
Translate this page into:
Combination of expansion and orthognathic surgery in a severe hyperdivergent skeletal Class III malocclusion
Address for Correspondence: Dr. Anadha Gujar, No. 23, Flat No. TF01, Sree Sai Leela Paradise, Byrasandra Main Road, 1st Block East Jayanagar, Bengaluru - 560 011, Karnataka, India. E-mail: anadha@gmail.com
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Gujar A, Rani MS, Durgekar SG. Combination of expansion and orthognathic surgery in a severe hyperdivergent skeletal Class III malocclusion. APOS Trends Orthod 2016;6:312-8.
Abstract
Class III malocclusions with a severe hyperdivergent growth pattern are very complex to plan and treat. This case report describes the treatment of an adult with a skeletal Class III malocclusion with a midface deficiency, severe bilateral posterior crossbite, and a severe hyperdivergent growth pattern by a combination of a bonded rapid maxillary expansion appliance and surgical procedure of Le Fort I osteotomy for maxillary advancement.
Keywords
Class III malocclusion
crossbite
hyperdivergent growth pattern
Le Fort I osteotomy
midface deficiency
rapid maxillary expansion

[SHOW_RELATED_PUBMED_ARTICLES]
INTRODUCTION
Among all the malocclusions, the complexity in diagnosing and treating the cases is more in Class III malocclusions.[1] The complexity further increases if malocclusions have severe hyperdivergent growth pattern. A low prevalence of Class III malocclusions was seen in Indian population when compared to other racial groups. The prevalence was higher in Chinese and Malaysian populations which ranged from 0% to 26%.[1]
Multiple combinations of skeletal and dentoalveolar components constitute a Class III malocclusion as reported by various studies that were done to determine the morphologic variability of craniofacial complex in patients with Class III malocclusions.[2-7] Along with various other factors, skeletal Class III malocclusions can result from the maxillary deficiency or mandibular excess or a combination of both. In an adult with a skeletal Class III malocclusion, the treatment requires dentoalveolar compensation or a combined orthodontic and surgical procedures, with the aim to correct the malocclusion and improve the facial esthetics.[8,9]
The objective of this article is to present the treatment of a skeletal Class III malocclusion in a patient with a midface deficiency, severe bilateral posterior crossbite, and a severe hyperdivergent growth pattern. The dentoalveolar orthodontic compensation and surgical alternatives are discussed.
CASE REPORT
Diagnosis and etiology
A 16-year, 2-month-old girl reported with the chief complaint of an unaesthetic smile due to irregularly placed maxillary front teeth [Figure 1]. She was physically healthy and had no history of medical or dental trauma. No signs or symptoms of temporomandibular joint dysfunction were noted at the initial examination.

- Pre- and post-treatment extra- and intra-oral photographs
The extraoral clinical examination showed a concave profile caused by a midface deficiency with “sunken in” or flat appearance[10] of the upper lip along with a thin vermilion border [Figure 1]. The cheekbone contour[11] was deficient with acute nasolabial angle. There were no gross asymmetries. The intraoral examination [Figures 1 and 2] showed an angle Class III malocclusion with severe crowding of 7 mm in maxillary arch with buccally erupting maxillary canines and midline diastema. The mandibular arch showed moderate crowding of 5 mm. The anterior teeth had edge-to-edge relationship with maxillary lateral incisors in crossbite. There was bilateral posterior crossbite with retained maxillary left deciduous canine and left deciduous second molar. The arch width was reduced in premolar region by 11 mm and molar region by 9 mm as evaluated by Pont’s analysis.[12] The mandibular dental midline was shifted to the left by 2 mm.

- Pretreatment models
Cephalometrically [Figure 3], the patient had a Class III skeletal relationship (ANB angle: −10°) with maxillary retrognathism (SNA: 76°). A severe vertical growth pattern was seen (SN.GoGn: 46°). Maxillary incisors were proclined with the upper incisor at 11 mm and 37° to NA. The lower incisors were retroclined, with an IMPA of 70° and the lower incisor at 21° and 3 mm to NB, resulting in a reduced interincisal angle [Table 1]. The panoramic radiograph showed all permanent teeth including the maxillary and mandibular unerupted third molar buds [Figure 3].

