcome understanding that she was not at the best age for orthopedic correction of maxilla.
Treatment progress
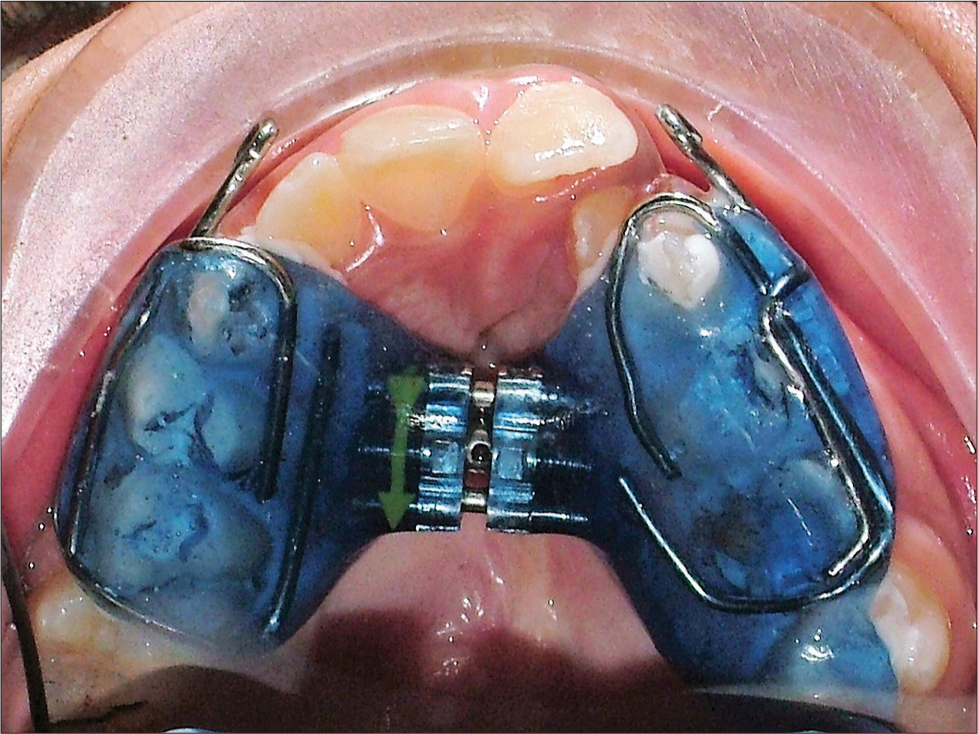
A rapid palatal expander with Jackscrew (Leone, Florence) was cemented with GC Fuji Ortho Band (GC Corporation, Tokyo, Japan) [Figure 5]. The expander was activated a quarter turn every day till overcorrection was seen, i.e., palatal cusps of upper posterior teeth occluding with buccal cusps of lower posterior teeth. Active expansion was continued for 30 days followed by a retention period for 6 months and the screw of the expander was obliterated with composite for the retention phase. Reverse pull headgear (Petit design, Ormco) was started after the active phase of expansion. The facemask was worn for 16 hours/day with 450 g force bilaterally. The direction of pull on maxilla was downward and forward at 30° to the occlusal plane [Figures 6-9]. An autologous iliac crest bone graft was performed by the plastic surgeon in the region of the bone defect created by the expansion. As per the surgeon’s advice, the patient was put on fixed appliances. Preadjusted edgewise 0.022 MBT (3M Unitek, Gemini) appliances were used, the wire sequence was 0.014 NiTi, 0.016 NiTi, 18 × 25 NiTi, and 19 × 