- Pretreatment lateral cephalogram and orthopantomogram
| Measurement | Norm | Pretreatment | Posttreatment |
|---|---|---|---|
| Maxillary components | |||
| SNA (°) | 82 | 76 | 81 |
| A-Nperp (mm) | 2 | −9 | 3 |
| Mandibular components | |||
| SNB (°) | 80 | 80 | 80 |
| P-NPerp (mm) | −2.4 | −6 | −5 |
| Maxillomandibular relationship | |||
| ANB (°) | 2 | −5 | 1 |
| Convexity (NAP) (°) | 0 | −10 | 0 |
| Facial growth pattern | |||
| SN.GoGn (°) | 32 | 46 | 46 |
| Maxillary dentoalveolar components | |||
| Mx1.NA (°) | 22 | 37 | 21 |
| Mx1-NA (mm) | 4 | 11 | 10 |
| Mx1-PP (mm) | 30.5±2.1 | 34 | 36 |
| Mx6-PP (mm) | 26.2±2 | 29 | 28 |
| Mandibular dentoalveolar components | |||
| Md1.NB (°) | 25 | 21 | 33 |
| Md1-NB (mm) | 4 | 3 | 6 |
| Md1-GoMe (mm) | 45±2.1 | 32 | 38 |
| Md6-GoMe (mm) | 35.8±2.6 | 23 | 26 |
| IMPA (°) | 90 | 70 | 83 |
| Overjet (mm) | 2.08 | 0 | 2 |
| Overbite (mm) | 2.87 | 0 | 2 |
| Soft tissue components | |||
| Nasolabial angle (°) | 110 | 73 | 90 |
| ST convexity (°) | 12 | −4 | +6 |
| Upper 1 exposure (mm) | 2 | 4 | 3 |
| Upper lip to E (mm) | −3±1 | −3 | 1 |
| Lower lip to E (mm) | −2±1 | 1 | 2 |
Hand–wrist radiograph showed completion of circumpubertal growth [Figure 4].

- Hand–wrist radiograph
The treatment objectives
The initial treatment objective was to expand the maxillary arch and correct the transverse discrepancy. The orthodontic procedure would align the maxillary and mandibular dental arches and correct the shift in the dental midline. Our treatment objective also included achieving a Class I skeletal and dental relationship with a pleasing profile and to improve the smile arc.
Treatment alternatives
Three alternatives were presented to the patient.
Extraction of maxillary second premolars and mandibular first premolars. The two main advantages of this treatment option were the efficiency to resolve the severe arch length deficiency and correction of molar relationship by protraction of maxillary molars. Nevertheless, a four-premolar extraction treatment would not address the transverse discrepancy and the lip retrusion and might even worsen the profile
Extraction of the mandibular right central incisor. This would address the arch length deficiency in the mandibular arch. The right central incisor extraction would help in the correction of the lower midline which is shifted toward the left by 2 mm. The nonextraction treatment plan of maxillary arch would help in the correction of crowding by gaining space for it through flaring of the incisors. Class III elastics would help correct the anterior edge–to-edge bite and finish in a Class I molar relationship. However, the facial and smile esthetics would not be optimized
Nonextraction with rapid maxillary expansion (RME) using Hyrax. The arch length deficiency in maxillary arch would be resolved by transverse expansion, followed by which surgical advancement of maxilla can be done. The combined effects of RME and surgical orthodontics would correct both the transverse and anteroposterior discrepancies thus help in achieving ideal dental and skeletal relationships. This would enhance both the profile and the smile esthetics by increasing incisor display.
The nonextraction, RME, and orthognathic surgery option were adopted because it would optimize facial and smile esthetics. Cooperation and stability issues were discussed with the patient and her parents.
Treatment progress
A bonded Hyrax (tooth-borne appliance) was cemented for RME [Figure 5]. The appliance was activated by turning the screw once a day for 30 days, and after sufficient expansion of maxillary arch, the activation was stopped. The achieved expansion was confirmed by the position of maxillary molars in relation to mandibular molars, wherein the palatal cusps of the first molar were in line with buccal cusps of mandibular first molar.[13] This resulted in 10 mm arch widening at the level of maxillary first premolars and 8 mm arch widening at the level of maxillary first molars. Once the activation of RME was stopped, the appliance was locked with a ligature tie and was kept cemented for 3 months for stabilization. After the removal of bonded RME appliance [Figure 6], extractions of the retained maxillary left deciduous canine and left deciduous maxillary molar were done, and the preoperative orthodontic preparation was performed with conventional 0.022-inch MBT appliances. During the bonding of brackets on maxillary lateral incisors, the brackets were rotated by 180° which changed the torque from +10° to −10°. This inversion of the brackets assisted in labial root torque at the rectangular wire stage.[14] The tip stayed the same at 8°. Leveling and alignment began with 0.016-inch nickel–titanium (NiTi) archwires, followed by 0.019 × 0.025-inch NiTi and 0.019 × 0.02-inch stainless steel (SS) rectangular archwires. Transpalatal arch was placed for anchorage control. Decompensation of upper and lower arches was done, and a reverse overjet of 4mm was achieved [Figures 7 and 8]. Final stabilizing archwires in both arches were 0.019 × 0.025-inch SS with crimpable hooks for intermaxillary fixation. This whole presurgical orthodontic procedure took 18 months.

- Bonded rapid maxillary expansion appliance (Hyrax)

- Postremoval of bonded rapid maxillary expansion appliance

- Presurgical photographs - extraoral and intraoral

- Presurgical lateral cephalogram
Facebow transfer onto the anatomical articular was done, and a mock surgery was performed to achieve ideal Class I skeletal and dental relationship through maxillary advancement of 6 mm. A surgical splint was fabricated using cold cure acrylic. The patient was then operated with a surgical procedure of Le Fort I osteotomy with 6 mm maxillary advancement using surgical splint as a guide. Splint was left in position with intermaxillary fixation for 2 days.[15] After initial healing of 6 weeks, postsurgical orthodontics was initiated.
Postsurgically, there was posterior open bite of 1 mm at the premolars and the molars [Figure 9]. Hence, settling was done using 0.014″ SS arch wires followed by up and down finishing elastic with Class III vector for a period of 2 months.[16] Since the maxillary central incisors crowns were barrel shaped, we did composite buildup to achieve ideal tooth crown anatomy. After adequate settling was achieved, the appliance was removed [Figures 10 and 11]. The patient was placed on maxillary and mandibular 0.0125-inch twisted wire bonded onto lingual side of the incisors and canines. The total time duration for the treatment was 24 months.

- Postsurgical extra- and intra-oral photographs

- Posttreatment extra- and intra-oral photographs

- Posttreatment models
Treatment results
The facial esthetic was improved with better lip support and improved nasolabial angle [Figure 10]. The smile was enhanced. and the consonant smile arc was achieved. The concavity was corrected with improved upper lip protrusion. Intraorally, the posterior bilateral crossbite was corrected with sufficient expansion of 10 mm arch widening at the level of maxillary first premolars and 8 mm arch widening at the level of maxillary first molars. Le Fort I osteotomy with maxillary advancement helped in correcting anterior teeth relation. Ideal overjet and overbite were achieved with Class I molar and canine relationship. The midlines coincided.
The posttreatment panoramic radiograph [Figure 12] showed good overall root parallelism and lack of root resorption. The pre- and post-treatment lateral cephalographic superimpositions on the anterior cranial base along S-N plane with sella as registration point [Figures 12 and 13] showed satisfactory improvement in ANB angle by 6° and improvement in maxillary position (SNA: 81° and A-Nperp: 3 mm). A favorable profile change by 10° increase in facial profile contoural angle was seen. The mandibular plane angle remained same [Table 1].