25 SS [Figures 10 and 11]. Alignment of the lower arch with fixed appliances developed a reverse overjet. Thus, facemask was continued along with fixed appliances with hooks crimped to upper 19 × 25 SS in canine-premolar region. The upper left canine needed a surgical exposure due to its excessive mesial angulation. The upper left lateral incisor was extracted as it had poor crown-root ratio and poor prognosis.[3,4] A wraparound retainer in upper arch and fixed lingual bonded retainer in lower arch was given. The upper retainer had a temporary tooth replacement for upper left lateral incisor. The definitive replacement for the upper left lateral incisor will be done with an alveolar bone graft followed by dental implant after 4–6 months of the graft placement.[5]
- Phase I orthopedic treatment – transverse correction of maxilla with palatal expander
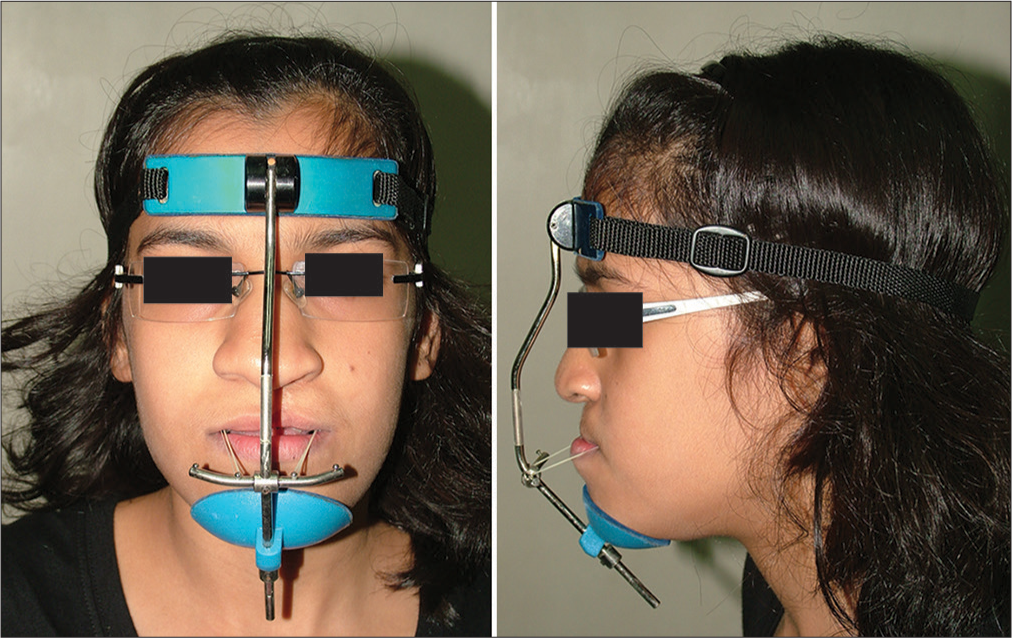
- Phase I orthopedic treatment – sagittal correction of maxilla with reverse pull headgear appliance
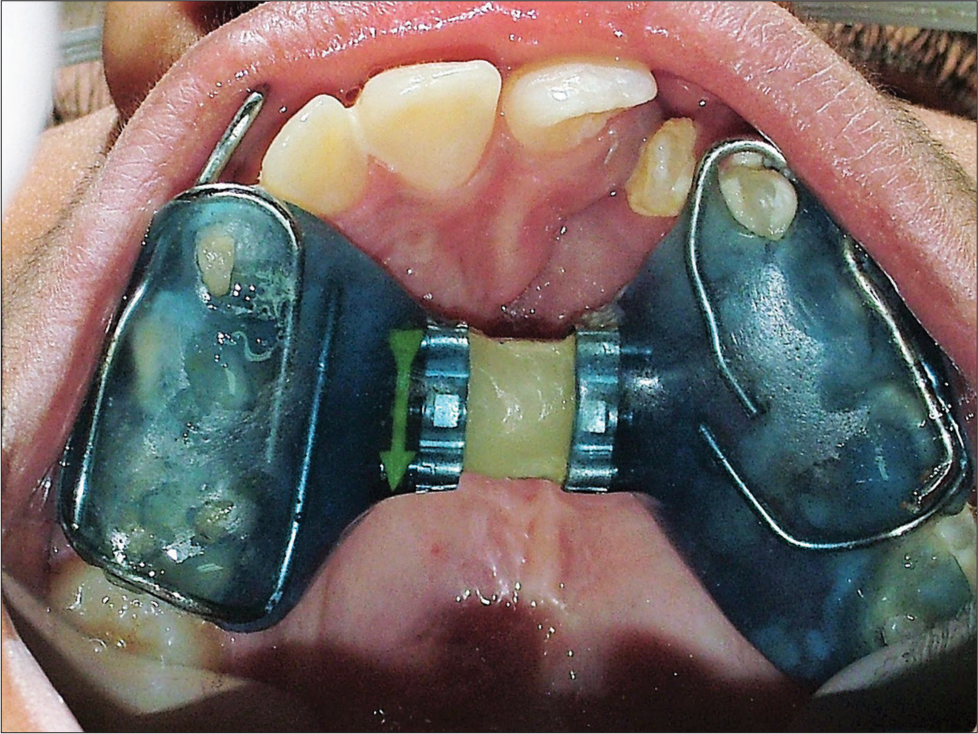
- Maxillary occlusal view after palatal expansion. The appliance acts as a retention appliance for 6 months after active expansion is completed. The screw is obliterated with composite to avoid any change