- Posttreatment lateral cephalogram and orthopantomogram
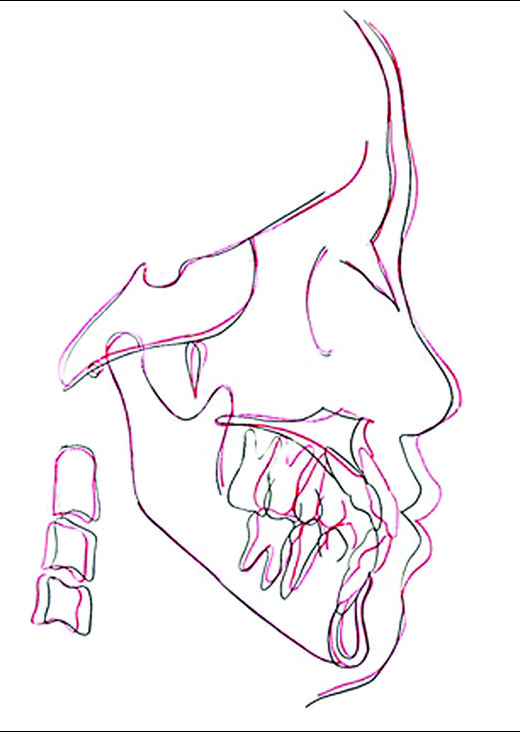
- Pre- and post-treatment lateral cephalographic superimposition
DISCUSSION
Approximately, 4% of the population has a dentofacial deformity that requires surgical-orthodontic treatment to correct out of which, Class III patients are a large proportion of those seeking it in a nongrowing patient.[10,17] Many of the Class III malocclusions are the result of mandibular prognathism; however, some Class III malocclusions are the result of a deficient maxilla, and the treatment plan of choice would be to protract the maxilla downward and forward.[18] Dentofacial deformities characterized by midfacial deficiency are difficult to manage nonsurgically, particularly when a hyperdivergent mandibular growth pattern is present.[19] According to Schudy[20-22] and Isaacson et al.,[23] the degree of inclination of the mandibular plane to the cranial base (SN) has an effect on the degree of mandibular rotation with the growth. The vertical dimension can be managed in hyperdivergent growth patterns by utilizing appliances with interocclusal acrylic such as a bonded expander.[24]
A posterior crossbite typically results from a constricted maxillary arch width. Maxillary expansion is a valid way to solve this problem.[25-29] It was very challenging to use RME appliance (Hyrax) in our patient and to maintain the changes achieved. This appliance helped in correcting bilateral crossbite. Since our patient had a severe hyperdivergent growth pattern, it was very important to avoid the extrusion of maxillary posterior teeth, which would further worsen the vertical growth pattern. Hence, we preferred to use bonded RME appliance. RME produced a significant increase in all maxillary transverse dimensions.[30]
The two most commonly cited reasons for extractions today are crowding and profile considerations.[31,32] An average increase in arch perimeter of 4.7 mm for an average molar expansion of 6.5 mm has been reported.[32] It was possible to correct the crowding present by gaining arch perimeter space through palatal expansion. The main aim of the presurgical orthodontic phase was to correct the incisor inclinations to normal to allow maximum surgical correction.[17,33]
The age of the patient plays a very important role in determining the planning and stability of orthognathic surgery. If the patient had enough growth potential, the severe malocclusion could be corrected without surgery. This depends on a careful clinical evaluation and a valid differential diagnosis followed by proper treatment planning that must include a directionally controlled growth force system.[34] Approximately, 98% of all facial growth ceases by the age of 15 years in girls and 17 or 18 years in boys.[35] Up to age 14, males and females display average yearly maxillary growth increments of 1.14 and 1.31 mm/year, respectively. After age 14, growth increments in females tend to diminish, and at a mean chronological age of 16, growth ceases.[36] The growth of maxilla completed much earlier than mandible.[37] The age of our patient, clinical examination, and radiographic evaluation showed completion of circumpubertal growth which motivated us in planning our treatment protocol. Hence, Le Fort I osteotomy with 6mm maxillary advancement was performed on our patient.