- Post Phase I - intraoral photos

- Post Phase I - extraoral photos
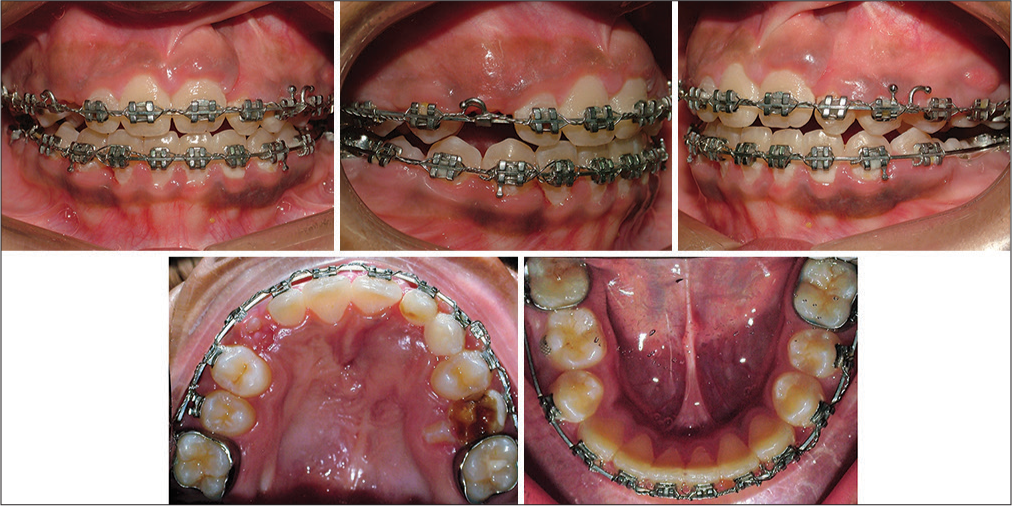
- Phase II - fixed appliances, Crimpable hooks attached to upper arch wire to continue reverse pull headgear
- Phase II - fixed appliances, 22 extracted due to poor prognosis, alignment continued
Treatment result
Phase I treatment corrected the crossbite and expanded the upper arch by 4.5 mm at canine-premolar region and 4 mm at molar region. The reverse overjet improved by 2 mm [Figures 7-9]. Posttreatment after phase II treatment exhibited Class I canine and molar relation bilaterally, positive overjet, and overbite [Figures 12-15]. 1-year follow-up shows the stability of results obtained [Figures 16-20]. A cosmetic surgery for nose revision is scheduled after she is 18 years of age.[6]