Le Fort I osteotomy resulted in secondary morphological changes in the nose, including alar flaring, as reported by many studies.[38] The nasal changes seemed to be mainly influenced by the movement of the maxilla through Le Fort I osteotomy. This had a negative effect on overall esthetics of the face in those with a wide nasal width. This was extremely important particularly for Asian population because their noses have a wider width and flat appearance.[38-41] In our patient, after Le Fort I osteotomy, nasal cinching was done to avoid alar flaring. The nasal base width widening was thus prevented.
After the surgical procedure was performed in our patient, there was posterior open bite which was closed using intermaxillary elastics. These elastics were used for 2 months till satisfactory results were obtained. 0.014 SS archwires were placed in both the arches during settling.
The pre- and post-treatment lateral cephalographic superimpositions [Figure 13] showed drastic improvement in hard and soft tissue facial profile. The maxilla achieved an ideal position. The mandibular plane angle was maintained same as that of pretreatment [Table 1]. Maintaining the basal divergence was very important since our patient had a severe hyperdiverging growth pattern.
CONCLUSION
Our results showed a satisfactory improvement in ANB angle and a pleasing external soft tissue profile was achieved. Ideal skeletal and dental relationships were obtained. The combined effect of RME and orthognathic surgery was instrumental in reestablishing the major components of a balanced smile for this patient, whose main concern was her unpleasant smile.
The optimal results achieved by our treatment despite the lateral expansion and anteroposterior positioning with nonextraction treatment along with profile considerations, helped us meet a strong challenge!
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Prevalence of angle Class III malocclusion: A systematic review and meta-analysis. Open J Epidemiol. 2012;2:75-82.
- [Google Scholar]
- Components of adult Class III malocclusion. J Oral Maxillofac Surg. 1984;42:295-305.
- [Google Scholar]
- Components of Class III malocclusion in juveniles and adolescents. Angle Orthod. 1986;56:7-30.
- [Google Scholar]
- Class III malocclusion: A cephalometric study of Saudi Arabians. Br J Orthod. 1989;16:201-6.
- [Google Scholar]
- The craniofacial morphologic structures of the adult with Class III malocclusion. Int J Adult Orthodon Orthognath Surg. 1995;10:285-93.
- [Google Scholar]
- Cephalometric evaluation of craniofacial pattern of Syrian children with Class III malocclusion. Am J Orthod Dentofacial Orthop. 2001;119:640-9.
- [Google Scholar]
- Cephalometric evaluation of dentofacial features of Class III malocclusion in adults of Mashhad, Iran. J Dent Res Dent Clin Dent Prospects. 2007;1:125-30.
- [Google Scholar]
- Extreme dentoalveolar compensation in the treatment of Class III malocclusion. Am J Orthod Dentofacial Orthop. 2005;128:787-94.
- [Google Scholar]
- Orthognathic treatment for a patient with Class III malocclusion and surgically restricted mandible. Am J Orthod Dentofacial Orthop. 2009;136:290-8.
- [Google Scholar]
- Surgical Orthodontic Treatment (1st ed). St. Louis: Mosby International Publishers; 1991. p. :429-32.
- Facial keys to orthodontic diagnosis and treatment planning–Part II. Am J Orthod Dentofacial Orthop. 1993;103:395-411.
- [Google Scholar]
- Rapid Maxillary Expansion (1st ed). Chicago, Berlin, Rio de Janeiro, Tokya: Quintessence Publishing Co.; 1981. p. :56-7.
- Systemized Orthodontic Treatment Mechanics (1st ed). Spain: Mosby International Ltd Publishers; 2001. p. :40-1.
- Contemporary Orthodontics (5th ed). St. Louis: Mosby Publishers; 2013. p. :719-20.
- The Alexander Discipline: Contemporary Concepts and Philosophies. California: Ormco Corporation Publishers; 1986. p. :159.
- Class III surgical-orthodontic treatment: A cephalometric study. Am J Orthod Dentofacial Orthop. 2006;130:300-9.
- [Google Scholar]
- Orthodontic correction of a Class III malocclusion in an adolescent patient with a bonded RPE and protraction face mask. Am J Orthod Dentofacial Orthop. 1999;116:177-83.
- [Google Scholar]
- Early treatment of skeletal Class III open bite with the tandem appliance. J Clin Orthod. 2011;45:308-16.
- [Google Scholar]
- Vertical growth versus anteroposterior growth as related to function and treatment. Angle Orthod. 1964;34:75-93.
- [Google Scholar]
- The rotation of the mandible resulting from growth: Its implications in orthodontic treatment. Angle Orthod. 1965;35:36-50.
- [Google Scholar]
- Craniofacial growth in untreated skeletal Class I subjects with low, average, and high MP-SN angles: A longitudinal study. Am J Orthod Dentofacial Orthop. 2003;124:670-8.
- [Google Scholar]
- Extreme variation in vertical facial growth and associated variation in skeletal and dental relations. Angle Orthod. 1971;41:219-29.
- [Google Scholar]
- An orthopedic approach to the treatment of Class III malocclusion in young patients. J Clin Orthod. 1987;21:598-608.
- [Google Scholar]
- Palatal expansion: Just the beginning of dentofacial orthopedics. Am J Orthod. 1970;57:219-55.
- [Google Scholar]
- Midpalatal suture opening during functional posterior cross-bite correction. Am J Orthod. 1978;74:310-3.
- [Google Scholar]
- The effect of early interceptive treatment in children with posterior cross-bite. Eur J Orthod. 1984;6:25-34.
- [Google Scholar]
- A comparison of different treatment techniques for posterior crossbite in the mixed dentition. Am J Orthod Dentofacial Orthop. 1999;116:287-300.
- [Google Scholar]
- Early intervention in the transverse dimension: Is it worth the effort? Am J Orthod Dentofacial Orthop. 2002;121:572-4.
- [Google Scholar]
- Immediate effects of rapid maxillary expansion with Haas-type and hyrax-type expanders: A randomized clinical trial. Am J Orthod Dentofacial Orthop. 2011;140:366-76.
- [Google Scholar]
- The decision to extract: Part II. Analysis of clinicians’ stated reasons for extraction. Am J Orthod Dentofacial Orthop. 1996;109:393-402.
- [Google Scholar]
- Nonextraction treatment of a skeletal Class III adolescent girl with expansion and facemask: Long-term stability. Am J Orthod Dentofacial Orthop. 2015;147:252-63.
- [Google Scholar]
- Orthodontic considerations in orthognathic surgery. Int J Adult Orthodon Orthognath Surg. 1995;10:97-107.
- [Google Scholar]
- Class II correction in a severe hyperdivergent growth pattern, bilateral open bite and oral compromise. Angle Orthod. 2005;75:870-80.
- [Google Scholar]
- Ortho-surgical treatment of patients in the growth period: At what cost? Dent Press J Orthod. 2012;17:159-77.
- [Google Scholar]
- Contemporary Orthodontics (5th ed). St. Louis: Mosby; 2013. p. :21-2.
- Nasal changes after surgical correction of skeletal Class III malocclusion in Koreans. Angle Orthod. 2008;78:427-32.
- [Google Scholar]
- International anthropometric study of facial morphology in various ethnic groups/races. J Craniofac Surg. 2005;16:615-46.
- [Google Scholar]
- The Korean American woman’s nose: An in-depth nasal photogrammatic analysis. Arch Facial Plast Surg. 2006;8:319-23.
- [Google Scholar]