- Posttreatment intraoral photos

- Posttreatment extraoral photos

- Posttreatment orthopantomogram
- Posttreatment lateral cephalogram

- 1-year follow-up intraoral photos

- 1-year follow-up extraoral photos

- 1-year follow-up Orthopantomogram

- 1-year follow-up lateral cephalogram
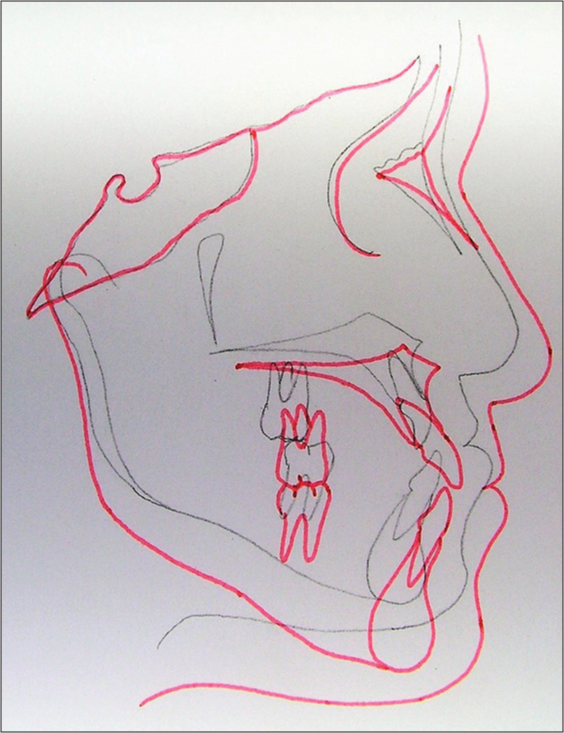
- Superimposition showing changes from pretreatment (black) to posttreatment (red)
DISCUSSION
The skeletal changes in maxilla are best in young children of 7–10 years.[7] Transverse and sagittal correction of the maxilla increases the nasal volume and improves nasal breathing, thus, creating a favorable environment for maxillary growth.[8] Expansion of maxillary arch improves its sagittal correction by reducing the resistance of the circummaxillary sutures.[9] The bone graft was done after the expansion of upper arch so that the permanent teeth adjacent to the cleft area could erupt with healthy periodontal support.
The facemask applied a downward and forward pull on maxilla, about 30° to the occlusal plane.[10] This appliance works by a combination of skeletal advancement, dental compensation, and rotation of the occlusal planes.[11,12] It helps improve the inadequate anterior vertical maxillary development and attain good vertical closure of upper and lower incisors after crossbite correction which is important for transmitting functional stimuli to maxilla thereby increasing stability in the sagittal and vertical plane.[9]
Significant overcorrection of the maxilla in the sagittal plane could not be achieved considering that the patient was 10 years, 10 months at the start of treatment.[10] The facemask with fixed appliances gave a greater component of dentoalveolar correction as indicated by upper incisor inclination in cephalometrics posttreatment [Table 1]. Greater positive overlap should have been given to avoid any relapse tendency in anteroposterior plane. However, deficiency of maxilla in the vertical plane in cleft cases prevents from extruding the incisors to great extent. The scar in the cleft palate repair area undergoes a continual contracture. Hence, to maintain the changes brought about by orthodontic treatment, rigid long-term retention should be strictly followed. The retainer should cover a large area of the palatal tissue to maintain the width of the expanded palate.[13] Cast partial retainer with complete palatal coverage or acrylic wrap around retainer would best serve the purpose. Rapid maxillary expansion after secondary alveolar bone grafting in patients with alveolar cleft can help to reduce the scar contracture.[14]
CONCLUSION
The key to success in maintaining a good functional occlusion in cleft palate patients is to house the teeth well in the bone; any overcompensation should be avoided to maintain the stability of occlusion.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Orthodontic management of patients with cleft lip and palate. APOS Trends Orthod. 2016;6:281-6.
- [CrossRef] [Google Scholar]
- Is alveolar cleft reconstruction still controversial? (Review of literature) Saudi Dent J. 2016;28:3-11.
- [CrossRef] [PubMed] [Google Scholar]
- A review of tooth formation in children with cleft lip/palate. Am J Orthod Dentofacial Orthop. 1986;90:11-8.
- [Google Scholar]
- Orthodontic space closure versus prosthetic replacement of missing upper lateral incisors in patients with bilateral cleft lip and palate. Cleft Palate Craniofac J. 2010;47:591-6.
- [CrossRef] [PubMed] [Google Scholar]
- Dental implants in cleft lip, alveolus, and palate patients: A systematic review. Int J Oral Maxillofac Implants. 2014;29:384-90.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of esthetic, functional, and quality-of-life outcome in adult cleft lip and palate patients. Cleft Palate Craniofac J. 2005;42:355-61.
- [Google Scholar]
- Cephalometric effects of face mask/expansion therapy in Class III children: A comparison of three age groups. Am J Orthod Dentofacial Orthop. 1998;113:204-12.
- [CrossRef] [Google Scholar]
- Orthopedic expansion and protraction of the maxilla in cleft palate patients – A new treatment rationale. Cleft Palate J. 1982;19:104-12.
- [CrossRef] [Google Scholar]
- Managing the developing Class III malocclusion with palatal expansion and facemask therapy. Am J Orthod Dentofacial Orthop. 2002;122:349-52.
- [Google Scholar]
- Protraction of the cleft maxilla. Eur J Orthod. 1988;10:215-22.
- [CrossRef] [PubMed] [Google Scholar]
- Protocols for late maxillary protraction in cleft lip and palate patients at childrens hospital Los Angeles. Semin Orthod. 2011;17:138-48.
- [Google Scholar]
- Evaluation of maxillary protraction therapy in CLP patients: A review of the literature. EJCO. :2.
- [Google Scholar]
- Orthodontic and prosthodontic management of an adult patient with unilateral cleft lip and palate. Indian J Dent Sci. 2016;8:159-62.
- [CrossRef] [Google Scholar]
- Rapid maxillary expansion in the deciduous and mixed dentition evaluated through posteroanterior cephalometric analysis. Am J Orthod Dentofacial Orthop. 1995;107:268-75.
- [Google Scholar]




